











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Onychocryptosis consists of an inflammatory condition of the lateral nail fold resulting from the ingrowth of the lateral edge of the nail fold into the lateral groove1. It is more common in males and occurs more commonly in the toes, with the hallux being most affected2. Often associated with pain and edema, sometimes disabling, onychocryptosis is a reason for great demand in primary health care and the main cause of surgery on the nail system. Its etiology is multifactorial, involving heredity, exaggerated convexity of the nail plate, the disproportion between the width of the plate and the nail bed, chronic trauma, use of tight shoes, and inadequate nail cutting3.
Pathophysiologically, the inflammatory reaction is triggered by the penetration of a portion of the nail plate into the epidermis of the lateral groove, recognized as a foreign body, which leads to signs of edema, redness, heat, and pain and, occasionally, secondary infections of adjacent tissues with associated purulent drainage4.
Most individuals who seek health services already have a previous history of onychocryptosis and prolonged inflammation, progressing with the formation of granulation tissue and consequent chronic hypertrophy of the lateral nail fold. The prolonged condition results in a vicious cycle of swelling, pain, and infection, leading to significant morbidity, whose effect on work capacity and consequent work absenteeism has a considerable impact on the economic and social sphere, in addition to aesthetic damage5.
Onychocryptosis can be classified according to the degree of severity, as follows: 1) Grade I, due to the presence of inflammatory signs (erythema, mild edema, and pain); 2) Grade II, when inflammatory signs increase and exudate, secondary infection, and local drainage appear; and 3) Grade III, when there is the formation of granulation tissue and hypertrophy of the lateral fold of the nail6.
The literature cites different managements for onychocryptosis, either conservative, such as the use of orthoses, or surgical. In grades II and III, surgical treatment offers better efficacy and can definitively resolve onychocryptosis by definitively narrowing the nail plate or through resection of periungual soft tissues7. In the most severe cases, generally of untreated disease, the hypertrophy of the periungual soft tissues extends distally, forming a false distal nail fold. In such conditions, resection of the nail fold soft tissues is necessary when hypertrophy is significant8.
Regarding the resection of periungual soft tissues, numerous techniques can be used, such as Super U and the Vandenbos Procedure. In view of this, the present work is justified by the importance of early resolution of onychocryptosis, highlighting the effectiveness of surgical treatment in the most chronic and exuberant cases, related to nail fold hypertrophy.
Case report
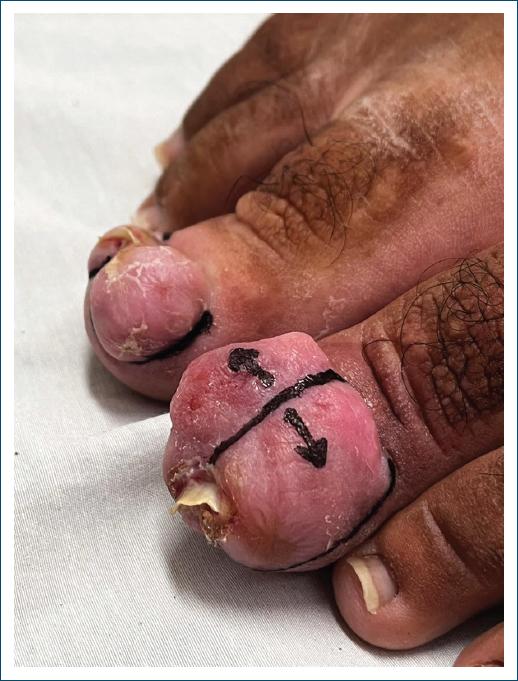
A female patient, 33 years old, attends a consultation with a dermatologist, reporting aesthetic and functional discomfort due to the growth of a tumor in both halluxes. She reported that over the last 10 years, she has been experiencing recurrent inflammation in her nail folds, resulting from attacks of undiagnosed onychocryptosis of both halluxes. The chronic inflammatory process led to exuberant hypertrophy of the nail folds, that almost completely covered the nail plate. On physical examination, the lesions appeared as slightly erythematous, firm, painless tumors, covering practically the entire nail plate of the left hallux. In the right hallux, there was significant hypertrophy of the nail fold, but without preventing visualization of the nail plate (Fig. 1). The team opted for surgical treatment on both hallux, performing the resection of all redundant tissue in the lateral, proximal and distal nail folds, associated with electrocoagulation of the corners of the nail matrix (Figs. 2 and 3). The healing of the surgical wound occurred with secondary intention. During the procedure, preparation was carried out with local antisepsis, anesthesia with lidocaine without vasoconstrictor, and a tourniquet. Initially, all redundant tissue was resected with a #15 scalpel blade, seeking to level the nail folds at the appropriate level and consequently complete exposure of the nail plates. Subsequently, the nail plates were detached from the nail folds and nail beds and removed. The surgery was completed with electrocoagulation of the corners of the nail matrix bilaterally and hemostatic suturing with a stitch anchored with 3-0 nylon (Figs. 4 and 5). Healing occurred by secondary intention with good functional results and patient satisfaction (Fig. 6).





Discussion
In the case report described, techniques similar to the Super U (left hallux) and Vandenbos Procedure (right hallux) were used, also combining the resection of redundant tissue in the proximal nail folds.
The Super U technique, developed by Brazilian dermatologist Pérez Rosa, is an invasive procedure based on the removal of all excess nail tissue, as a U-shaped band, and encompasses both the excision of the lateral nail folds and the distal nail fold9. The technique consists of anesthesia by digital block and application of a tourniquet, followed by a horizontal U-shaped incision, starting from the proximal part of one of the lateral folds and extending to the opposite proximal portion. Next, another incision is made in the same location as the first, covering the lateral, distal, and opposite lateral sulcus, ending in the same location as the first incision. The recovery time, around 2 months, is the main disadvantage of the Super U technique when applied in the most severe cases, but, even so, it does not rule it out as a choice in the presence of concomitant severe hypertrophy of both folds, given its large resolving and preventive potential for recurrences and secondary infections, which are very rare10. The Vandenbos procedure is indicated in severe cases of hypertrophy of the lateral nail folds, which cover a significant part of the nail plate. The first incision is made along the lateral nail groove from distal to proximal to junction 30 between the lateral and proximal nail folds. The second incision begins where the first ends and runs along the side of the finger, extending to its lower third. The continuity solution heals by secondary intention within a period of 4-6 weeks. The advantages of applying this technique are its easy execution, low levels of pain in the post-operative period, and the minimal risk of dystrophy of the nail plate since the procedure does not interfere with the matrix. In other words, the long recovery time is justified by the excellent functional and cosmetic results in the medium and long term11.
Conclusion
The present study addresses a case of a 33-year-old patient who, over the past 10 years, presented multiple attacks of onychocryptosis, initially with spontaneous resolution, progressing to exuberant hypertrophy of the nail folds with progressive growth and later involvement of the entire nail plate of both halluxes. The literature cites different managements for onychocryptosis, with surgical treatment being classic, financially accessible, and functional for resolving nail diseases. Such cases are essential to demonstrate the importance of an appropriate therapeutic choice and early intervention in the condition since the treatment of diseases of the nail system brings great aesthetic and functional benefits to patients.

