











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Amphotericin B (AmB) is a natural polyene macrolide, extracted through fermentation from the soil actinomycete Streptomyces nodosus. Although developed primarily for the treatment of life-threatening systemic fungal infections, presently the utility of AmB has extended for the management of complicated cutaneous and visceral leishmaniasis (VL). Besides, there are reports describing the use of AmB in subcutaneous mycoses, onychomycosis, and superficial fungal infections with promising outcomes1.
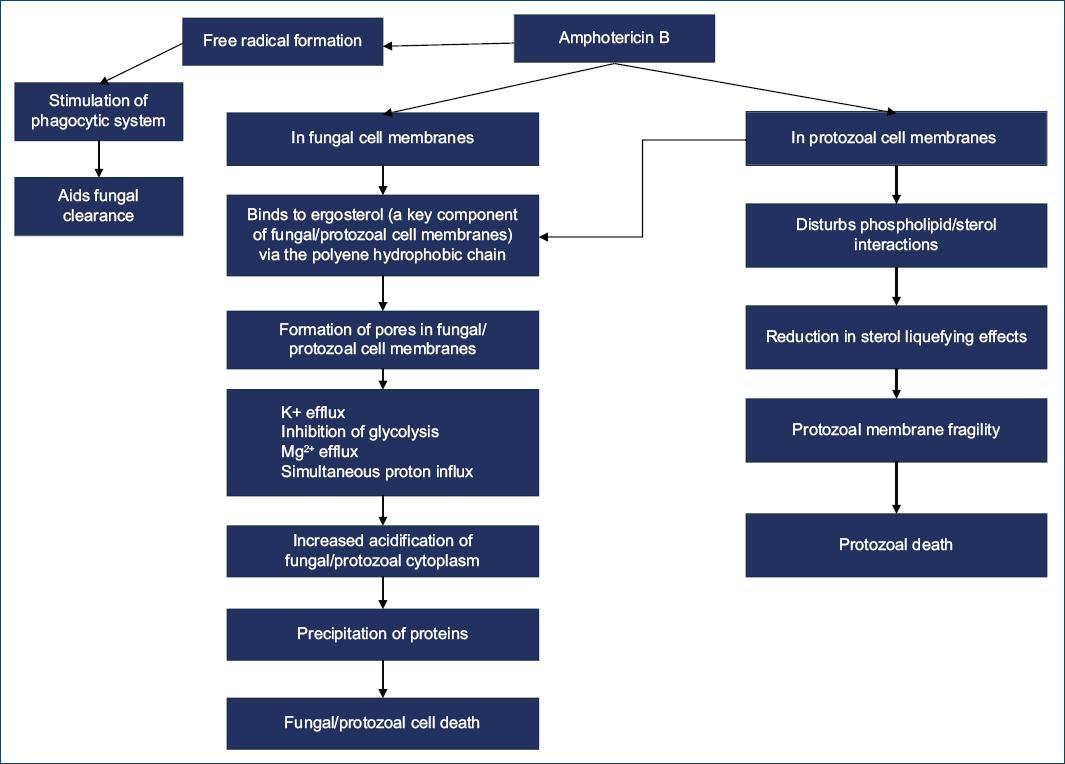
Mechanism of action
AmB causes fungal cell death mainly by binding to ergosterol of the cell membrane which leads to pore formation and ultimately fungal cell destruction, as represented in figure 1 2. In addition, for leishmaniasis, other mechanisms postulated include cholesterol sequestration in the host membrane, thereby blocking interaction of the parasite with host macrophages (mandatory for initiation and perpetuation of infection)3,4, lipid peroxidation, with subsequent protozoal destruction, antagonism of endosome-lysosome fusion5,6, apoptosis of the parasite7 and promotion of IFNγ production from natural killer cells, which helps macrophage activation6.
Clinical uses
Invasive fungal infections (IFIs)
The incidence of IFIs has increased remarkably in recent years. Comorbidities such as neutropenia, human immunodeficiency virus infection (HIV)/acquired immunodeficiency syndrome (AIDS), and cancer are often encountered in patients presenting with IFIs, with an increased predisposition for resistance to antifungal agents8-10.
