











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
The Global leprosy strategy 2021-20301 and the road map for Neglected Tropical Diseases (NTDs) 2021- 20302 call for accelerating action to move from leprosy control towards the goal of zero leprosy (zero disease, zero disability, zero stigma, and discrimination) through a four-pillar approach. Leprosy is listed as one of the NTDs targeted for elimination (interruption of transmission), and affected countries are urged to develop more effective and integrated country owned “zero leprosy” roadmaps. Except for yaws, whose status is presently unknown, Angola is endemic to all skin NTDs3 and was classified in 2022 by the WHO as one of the 23 global priority countries for leprosy elimination4. Better known in Angola as Hansen’s disease and commonly associated with poor socioeconomic conditions, leprosy is a complex chronic disease affecting the skin, peripheral nerves, and eyes; left untreated, it can progress to permanent impairments to the skin, nerves, face, hands and feet, lifelong disabilities, and social exclusion. Stigma and discrimination play a critical role in fostering the social marginalization of people affected by leprosy and family members, hereafter referred to as PAL&FM. As highlighted by the WHO the Global Strategy1,2, for ending leprosy transmission requires integrated approaches including actions towards zero stigma and discrimination, as well as policies and strategies to address the social determinants of the disease and the systemic roots of discrimination.
Our purpose is to document and assess the 2000- 2022 epidemiological trends towards leprosy elimination in Angola, key strengths and weaknesses of the National Leprosy Control Program (NLCP) in line with the 2021-2030 WHO Global Leprosy strategy and to explore what is known in Angola about stigma and discriminations affecting PAL&FM. Beyond achieved progress and knowledge gaps, priority actions to reactivate the disease elimination process are highlighted.
Angola is a vast middle-income Portuguese-speaking country, located on the South Atlantic coast of West Africa, between Congo and Namibia, and bordering to the east the Democratic Republic of Congo (DR Congo) and Zambia. Total area of 1,246,700 km2, divided into 18 provinces and 164 municipalities. The year 2022 basic indicators: estimated total population 35.58 million, with 46% children aged 0-14 years; annual population growth 3.1%; GDP per capita 3000, 4 USD; 2021 development index 0.586; 2018 population poverty headcount ratio below USD 2.15 a day: 31.1%; and Gini coefficient 51.3 (World Bank most recent data5).
Methods
Retrospective study of quantitative and qualitative leprosy-related data, collected between 2000 and 2022 by the NLCP/National Directorate of Public Health (DNSP)6-9. Additional information from the Ministry of Health (MOH), including dermatology services, UN reports, NGOs, and from the scant published literature on leprosy in Angola, was searched, analyzed, and incorporated as appropriate.
All new cases of leprosy were diagnosed clinically according to the WHO case definition and simplified classification10 as paucibacillary or multibacillary. Bacilloscopic examinations of slit skin smears and histopathology of biopsy material were performed in a minority of cases, due to weak capacity of public and private microbiology and histopathology services, particularly outside the more developed urban centers of Luanda, Benguela, Lubango, and Huambo.
Discrimination-related publications on leprosy were searched and consulted, in particular the report issued by Alice Cruz, UN/Special Rapporteur on the elimination of discrimination against PAL&FM, following her first visit to Angola in 202211.
Results
Leprosy work in Angola
The first leprosarium of the leprosy care network of the Swiss Phil African mission was opened in 1946 in Caluquembe, Huíla province by Bréchet, a pioneer of leprosy work in Angola. In 1965, he reported the positive results of a Dapsone (DDS) chemoprophylaxis trial in more than 700 child contacts of leprosy, recommending its use as an effective, simple, and easy preventive approach12.
