











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkAn 81-year-old, non-smoker woman presented with slowly growing and mildly painful tongue ulcers that had been first noted 3 months earlier.
Clinical examination revealed three ulcers of the tongue’s body, measuring between 0.4 and 1 cm, with a gray base and irregular, defined, slightly infiltrated borders (Fig. 1). There were no palpable lymph nodes and no teeth abnormalities.

Polymerase chain reaction testing for herpes simplex virus (HSV) and treponema pallidum h-emagglutination, venereal disease research laboratory, and human immunodeficiency virus (HIV) serologies were negative. A punch biopsy revealed ulceration, densification of collagen, vascular proliferation, and a mixed inflammatory infiltrate with lymphocytes, histiocytes, and eosinophils that extended through the striated muscle fibers (Fig. 2). A diagnosis of eosinophilic ulcer of the tongue (EUT) was made.
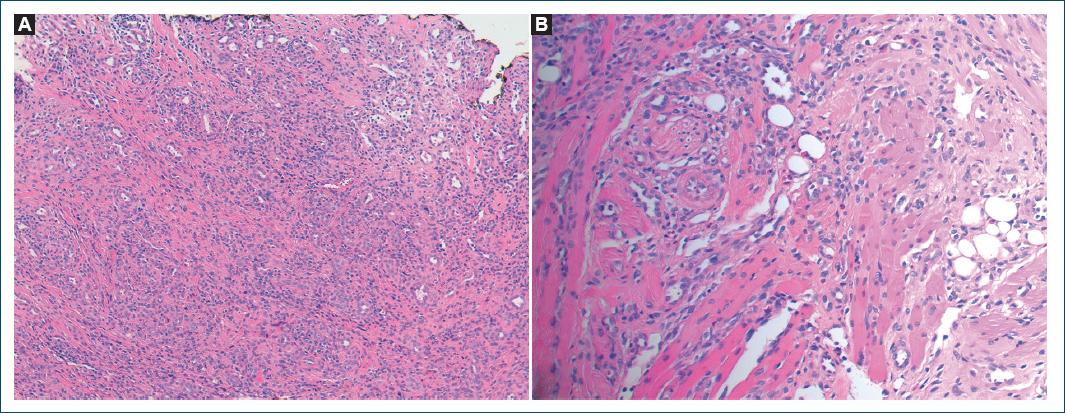
Figure 2 A: punch biopsy revealing ulceration, collagen densification, and a dense mixed infiltrate containing eosinophils (H&E, ×100); B: vascular proliferation and inflammatory infiltrate extending through striated muscle fibers (H&E, ×200).
After discussing possible treatments, a wait-and-see approach using topical lidocaine for pain management was selected. Lesion resolution occurred 4 months later, with no recurrence at 12-month follow-up.
EUT is a benign, self-limited entity, usually diagnosed during the 1st year or between the 5th and 7th decades of life1-4. Most lesions are solitary, asymptomatic, and located on the tongue1-4. Local trauma (biting, deformed teeth) is one of the drivers for EUT1-4 but is insufficient to explain lesion progression.
Differential diagnosis includes inflammatory (aphthous stomatitis and oral lichen planus), autoimmune (Behçet, pemphigus vulgaris, and systemic lupus erythematosus), infectious (HSV, syphilis, HIV), and malignant (squamous cell carcinoma) diseases.
A wait-and-see approach can be used and surgical excision, cryosurgery, and topical/intralesional corticosteroids are options for persistent lesions1-4. Recurrence is rare but removal of possible triggers (behavioral modification, dental care) is also important.