AmB continues to be the reference drug in treating IFIs, essentially due to its broader mechanism of action. Due to the association of several adverse effects with the conventional formulation of AmB (d-AmB), various newer AmB preparations have now been developed with an effort to reduce the toxic effects of d-AmB. Newer lipid-based formulations with a favorable lipid solubility of AmB include liposomal AmB (L-AmB), AmB colloid dispersion (ABCD), and AmB lipid complex (ABLC) (Table 1)8,11-18. Main IFIs where AmB is utilized are cryptococcal meningitis, candidemia, and invasive candidiasis (namely, in neutropenic patients or chronic disseminated candidiasis), neonatal candidiasis, and invasive aspergillosis19-22. The dose of d-AmB for IFIs is 1 mg/kg/day, which is administered for a period of 5-7 days, followed by transition to other anti-fungal drugs1,19. In addition, a single 10 mg/kg dose of d-AmB was found to be equally effective20. Liposomal AmB is given at 3-5 mg/kg/day and holds efficacy similar to voriconazole for invasive aspergillosis21,22.
Table 1 Salient points related to the lipid formulations of amphotericin B
| Feature evaluated | Liposomal AmB | AmB colloid dispersion | AmB lipid complex |
|---|---|---|---|
| Components | Unilamellar lipid structure AmB complexed with 3 major components, soy phosphatidylcholine, distearoylphosphatidylglycerol and cholesterol (2:1:1:0.8) | Disc-like lipid structure AmB and cholesteryl sulfate (1:1) | Ribbon-like lipid structure AmB complexed with L-α-dimyristoyl-phosphatidyl glycerol (1:7:3) |
| Year of approval by the US-FDA | 1977 | 1996 | 1995 |
| Standard dose | 3 mg/kg/day | 3-4 mg/kg/day | 5 mg/kg/day |
| Pharmacokinetics | Extraordinarily high serum concentrations T1/2 of 152 h < 10% is excreted unchanged in the urine and feces Small particle size Substantial escape from the MPS Higher Cmax and higher AUC |
Lower serum levels Larger size/poor dissociation Rapidly engulfed by MPS Lower Cmax and AUC |
Low serum levels Higher organ distribution (lungs) Larger molecule Engulfed by MPS Lower Cmax, low AUC, high volume distribution |
MPS: macrophage phagocytic system; AUC: area under the curve; AmB: amphotericin B; US-FDA: United States Food and Drug Administration.
Cutaneous mucormycosis (CM)
CM is an emerging mycotic infection commonly encountered in immunosuppressed individuals and patients with uncontrolled diabetes. It often occurs following direct inoculation through trauma with a non-specific presentation closely mimicking other dermatologic disorders23. Although d-AmB is the therapy of choice, lipid formulations are often used, due to their favorable toxicity profile24. In fact, studies reveal AmB as the most active drug against mucorales, with minimum inhibitory concentrations (MICs) of ≤ 1 mg/mL in majority of tested strains25. Apart from AmB therapy, which should be initiated within 5 days of diagnosis, surgical debridement and control of underlying immunosuppression are equally important.
Recommended dosing of d-AmB is 1-1.5 mg/kg/day or 0.5-1 mg/kg/day, respectively, for immunosuppressed or immunocompetent patients with CM. L-AmB is dosed at 5-10 mg/kg/day and ABLC is administered at 5-7.5 mg/kg/day in both immunosuppressed and immunocompetent individuals26. Treatment duration is still not determined, with some authors suggesting to continue therapy till clinical/radiological resolution, and others recommending a treatment period of 6-8 weeks26,27.
Interestingly, successful use of L-AmB has been documented in an extremely pre-term infant (< 28 weeks) who developed primary CM along with polymicrobial sepsis, within the first 10 days of life. L-AmB given for a period of 4 weeks resulted in spontaneous sloughing of the fungal eschar and no long-term sequelae28.
Furthermore, the use of topical AmB, both as combination and monotherapy for CM has been described29,30. In a 6-month-old infant with leukemia, severe necrotizing skin and soft-tissue mucormycosis of the chest wall was treated with systemic L-AmB, local wound control, surgical resection, and topical AmB, which was successfully added due to incomplete response to systemic L-AmB alone29.