The colonial Leprosy Control Program, created in 1958, operated through mobile teams and two leprosaria, one in Cazombo, Moxico province, and the other in Funda, Luanda province. By 1975, year of the country’s independence, more than 15,000 leprosy patients were reported as being treated with DDS monotherapy. Multidrug Therapy (MDT) was introduced in 1994, becoming available countrywide by 1998, freely supplied by the WHO. In 2002, all existing leprosaria were integrated by the MOH either as health posts or health centers into the national primary health care (PHC) system13.
In 1994, the NLCP initiated a collaboration with international NGOs, under the banner of the the Evangelical Solidarity Association (SOLE), working in partnership with the National Association for the Reintegration of People Affected by Leprosy (ARPAL)13.
Epidemiological trend
Administratively recorded and reported cases are presented in figure 1 (2000-2022) and table 1 (2015–2022), including data on incidence, prevalence, age, gender, MB cases, disability, and relapses14,15.
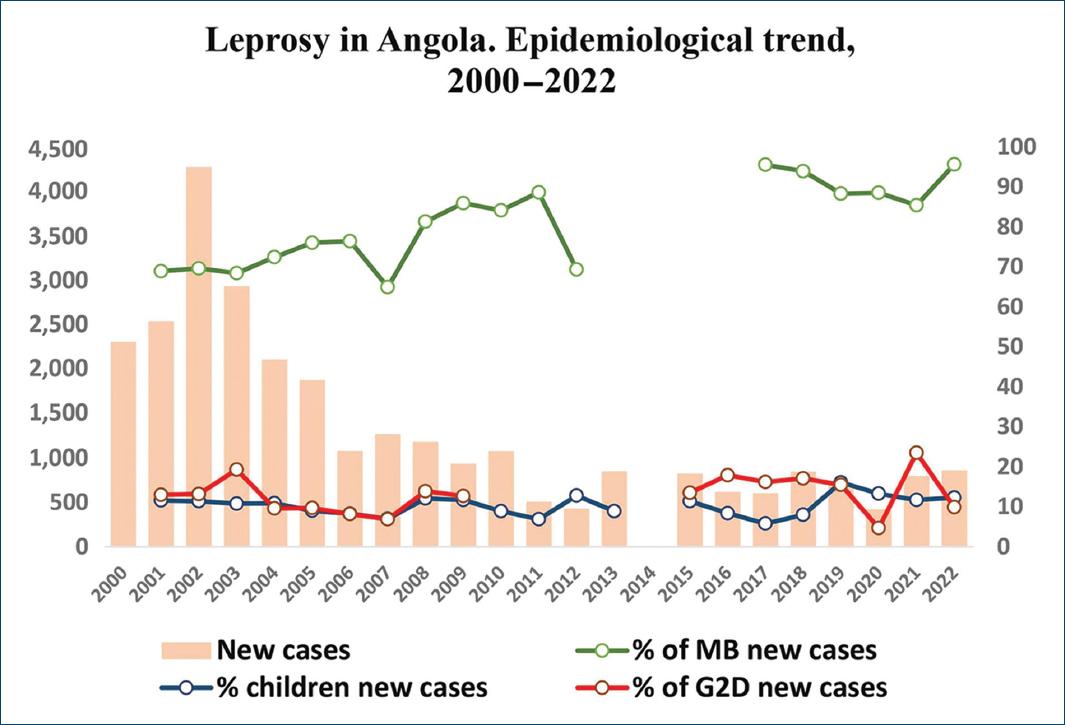
Figure 1 Leprosy in Angola: trend of newly detected cases, 2000-2022, % of children in new cases, % of Grade 2 deformities (G2D) in new cases and % of multibacilar (MB) in new cases (Source: WHO/DNSP).
