











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Kaposi’s sarcoma (KS) is an angioproliferative neoplasm associated with human herpesvirus 81. Diagnosis is based on clinical features, with histological and immunohistochemical confirmation2. It occurs more frequently in males3. The overall incidence and mortality have changed over the last few decades, with a decrease in the epidemic subtype in the last 30 years with the introduction and diffusion of antiretroviral therapy (ART)2,3.
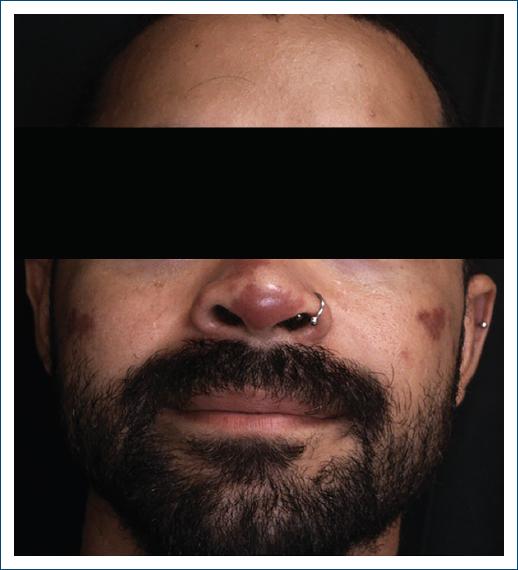
There are four major subtypes, which are histologically indistinguishable: classic (typical of older men from the Mediterranean region) (Fig. 1), endemic (a more aggressive form, mostly seen in young adults from sub-Saharan Africa), iatrogenic (a form seen in transplant patients or those undergoing intense immunosuppressive treatments) and epidemic (human immunodeficiency virus [HIV]-positive patients) (Fig. 2)1,4.

Figure 1 Classic subtype: erythematous to violaceous plaque extending across the medial plantar arch and heel, with an infiltrative component, areas of induration, and swelling. Multiple discrete ulcerated nodules with crusting are present within the plaque.
The treatment of KS is heterogeneous, depending on the cause and the clinic, including local and/or systemic therapeutic strategies4.
The aim of our study was to describe the characteristics of patients with KS diagnosed by histology at Hospital Garcia de Orta, in Portugal, over 15 years, between March 2009 and March 2024. The data collected was used to characterize the demographics of the patients. Furthermore, we also sought to understand the variations between each subtype, particularly regarding the time to diagnosis, age at diagnosis, location of the disease (whether it was confined to the skin or systemic), and the therapeutic approach used. In addition, we conducted comparisons with other Portuguese and European studies that employed similar methodologies and with overlapping years of data collection.
Material and methods
This is a retrospective, descriptive, and observational study. It included patients with a histological diagnosis of KS at Hospital Garcia de Orta in Portugal between March 2009 and March 2024. Three patients were excluded due to missing data.
The endemic subtype was assumed for patients from sub-Saharan Africa, and the epidemic subtype was assumed for patients with HIV infection, regardless of their place of birth.
Clinical and demographic data were studied (age, gender, place of birth, subtype, location of lesions, time until diagnosis, and treatment used).
Statistical analysis was carried out using IBM Statistical Package for the Social Sciences Statistics, version 29.0. The correlations between the variables were considered statistically significant if p < 0.05.
Results
The study included a total of 55 patients, 43 (78.2%) male and 12 (21.8%) female. The age of our patients at diagnosis ranged from 26 to 92 years, with a mean age at diagnosis of 63.55 ± 18.7. The mean male age at diagnosis was 61.26 ± 17.434, and the mean female age at diagnosis was 71.75 ± 21.495. The distribution of ages at diagnosis by gender was not statistically significant (p = 0.057).
Over the years, there have been fluctuations in the number of KS diagnoses per year, with a statistically significant downward tendency (p = 0,005). The maximum number of diagnoses per year was in 2011 (Fig. 3).
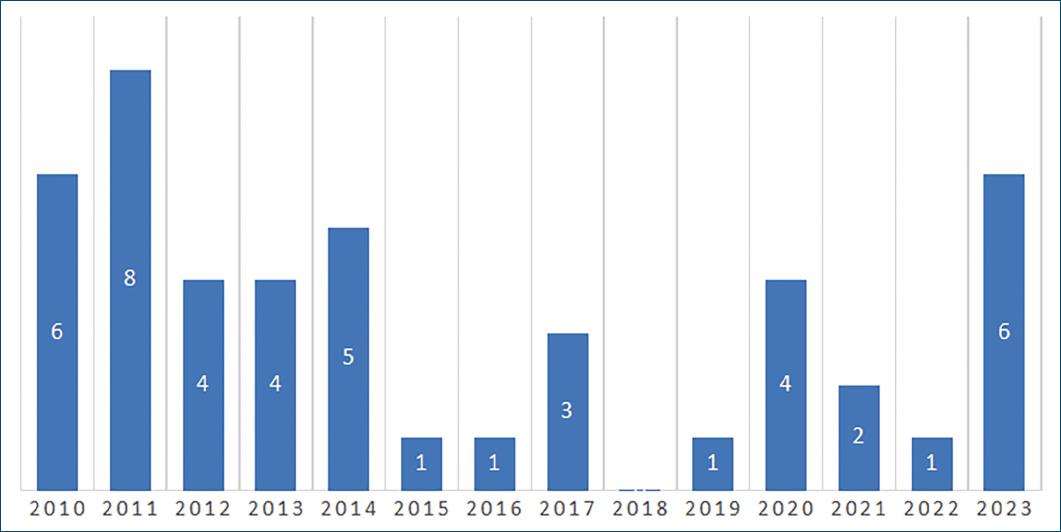
Figure 3 Number of diagnoses per year. 2009 and 2024 were not included because the data were collected from March 2009 to March 2024.