AmB 3% cream was found to be highly effective in treating vaginal mucormycosis in a 56-year-old woman, with a once-daily application schedule for 3 weeks, but due to relapse after therapy cessation, AmB cream was restarted for another month and gradually tapered as an alternate day schedule for 2 months with complete clinical and mycological cure (MC), even at 12 months of follow-up30.
Chromoblastomycosis
Chromoblastomycosis represents a cutaneous/subcutaneous mycotic infection caused by a group of dematiaceous (black) fungi and occurs following traumatic skin inoculation, with the majority of lesions involving the lower extremities of outdoor workers31.
At present, existing trials regarding its treatment are limited; with oral itraconazole and terbinafine constituting the primary therapeutic pillars for chromoblastomycosis. Unfortunately, cure rates are low and relapse rates are high32.
AmB has been used in two reports for chromoblastomycosis33,34. In the first report, intravenous L-AmB for 1 month was helpful in attaining MC in a 37-year-old woman with chromoblastomycosis of the right breast. Following this, the patient was maintained on itraconazole (200 mg/day) and 5-flucytosine (4 g/day) for 12 months with no relapse33. In the second report, intralesional AmB (obtained by dissolving 25 mg of AmB in 20 mL of sterilized water and 5 mL of 2% lidocaine solution to make 1 mg/mL of AmB) given once weekly for 19 weeks along with 500 mg/day of oral terbinafine was successful in attaining clinical cure of chromoblastomycosis in a 75-year-old farmer who had the disease for 12 years, and was unresponsive to oral itraconazole, cryotherapy, and complete surgical excision34.
Despite these promising reports, more robust clinical data are needed in relation to the precise dosing schedule of AmB and its combination with other antifungals for treating chromoblastomycosis.
Blastomycosis
Blastomycosis is a chronic granulomatous and suppurative systemic mycosis primarily affecting the lungs; with involvement of the skin, bones, and central nervous system (CNS) in disseminated forms35. Although itraconazole is employed as the first-line drug for most cases, AmB proves to be valuable in widespread and disseminated forms of the disease. Furthermore, in cases unresponsive to itraconazole, AmB has demonstrated efficacy36.
Histoplasmosis
Histoplasmosis is a highly infectious mycosis caused by Histoplasma capsulatum that primarily affects the lungs. Although most pulmonary lesions heal spontaneously in immunocompetent hosts, in immunosuppressed individuals this progresses to disseminated histoplasmosis, with mucocutaneous involvement serving as an important diagnostic clue37. Regimen of AmB in the management of histoplasmosis consists of 0.7 mg/kg/day for d-AmB, 3-5 mg/kg/day for liposomal AmB; that may need to be continued for a period of 2-4 months38,39.
Recently, in a randomized controlled trial, a single high dose of L-AmB (10 mg/kg) in HIV/AIDS-related disseminated histoplasmosis was documented to be non-inferior to the standard therapy with AmB. Besides, a single induction dose would considerably reduce drug acquisition costs (almost 4-fold) and help in simplifying treatment39. However, more robust data are needed to confirm these findings.
Cutaneous fusariosis
Fusariosis is a complex infection caused by the pathogenic fungus Fusarium spp., which is commonly found in soil and water, and transmitted to humans following traumatic inoculation. Based on the host’s immune status, the clinical presentation of fusariosis differs: localized and superficial symptoms confined to the skin in immunocompetent individuals, and invasive and disseminated lesions in immunosuppressed patients. Prolonged periods of neutropenia predispose to disseminated fusariosis, which is associated with high mortality40. d-AmB (1-1.5 mg/kg/day) in combination with terbinafine (250 mg TID) and subsequent intravenous L-AmB (5 mg/kg/day) has demonstrated efficacy in treating a case of disseminated infection with Fusarium oxysporum following chemotherapy for acute myelogenous leukemia41. Furthermore, in a granulocytopenic patient with myelodysplastic syndrome post-peripheral blood stem cell transplant, combination of L-AmB (3 mg/kg/day) and terbinafine (250 mg TID) showed efficacy in treating fusariosis, following failure with voriconazole42.