Table 1 Leprosy in Angola: administratively recorded cases, 2015–2022
| Reported cases | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 |
|---|---|---|---|---|---|---|---|---|
| Population (M) | 28.1 | 29.1 | 30.2 | 31.3 | 32.3 | 33.4 | 34.5 | 35.6 |
| Newly detected cases (Rate/million pop.) | 823 (29.3) | 619 (21.2) | 605 (20.0) | 847 (27.0) | 721 (22.3) | 422 (12.7) | 797 (23.1) | 860 (24.2) |
| Registered prevalence (Rate/million pop.) | 1,173 (41.7) | 1,230 (42.3) | 1,018 (33.7) | 1,070 (34.2) | 1,070 (33.1) | 1,870 (55.9) | 1,785 (51.7) | 1,731 (48.6) |
| New child cases < 15 years (% of new cases) | 94 (11.4) | 52 (8.4) | 35 (5.8) | 68 (8.0) | 116 (16.1) | 56 (13.3) | 93 (11.7) | 106 (12.3) |
| New cases with G2D (% of new cases) | 111 (13.5) | 111 (17.9) | 98 (16.2) | 145 (17.1) | 112 (15.5) | 20 (4.7) | 187 (23.5) | 85 (9.9) |
| New child cases with G2D (% of new cases) | NA NA | NA NA | 4 (0.7) | 5 (0.6) | 0 0 | 6 (1.4) | 72 (9.0) | 9 (1.0) |
| MB new cases (% of new cases) | NA NA | NA NA | 578 (95.5) | 795 (93.9) | 637 (88.3) | 361 (85.5) | 681 (85.4) | 821 (95.6) |
| Women: new cases (% of new cases) | 420 (51.0) | 235 (37.9) | 257 (42.4) | 312 (36.8) | 197 (27.3) | 157 (37.2) | 197 (24.7) | 201 (23.4) |
| Relapses | NA | NA | NA | 2 | 107 | NA | 146 | 107 |
| Abandons | NA | NA | NA | NA | NA | NA | 202 | NA |
Source: DNSP/WHO.
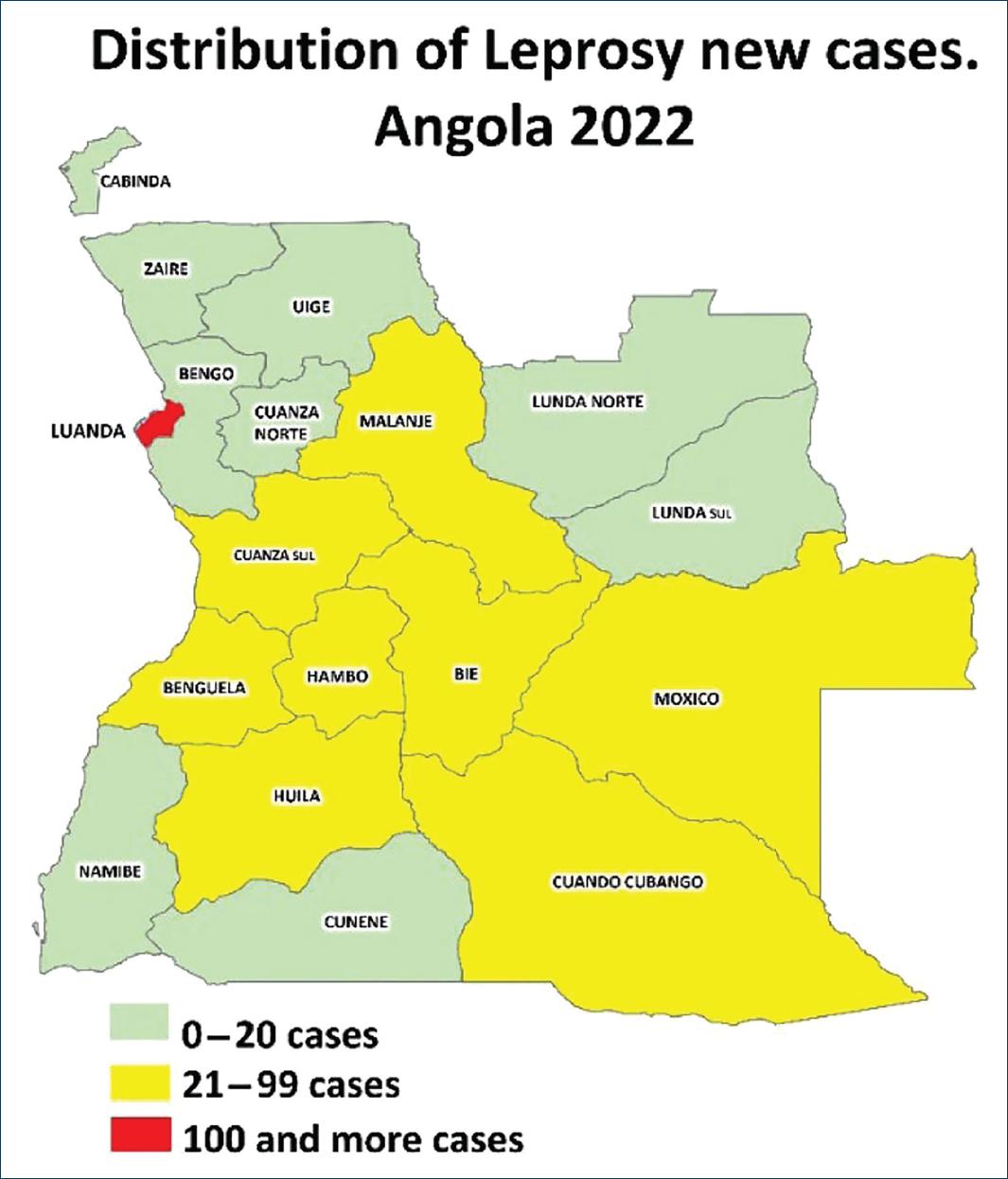
The total number of newly detected cases reached in 2002 a peak of 4,272, followed by a decline in subsequent years. In 2005, Angola registered 1,877 new cases and formally reached the status of “leprosy elimination as a public health problem”14-16, as defined by the WHO17 (i.e. national prevalence < 1 case per 10,000 population). In 2009, the total number of new cases went further down to 937, but the elevated rates