











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkA Caucasian 82-year-old woman was sent to the emergency department due to a rapidly growing nodule on her left shoulder (Fig. 1). The remaining examination was normal. She had no personal or family history of neoplasms and routine cancer screenings were up to date. The hypotheses of Merkel carcinoma and amelanotic melanoma were considered. Surgical excision was performed, and the histological study revealed a sebaceous carcinoma (Fig. 2). Margin enlargement and cervical-thoracic-abdominal CT were negative, and the patient has been disease free for 1-year.

Figure 1 Exophytic, well-demarcated, purplish nodule, centrally eroded, with 2 × 2.5 cm on the left shoulder.
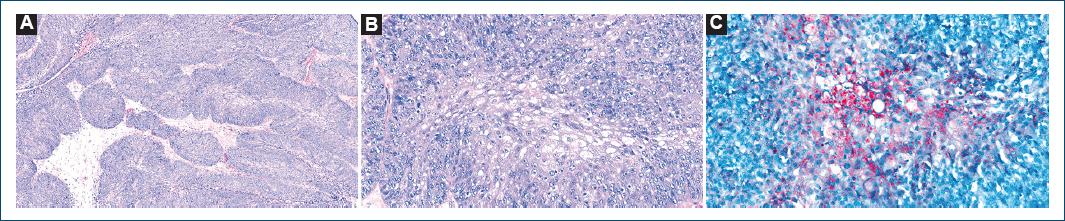
Figure 2 A: malignant epithelial neoplasm, with a solid and lobular pattern. B: consisting of atypical basaloid cells, with microvacuolated cytoplasm. C: intracellular lipid content, red oil O-positive and expression of p40, MSH2, and MSH6.
Discussion
Sebaceous carcinoma (SC) is rare, with an estimated incidence of 1-2 cases per 1,000,000 person-years1-3. It can appear anywhere with sebaceous glands, however, around 75% of cases occur in the periocular region, mainly on the eyelids. Extraocular SC is mainly located in the head and neck, where sebaceous gland density is higher and usually is less agressive1,2. CS can be sporadic or appear as a manifestation of Muir-Torre syndrome (MTS), an autosomal dominant hereditary disease resulting from mutations in DNA repair genes. As a negative immunohistochemistry to these genes is not diagnostic, a germline genetic test should be performed. In this case, the late presentation and lack of personal and family history of neoplasms indicate a low risk of MTS, therefore, a genetic study was not performed1,2. The treatment of choice for CS is excision with wide margins or Mohs micrographic surgery, but there is no consensus regarding sentinel node biopsy or adjuvant therapies1-4.
Extraocular CS is exceedingly rare, particularly outside the head and neck, but given its potential aggressiveness and possible association with MTS, it should be kept in mind.