Interestingly, successful combination of voriconazole and AmB in disseminated fusariosis in a patient with neutropenic fever has been reported43. Although voriconazole still remains the first-line choice of fusariosis, some Fusarium species like Fusarium proliferatum have shown low susceptibility to voriconazole42. In such scenarios, AmB proves to be a valuable alternative, and if combined with other antifungals, superior outcomes can be expected.
Protothecosis
Human protothecosis is an algal infection due to the environmentally ubiquitous achlorophyllic algae, Prototheca spp. Clinically, it presents in three forms, namely, as cutaneous lesions, olecranon bursitis, and disseminated/systemic infections44. Most treatments in protothecosis are drawn from isolated case reports, limited case series, and in vitro studies.
Among the available treatments, AmB displays the best activity against Prototheca spp. For cutaneous lesions, systemic as well as topical use of AmB has been attempted45. For olecranon bursitis, intrabursal administration of AmB is suggested in patients ineligible for bursectomy46. In systemic disease, intravenous AmB (including liposomal preparations) is considered the drug of choice. The dosing is similar for invasive mycotic infections, but responses may be variable. Combination with doxycycline, fluconazole, voriconazole and itraconazole may be beneficial in recalcitrant cases47-51.
Congenital and neonatal candidiasis
Congenital candidiasis is a rare entity, manifesting within the first 6 days of life. It usually occurs following intrauterine candidal infection and may be localized, involving the skin alone, or have a generalized presentation resulting in respiratory distress, meningitis, with ultimate sepsis and death52.
Systemic treatment with AmB (0.5-1 mg/kg/day) is the preferred line of management in neonates with disseminated systemic candidiasis, respiratory distress, and/or sepsis. Lipid-associated preparations of AmB (3.5 mg/kg/day) are reserved for those cases with invasive candidiasis and severe pre-existing renal insufficiency. Further, for infections involving the CNS, 5-flucytosine (50-100 mg/kg/day) is used in combination with AmB. At present, no controlled studies have defined the exact duration of therapy; however, a minimum of 21-28 days is suggested53,54.
Genital candidiasis
Vulvovaginal candidiasis (VVC) is one of the most common infections of the female genital tract55. Topical AmB has demonstrated efficacy in the treatment of refractory VVC due to Candida glabrata and Candida krusei. In the two reports on C. glabrata VVC, AmB 100 mg plus flucytosine 1 g in Aquagel (total 8 g) was given by a vaginal applicator for 14 nights. Following completion of treatment, all patients outlined significant symptomatic improvement as well as negative cultures56,57.
In the publication on C. krusei VVC, 3% amphotericin gel (containing d-AmB with Aquagel lubricant gel and propylene glycol) was developed and administered intravaginally for 14 days. Although patient’s symptoms resolved after 1 month, vaginal cultures remained positive58.
Oral candidiasis
D-AmB oral suspension has been recommended by the IDSA to treat oral candidiasis refractory to fluconazole20.
Pityriasis versicolor (PV)
PV, a mild yet chronic superficial cutaneous mycosis caused by Malassezia yeasts, is currently treated with several topical azole compounds; the cornerstone of PV therapy59. Although never used for this indication, lipophilic properties of AmB may suggest favorable effects, as observed in a study where topical AmB 0.4% was equally effective as clotrimazole 1% in obtaining clinical and mycologic cure for PV60. However, based on this anecdotal report, no significant conclusions can be drawn.
Onychomycosis
At present, oral itraconazole and terbinafine are the recommended first-line drugs for onychomycosis61. However, due to adverse effects and concomitant drug interactions, their utility in many individuals may not be suitable, making it mandatory to consider alternative approaches to tackle these issues. In such scenarios, topical therapy might offer advantages like better site selectivity, avoidance of systemic adverse effects, and easy application at the site of fungal infection. Besides, topical antifungal agents available at present (amorolfine, ciclopirox olamine, and azoles) have proven valuable, despite their lower potencies and limited on-site penetration62.