of new cases in children under 15 years of age (11.7%), of new cases with grade 2 deformities (G2D; 12.7%), and of new MB cases (85.9%) were indicative of continuous disease transmission in affected communities18. From 201219, the number of annually newly detected cases began to increase again from its 431 lowest point to 605 in 2017 and 860 in 20224. In 2022, the 860 newly reported cases still included high proportions of MB cases (96,6%), pediatric cases (12,3%), cases with G2D (9,9%), high number of treatment dropouts, and relapses (107 cases). About 75% of all new cases were males and 25% females, yielding a male-to-female ratio of 3:1 (Table 1)3. MDT was administered to 85% of all newly detected cases6. The total registered prevalence was 1731; all provinces were endemic (Fig. 2), with prevalence rates below the WHO public health elimination threshold. Luanda province, enjoying better availability of health services, registered the highest number of new cases (128). More than 80% of all cases were notified in nine central provinces6,9, essentially the same as in 201113.
With WHO support, integrated case searching was carried out in 2023 in 10 municipalities across the provinces of Bengo, Kwanza-Norte, and Kwanza-Sul. This led to the detection of 57 new leprosy cases, the training of 156 technicians, and heightened community awareness about the disease20.
The National Leprosy Control Program
The NLCP is a constituent of the NTDs program, itself subordinated to the DNSP. The NLCP staff at central level has only two full-time public health specialists, assisted by a dermatologist and NTDs technical officers at provincial and municipal levels. The 2021–2025 national Leprosy and NTD strategic plans were developed along with the 2021-2030 WHO Global Leprosy Strategy1 and Global Roadmap for ending NTDs4.
In 2022, 102 health facilities, corresponding to 3.7% of the 2793 registered public health facilities, and located in 62% of the 164 municipalities, were providing leprosy diagnosis and treatment services; the rapidly growing capital city of Luanda, with an estimated population of 9 million has only two units dedicated to the care of leprosy cases, where suspected cases are referred for diagnosis and/or treatment. Data from the Américo Boavida Hospital Dermatology Service show that over recent years, the service diagnosed and subsequently referred for follow-up to the NLCP leprosy units more than 50% of the new cases detected in Luanda.
Recent leprosy program reviews6,7,20 and planning documents8,9 have identified planning and operational deficiencies, including (i) low community and health-workers awareness of the disease, (ii) deficient local diagnostic capacity and delays in referring suspected cases, (iii) weak active case finding, (iv) sporadic contact tracing and preventive chemotherapy, (v) dwindling of skilled personnel, (vi) scarcity of referral services with capacity to manage disease complications and reactions, as well as weak psychosocial care and rehabilitation services, (vii) incomplete and fragmented data, despite mandatory notification of the disease, (viii) paper-based data entries and reports leading to data omissions, mistakes, and transmission problems, and (ix) deficient funding and insufficient collaboration with other programs such as other NTDs and TB control programs. Skin-related NTDs have indeed been receiving much less funding and attention than NTDs managed primarily through mass drug administration.
On a positive note, dermatologists are increasingly working in partnership with the NLCP, expanding their action from clinical work to advocacy, training activities, and field investigations. Furthermore, the emergence of national solidarity and social reintegration networks, such as SOLE and ARPAL, though still incipient, is giving to PAL&FM greater confidence and a stronger voice in society.
The burden of stigma, discrimination, and socioeconomic disadvantage
The fourth strategic pillar of the WHO Global Leprosy Strategy 2021–20301 is the combat of stigma and the respect of human rights. In 2022, Angola set a good example of cooperation with the UN/Human Rights Council by inviting its Special Rapporteur on discrimination against PAL&FM, to explore locally the challenges and opportunities to reduce stigma and discrimination against PAL&FM21.
The general principle of nondiscrimination is established in Angola’s Constitution and legal framework, and the country is a State Party to core International Human Rights Treaties, including the Convention on the Rights of Persons with Disabilities, the Convention on the Elimination of All Forms of Discrimination against Women, and the Convention on the Rights of the Child. A key milestone was the establishment in 2020, by Presidential Decree, of a national human rights strategy and action plan incorporating equality and nondiscrimination as a pillar to warrant the respect of vulnerable groups22. Solidarity, equity, ethics, cultural identity, and gender equality are core values of the National Health Policy. Universality, quality, humanization, accountability, and intersectoral approaches are adopted basic principles for health interventions23.
While a sound legal and institutional framework appears to be in place in Angola, without laws nor regulation in force formally discriminating PAL&FMs24, field observations have revealed a lack of effective application of the formal legislation, leading to a negative impact on the enjoyment of fundamental human rights by PAL&FM. A search of official data has shown the absence of qualitative and quantitative information on incidents of discrimination, human rights violations, and on the living conditions of PAL&FM. However, the UN/SR visit report11 made reference to documented accounts of discrimination incidents faced by PAL&FM such as (i) school children being victims of neglect or even exclusion, (ii) PAL&FM suffering familial lack of attention or rejection, and (iii) PAL&FM suffering from denial or loss of employment and even of refusal to be attended or treated by health workers; loss of follow-up often related to stigma. It has also been noted that some impoverished PAL&FM are living isolated, nearby, or inside old leprosy sanatoria, considered as safe heaven. Such reports are a matter of concern and warrant further research, as already done in some other countries with endemic leprosy25.