Topical AmB in onychomycosis has recently been evaluated in two reports63,64. In the first, a topical formulation consisting of 0.3% AmB in 30% dimethyl sulfoxide (DMSO) cream (group A, n = 10) was compared with 30% DMSO cream (group B, n = 9) in non-dermatophyte onychomycosis daily for 36 weeks, with clinical cure in 70% of patients in Group A and 22% patients in Group B, and MC rates in 80% and 44.4% of patients in Group A and Group B, respectively63. In the second report, topical nano liposomal AmB 0.4% gel was utilized in 12 onychomycosis patients for a period of 12-36 weeks twice daily over the entire surface of the affected nails, including a 6 mm margin around the cuticle. At 12 weeks, 50% showed complete clinical cure (CCC), 16.66% outlined an effective clinical response and 16.66% denoted a partial clinical response. MC was observed in 50% of patients at week 12. At week 24, CCC and MC were observed in 91.66% of patients, with 8.33% delineating no response. Apart from temporary nail detachment in one patient, no other adverse events were reported. Notably, in one patient, nano-liposomal AmB induced CCC at week 12 in fluconazole-resistant onychomycosis64.
Furthermore, MICs of non-liposomal AmB are lower for Candida albicans, C. glabrata, Trichophyton rubrum, and Fusarium solani, making it a potential quasi-efficient alternative for onychomycosis, demanding lower doses and having the advantage of topical use, without any off-target systemic side effects64. Nevertheless, more studies become essential to strengthen these observations.
Dermatophytosis
At present, there are no clinical studies on the use of AmB in vivo for dermatophyte infections, although in vitro studies have demonstrated susceptibility of dermatophytes to AmB, even though with variable results. Terbinafine is considered the most effective drug against T. rubrum and T. verrucosum followed by AmB65.
In another evaluation, AmB was inferior to caspofungin and itraconazole but superior to ketoconazole and fluconazole against all dermatophytes tested66. Interestingly, Coelho et al.67, elucidated AmB to be the most superior drug against microconidia of T. rubrum and Trichophyton tonsurans in comparison to fluconazole, terbinafine, itraconazole and griseofulvin. Despite these positive findings, clinical application of this data warrants caution because in vitro susceptibility may not always translate to in vivo efficacy.
Nevertheless, topical AmB may at least in part provide a solution to the annoying issue of recalcitrant dermatophytes. However, it cannot be overlooked that AmB remains the primary drug for invasive life- threatening fungal infections, and it would be prudent to restrict its use only to very specific cases, where it is justified.
Cutaneous leishmaniasis (CL)
Leishmaniasis is a protozoal disease transmitted by sandfly vectors and is endemic in 88 countries, commonly in tropical and subtropical regions. Clinical manifestations of leishmaniasis range from aggressive cutaneous ulcers to systemic multi-organ disease (that constitute VL)68.
At present, systemic therapy for CL is only recommended in old-world CL with mucosal involvement, or patients with complicated cutaneous lesions; defined as ≥ 3 lesions, lesions with diameters > 30 mm, lesions in anatomic locations unsuitable for local treatment, and lesions refractory to local therapy69,70.
Common drugs currently employed for systemic therapy in leishmaniasis include pentavalent antimony, AmB, fluconazole, and miltefosine. No prospective clinical trials comparing the efficacy of any of these drugs for complicated CL have been conducted, with the choice of therapy relying solely on retrospective case descriptions and case series. d-AmB and lipid-bound AmB products are well-established treatments for VL71. However, in complicated CL, there is no clear consensus regarding its systemic use, as well as the optimal dosing schedule. Besides, in this scenario, L-AmB is preferable, due to reduced nephrotoxicity, and its ability to specifically target macrophages in which leishmania parasites develop72. Presently, the dosing schedule stated by the American Society of Tropical Medicine for VL is employed for this indication, and consists of intravenous L-AmB (3-4 mg/kg/day) on days 1-5, 10, 17 and then weekly until healing or a cumulative dose of 40 mg/kg is achieved73.
Besides, in uncomplicated CL, the use of intralesional and topical AmB has demonstrated propitious outcomes (Table 2)74-77. Moreover, as it is administered locally, systemic adverse effects with AmB are expected to be minimal. Although spontaneous healing of lesions may occur in uncomplicated CL, treatment is recommended to accelerate cure and reduce scar formation, especially in cosmetically important sites78.
Table 2 Studies outlining the utility of topical and intralesional amphotericin B for uncomplicated cutaneous leishmaniasis
| No. | Authors | Study type | Details | Remarks |
|---|---|---|---|---|
| 1 | Goyonlo et al.74 | Prospective study | 93 patients 79 unresponsive to intralesional meglumine antimoniate AmB deoxycholate intralesional once a week until lesion resolution 10.31 ± 5.41 injections |
Complete remission at 12 weeks 63.5% (urban leishmaniasis) 66.7% (rural leishmaniasis) 54.6% (lupoid leishmaniasis) Partial remission at 12 weeks 20.6% (urban leishmaniasis) 33.3% (rural leishmaniasis) 22.7% (lupoid leishmaniasis) No response at 12 weeks 15.9% (urban leishmaniasis) 22.7% (lupoid leishmaniasis) No recurrence (rural leishmaniasis) Recurrence < 6 months 4 patients (urban leishmaniasis) 2 patients (lupoid leishmaniasis) Recurrence at 6-12 months 2 patients (lupoid leishmaniasis) Recurrence at > 12 months 2 patients (lupoid leishmaniasis) Negligible side effects No premature discontinuation |
| 2 | Goswami et al.75 | Prospective study comparing 2 doses of intralesional AmB (2.5 mg/mL vs. 5 mg/mL) | Group A (n = 25) 2.5 mg/mL/week 8 weeks Group B (n = 25) 5 mg/mL/week 8 weeks |
At 8 weeks, Group A Complete response (72%) Partial response (20%) No response (8%) At 8 weeks, Group B Complete response (56%) Partial response (28%) No response (16%) At 12 weeks, Group A Complete response (88%) Partial response (8%) No response (4%) At 12 weeks, Group B Complete response (64%) partial response (24%) no response (12%) Side effects - pain (< 30 min) at injection site - no treatment discontinuation |
| 3 | Layegh et al.76 | Comparative clinical trial topical liposomal AmB versus intralesional meglumine antimonate | n = 39 patients: topical liposomal AmB (3-7 drops twice daily-8 weeks) + 11 not adherent n = 37 intralesional meglumine antimoniate weekly (max. 2 mL-8 weeks) + 23 not adherent | At 8 weeks, clinical cure AmB group (56.4%), Meglumine antimoniate (67.6%). Besides, at 6 months of follow–up, no recurrence of lesions was reported Limited side effects in both groups |
| 4 | López et al.77 | Open-label, randomized non-comparative phase Ib/II clinical trial Topical 3% AmB cream |
80 patients uncomplicated cutaneous leishmaniasis Group A (n = 40) 3% AmB cream TID – 4 weeks Group B (n = 40) 3% AmB cream BID – 4 weeks |
Definite cure at 90 days Group A (39.4%) Group B 35.3% No adverse events |
AmB: amphotericin B.
Post-Kalazar dermal leishmaniasis (PKDL)
PKDL is a complication of VL characterized by macular, maculopapular, and nodular rash in a patient apparently cured, inadequately treated, or untreated for VL79. L-AmB is the second-line treatment for PKDL in patients where miltefosine is contraindicated80.
Miltefosine (2.5 mg/kg/day in children and 100 mg/day in adults) is preferred over AmB due to its oral route of administration, but it has a high cost. d-AmB (1 mg/kg for 60-80 infusions) is often associated with nausea, vomiting, fever, rigor, and other toxicities accounting for patient non-compliance81. To tackle this issue, low dose d-AmB (0.5 mg/kg/day) for 20 infusions, for 3 courses, at an interval of 15 days between each course has been attempted with promising results, including shortening the duration of hospitalization and improving tolerability82. Furthermore, L-AmB is being used for treating PKDL with lesser toxicity compared to d-AmB.
In a randomized open-label study comparing L-AmB versus miltefosine for PKDL, the final cure rate as per protocol analysis was 74.5% and 86.9% for L-AmB and miltefosine, respectively. Further, relapse of PKDL was observed in 25.5% of patients in the L-AmB group and 13% of patients belonging to the miltefosine group. Besides, no patient in both groups developed any serious adverse effect83.