Discussion
Challenges and perspectives towards zero-leprosy
The free availability of MDT from 1998 and the end of the prolonged internal conflict in 2002 played a catalytic role in the elimination of leprosy as a public health problem, allowing better access to health care in remote areas, with enhanced case detection and treatment. Henceforth, there was a decline of leprosy incidence and prevalence, which, however, subsided by 2012 (Fig. 1). Various factors may have impacted on the transition to a steady, slowly upward, plateau such as (i) a misinterpretation that leprosy had been eradicated in 2005, (ii) a progressive dwindling of health staff with leprosy expertise, and (iii) a reduction of national and international funding which penalized both the NLCP and the partner NGOs13.
Many existing tools, such as contact tracing, preventive chemoprophylaxis, and active case finding, have not been systematically applied, resulting in operational gaps earlier mentioned. Furthermore, the limited capacity of the healthcare system to timely diagnose leprosy has also been acting as a limiting factor. The single use of the simplified WHO classification, the frequent lack of detailed neurological examination to detect early sensory alterations, especially in cases not yet showing typical skin lesions, and the scarce facilities for bacilloscopy and/histopathology26 contribute to mistakes and/or delayed disease diagnosis.
Given the occurrence of incorrect and/or late diagnosis and underreporting, particularly in rural provinces, epidemiological data must be interpreted with caution, as real numbers likely exceed those reported. All information available in the health structures of the public health system is not collected, and the weak interconnection with the private health units compounds the problem. Furthermore, the assumption that the leprosy program has been active in the entire country does not match the reality and may lead to biased detection and prevalence rates. Hence, it becomes urgent to improve the quality of the database, including mainstreaming leprosy and other skin NTDs in a digital case-based database, such as DHIS2.
The persisting high proportion of new cases among children (12.3% in 2022; Fig. 1) is of particular concern, as this is a well-recognized indicator of recent transmission1,2. Furthermore, the elevated number (85 in 2022) and proportion (9,9%) of new cases with irreversible physical impairments (G2D) indicate that active detection, contact tracing, and timely treatment must be improved1,2. Figure 3 shows a young girl with her infected untreated father and grandmother, presenting leprosy skin lesions and visible hand deformities (G2D), as a result of long-term family contact. This is a poor, illiterate family, living in a distant village where PHC health workers did not recognize the disease. At the age of 13, due to her hand deformity, the girl was taken by her father to an orthopaedist who referred her to the dermatologist who made clinically the diagnosis of leprosy. Bacilloscopy was negative.

Figure 3 A: leprosy in a family affecting a 13-year-old girl, her father, and her grandmother. B and C: leprosy skin lesions and G2D hand deformities.
As observed in other affected countries27-29, the lower number of newly reported cases in 2020 (see Table 1) resulted from the impact of the COVID-19 pandemic, which affected the overall performance of health services, including the NLCP. It has also been reported that throughout the COVID-19 pandemic, PAL&FM have disproportionately suffered of multiple discriminations and exclusions30.
Meaningful engagement of some relevant partners is still limited. Key stakeholders such as the associations of persons affected by leprosy face difficulties to play their expected role. Community development workers (ADE- COs) could be mobilized, with appropriate training, to become more involved in the prevention and early detection of new cases. However, the focus on PHC should not lead to a lack of medical expertise for correctly diagnosing and managing such a complex and polymorphic disease. In that regard, dermatologists are a precious resource to detect cases with lesions mimicking other diseases, such as dermatophytosis (Fig. 4A), seborrheic dermatitis, pityriasis versicolor, hypochromic patches (Fig. 4B), nodules (Fig. 4C), and ulcers of other origins, as well for complex clinical diagnosis and treatments. It is worth noting that dermatologists are progressively filling the gap left by the dwindling leprologists; in 2022, Angola had 40 trained dermatologists operating in 6 provinces, all familiar with NLCP guidelines31. Medical students and family doctors are equally trained on leprosy diagnosis and management.

Stigma and discrimination are more than just other medical issues
Though stigma and discrimination have been leprosy associated features for centuries, they have only been recently recognized by UN/State members not just as medical issues but also as deeply rooted right issues. This became visible in 2017 when the Human Rights Council appointed the first UN/Special Rapporteur on leprosy to investigate to which extent affected countries implement the UN principles and guidelines for the elimination of discrimination against PAL&FM32.