Interestingly, combination therapy with L-AmB and miltefosine has been assessed for PKDL by Ramesh et al.80. Association of L-AmB (3 injections 5 mg/kg on days 1, 8, and 15) with miltefosine (100 mg/day capsules for 45 days) was compared with miltefosine monotherapy (90 days) and demonstrated rapid decline in parasite load, along with 100% clinical cure and no reports of relapse. However, in the miltefosine monotherapy group, although gradual reduction in parasite load and ultimate clinical cure was attained, 25% of patients relapsed at 18 months of follow-up80. Given the promising report of this association, more clinical trials are warranted to substantiate the above finding. Moreover, the briefer duration of therapy along with minimal side effects encourage further application of this therapy for the treatment of PKDL.
Amphotericin adverse effects
In ~80% of patients, infusion-related adverse effects and nephrotoxicity is documented. As AmB interacts also with cholesterol in human cell membranes, toxicity is expected. Common adverse effects include:
− Hypokalemia, hypomagnesemia, and anaphylaxis84.
− Nephrotoxicity correlates with conventional AmB, but it is reversible post-AmB cessation. Besides, avoiding concomitant nephrotoxic drugs and appropriate hydration can reduce the incidence of nephrotoxicity, and liposomal formulations have considerably lower chances of renal toxicity. Vasoconstriction of afferent renal arterioles results in decreased renal blood flow and GFR accounting for nephrotoxicity85.
− Long-term AmB is associated with normochromic, normocytic anemia secondary to low erythropoietin concentrations86.
− Initial doses of AmB often cause fever, headache, cheilitis, hypotension, tachypnea, and vomiting within 2-6 h of perfusion. Transient substernal chest pain and flank pain are observed predominantly with d-AmB and ABCD (rarely with L-AmB and AMLC), but resolve on discontinuation and administration of intravenous diphenhydramine. This is explained by the release of proinflammatory cytokines such as interleukin (IL-1β), tumor necrosis factor-α, IL-6, and IL-8, after recognition via toll-like receptors and transmembrane signaling protein CD148.
− Cutaneous reactions mainly comprise of urticarial reactions and thrombophlebitis at the injection site. Drug rash with eosinophilia and systemic symptoms and cutaneous vasculitis have also been described with L-AmB8,87,88. The suggested etiology of urticarial eruptions is liposomal activation of the complement cascade and subsequent release of C3a and C5a89.
− Rare side effects include new onset dilated cardiomyopathy with associated heart failure that subsides within 6 months of treatment discontinuation. Other unusual toxicities include hyperbilirubinemia, elevated hepatic transaminases, pancreatitis, and pseudohypophosphatemia (observed even with L-AmB)89.
Amphotericin in special populations
Pregnancy
During pregnancy, AmB should be used only when indicated. According to IDSA guidelines, for invasive candidiasis in pregnancy, AmB is the drug of choice. Further, potential adverse effects on the fetus can be reduced by using the ideal body weight of the mother rather than the total body weight. Furthermore, it would be preferable to use the liposomal formulation due to the minimal risk of teratogenicity90.
Lactation
AmB can be used during lactation. As it is highly protein-bound, has a large molecular weight, and is poorly absorbed, the probability of its secretion in breast milk is minimal91.
Pediatric patients
All preparations of AmB have been used in children with documented safety and efficacy. However, its usage in neonates still needs more data92.
Geriatric patients
ABLC given to elderly patients at a dose of 5 mg/kg/day is not associated with significant adverse events21.
Patients with renal and hepatic impairment
No dose adjustment is needed in patients with renal impairment based on creatinine clearance estimate. L-AmB has been successfully dispensed in patients with pre-existing renal impairment. The effect of L-AmB in patients with hepatic impairment is not known21.
Storage and administration
This is elaborated in table 3.
Table 3 Storage and administration guidelines for Amphotericin B
| Feature evaluated | AmB deoxycholate | Liposomal AmB |
|---|---|---|
| Storage requirements | Store in dry form at 2-8°C away from light | Store in dry form at 2-8°C away from light |
| Reconstitution | 50 mg vial + 10 mL sterile water (5 mg/mL solution) | 50 mg vial + 12 mL sterile water (4 mg/mL solution) |
| Further dilution | 500 mL of 5% dextrose (0.1 mg/mL) | 5% dextrose to have 1-2 mg/mL (adults) 0.2-0.5 mg/mL (infants and children) |
| Test dose | 0.1 mg/kg (not exceeding 1mg) infusion over 20-60 min | 0.1 mg/kg (not exceeding 1mg) infusion over 20-60 min |
| Administration | Over 2-6 h via a distal vein Immediately after preparation |
Over 2-6 h via a distal vein Immediately after preparation |
| Premedication | For infusion-related reactions Paracetamol Diphenhydramine Corticosteroids (30 min before infusion) |
For infusion-related reactions Paracetamol Diphenhydramine Corticosteroids (30 min before infusion) |
| Monitoring requirements | Daily serum creatinine Regular K+, Mg2+, Ca2+, PO4- Proper hydration For infusion-related reactions (15 min-3 h) Signs of hypokalemia |
Regular K+, Mg2+, Ca2+, PO4- Proper hydration For infusion-related reactions (15 min-3 h) Signs of hypokalemia |
| Dose adjustment | If serum creatinine > 2.5 mg/dL Reduce dose by 50%, or Switch to L-AmB |
Based on clinical response |
| Special consideration | Higher risk of nephrotoxicity Careful monitoring of renal function |
Better renal tolerance Preferred in patients with/at risk of renal dysfunction |
| Emergency monitoring | For suspected hypokalemia (muscle cramps, drowsiness) Immediate ECG Serum K+ measurement Prompt correction of electrolytes Adequate hydration |
For suspected hypokalemia (muscle cramps, drowsiness) Immediate ECG Serum K+ measurement Prompt correction of electrolytes Adequate hydration |
Drug interactions
As AmB is not metabolized by the cytochrome P450 pathway, documented drug-drug interactions are few. Cyclosporine and tacrolimus used in kidney transplant can increase the toxicity of AmB, and there is an increased risk of hypokalemia with concomitant use of digoxin and corticosteroids93.
Amphotericin resistance
Fortunately, AmB resistance is rare compared to other antifungal agents. However, resistance has been encountered for Aspergillus terreus due to a reduction in polyene-induced oxidative stress94, for Aspergillus flavus and Candida tropicalis due to an increase in 1,3α-glucan and 1,3β-glucan fraction that leads to an alteration of the fungal cell wall with subsequent AmB resistance95,96, and for various Candida spp. a mutation in the ERG genes that alters the sterol composition of the fungal cell membrane, thereby preventing AmB antifungal effects97.
Novel oral amphotericin formulations
To date, oral AmB formulations are at various stages of preclinical development with some making it to human clinical investigations. Oral AmB lipid-based formulation has been specifically designed to reduce limitations existing with intravenous formulations as per the treatment of systemic mycoses and VL98.
This formulation consists of a self-emulsifying mixture of monoglycerol oleate, lauroyl polyoxyl-32 glycride, and D-α-tocopherol polyethylene glycol succinate (a penetration enhancer). Besides, this formulation further stabilizes the less toxic monomeric form of AmB98.
Recently 2 human phase-I clinical studies have been completed with the oral AmB formulation (capsule). Further, in both phase-Ia and Ib human clinical studies, the primary endpoint of safety and tolerability following administration of single ascending doses and repeated doses were met, including no signs of kidney, liver, and gastrointestinal adverse effects99.
Besides, the self-nanoemulsifying drug delivery system was utilized for AmB encapsulation to enhance its oral bioavailability100. With the above promising findings, oral AmB could revolutionize the management of many tropical dermatoses due to easier administration, reduced toxicity, cost efficacy, and the ability to be stored at room temperature.
Conclusion
AmB is a valuable drug for the treatment of many tropical dermatoses. With research going on regarding oral preparations of the drug, its utility could become more widespread due to the ease of administration. Further, although the use of topical AmB has been employed for PV and genital candidiasis, the use of AmB per se cannot be widely employed for these indications, due to very low quality of evidence (confined to case reports or trials with groups of 10 patients).