Several explanations are suggested by the UN/SR regarding the lack of official data on stigma and discrimination11: (i) Such data are not systematically collected by any State institution, (ii) There have been no official records of such incidents in the courts or other types of complaints filed by PAL or their families to the Office of the Ombudsman or other relevant bodies, and (iii) The current grading system for assessing and measuring leprosy-related impairments does not record invisible psychosocial impairments and disabilities as it only focuses on measuring visible physical impairments. By design, the basic Angolan Law on Social Protection (Law No 7/04 of October 15, 2004) protects people in the formal work market but, as a matter of fact, the majority of the population is working in the informal economy and is thus being left out. Some recently established poverty relief programs could however lead to improved financial and social inclusion of vulnerable groups. A good example is the noncontributory cash transfer programs called Kwenda33 implemented by the government’s social support fund, in partnerships with the World Bank, aiming to provide financial support and access to health and education to poor and vulnerable households. This type of project appears to be a promising avenue to improve the social and financial inclusion of PAL&FM.
Women and children, either directly affected or indirectly concerned as family members of PAL, require special attention1. Women suffer the double burden of leprosy stigma and gender-based discrimination, and children should under no circumstances be denied access to education. Women also tend to assume most of the responsibility for caregiving tasks and for bearing the social and economic costs of the disease30.
While most PAL&FMs already live in poverty or extreme poverty, leprosy frequently leads to a silent worsening of their living conditions, through denial of decent education and work opportunities, loss of job, disruption of family, community, and other social ties22,30. The worsening of the health conditions may also lead to additional costs, such as transportation costs to seek treatment, additional expenses for medication to treat leprosy reactions, ulcers, and other complications, as well as expenses associated with impairments and disabilities26,30.
In the context of other skin diseases associated with stigma, discrimination, and social exclusion, it is worth mentioning the approval by Presidential Decree (N° 193/23 of October 9, 2023) of the multisectoral and interministerial 2023-2027 plan to protect and support persons with Albinism (PAPPA 2027)34, a significant step forward to provide integrated protection, care, and support to a significant vulnerable minority group.
Conclusions
Almost 20 years after the elimination of leprosy in Angola as a public health problem, the disease is still endemic in all provinces, and the elimination process appears to have stalled since about 10 years. At this pace, the country is not on track to reach the 2030 WHO leprosy goal, a challenge that leaves no room for complacency and indifference.
To do so, the priority level of leprosy transmission elimination should be repositioned and the known program gaps should be filled. This requires a combination of renewed political commitment, allocation of adequate resources at national and subnational level, strengthening of technical and financial partnerships, innovative training approaches, laboratory support, and operational research.
Strategic interventions should also include stronger disease surveillance and case-finding capacity, involving family doctors and pediatricians to enhance the detection of new cases, particularly among children. Disaggregated data by demographic, geographic, socioeconomic, and cultural variables are needed to design improved evidenced-based and integrated policies towards zero leprosy, effective program monitoring and evaluation mechanisms, appropriate budget allocations, with targets, indicators, and benchmarks35.
Intensified approaches across sectors add value. The 2022 country visit of the UN/SR on the elimination of discrimination against PAL&FMs was a key milestone to explore the social and human rights dimension of leprosy and to advocate for strengthening national policies and practical measures to ensure effective anti-discrimination strategies and a minimum standard of living for PAL&FMs12. Making use of social safety nets such as the Kwenda scheme could help affected individuals and families to benefit from a minimum of social protection33.
As stakeholders of the coalition working for the control and elimination of leprosy and other skin-related NTDs, Angolan dermatologists already play a critical role in the detection and management of the disease. Their support for a range of expanded interventions, in the context of the integrated country road map to end leprosy and other skin NTDs, should be encouraged and further developed.