The majority of patients (67.3%) presented with lesions in a single anatomical site, mainly on the lower limbs. Only 32.7% of patients had lesions in two or more locations. Table 1 shows the anatomical locations of the lesions.
Table 1 Distribution of lesions by anatomical location
| Location of lesions | n (%) | Location of lesions | n (%) |
|---|---|---|---|
| Single site | 37 (67.3%) | Multiple sites | 18 (32.7%) |
| Head and neck | 3 (5.454%) | Lower limbs and trunk | 7 (12.726%) |
| Trunk | 2 (3.636%) | Lowe and upper limbs | 7 (12.726%) |
| Lower limbs | 31 (56.358%) | Hands and feet | 2 (3.636%) |
| Genitals | 1 (1.818%) | Genitals and lower limbs | 1 (1.818%) |
| Head, trunk, and lower limbs | 1 (1.818%) |
Patients were classified into the four subtypes mentioned above: the classic subtype was the most common (38.2%), followed by the epidemic (36.4%), the endemic (23.6%) and finally the iatrogenic (1.8%) (Table 2). The only case of the iatrogenic subtype is a patient with myasthenia gravis and thymoma under high doses of systemic corticoids and rituximab. In the endemic subtype, six patients were from Cape Verde, three patients were from São Tomé e Príncipe, two patients were from Guinea-Bissau, and two patients were from Angola. Of the 20 patients with the epidemic subtype, 17 (85%) had a low TCD4 + lymphocyte count at the time of diagnosis, 2 (10%) had a normal count, and in 1 patient (5%), the count was unknown. The mean age at diagnosis was 77.9 ± 11.251 in the classic subtype, 69.0 ± 12.955 in the endemic subtype, 45.25 ± 12.315 in the epidemic subtype, and 57 in the iatrogenic subtype (Table 2). The observed differences in age at diagnosis for each subtype are statistically significant (p < 0.001).
Table 2 Distribution of KS cases based on clinical and epidemiological characteristics, mean age at diagnosis, time (in months) until diagnosis, and skin and visceral involvement
| Subtype | Number of cases (percentage) | Mean age at diagnosis | Time (in months) until diagnosis | Skin involvement only (%) | Skin and visceral involvement (%) |
|---|---|---|---|---|---|
| Classic | 21 (38.2) | 77.9 ± 11.251 | 8.36 ± 8.801 | 21 (100) | 0 (0) |
| Epidemic | 20 (36.4) | 45.25 ± 12.315 | 10.95 ± 15.736 | 9 (45) | 11 (55) |
| Endemic | 13 (23.6) | 69.0 ± 12.955 | 40.78 ± 50.23 | 11 (84.6) | 2 (15.4) |
| Iatrogenic | 1 (1.8) | 57.0 | 6.0 | 1 (100) | 0 (0) |
| 55 | 42 (76.4) | 13 (23.6) |
The longest interval (in months) between the onset of symptoms and diagnosis was observed in the endemic subtype (40.78 ± 50.23), which exhibited a significantly longer duration than other subtypes (Table 2). The overall mean time was 18.3 months.
All patients with the classic subtype had only cutaneous involvement, just 2 patients (15.4%) with the endemic subtype demonstrated both cutaneous and visceral involvement, and the majority (55%) of patients with the epidemic subtype had both cutaneous and visceral involvement (Table 2).
Among the 55 patients included in the study, 37 (67.3%) underwent computed tomography (CT) scans, 16 (29.1%) underwent upper endoscopy, 15 (27.3%) underwent colonoscopy, and 11 (20.0%) underwent bronchofibroscopy. In terms of visceral involvement, the most common organs involved were the lungs (in seven patients), the gastrointestinal tract (in four patients), and the lymph nodes (in three patients).
About 56.4% of the patients received only one treatment, whereas 30.9% of cases necessitated the combination of multiple treatments. It is important to note that the follow-up of 7 patients (12.7%) was lost, and the treatment they received is unknown. Treatment approaches were both local and systemic and included ART, surgery, chemotherapy (CT), surveillance, radiotherapy, and cryosurgery.
The classic subtype predominantly underwent surgical intervention (10 cases), indicating a preference for localized surgical intervention in this subtype. The surveillance approach was used in two cases. The remaining cases displayed variability in treatment choice. The endemic subtype exhibited a broader therapeutic distribution, with CT alone being the most frequently applied treatment used in four cases. The epidemic subtype showed a marked reliance on ART, either alone or in combination with other treatments. ART alone was used in seven cases, whereas ART combined with CT was used in 11 cases.
Of the 55 patients, 18 died (32.7%). The mean time from diagnosis was 3.5 years, 8 of the classical subtype (38.1% within subtype), 2 of the endemic subtype (15.4% within subtype), none of the iatrogenic subtype, and 8 of the epidemic subtype (40% within subtype). The mean time (in years) from diagnosis to death was higher in the endemic subtype (6.00), followed by the classic subtype (4.63) and finally the epidemic subtype (1.75), but without statistical significance (p = 0.146).
Discussion
This study conducted a retrospective analysis of KS cases over a 15-year period in a hospital in Portugal. The demographic data from our study reveal an average age at diagnosis of 65.55 years (higher in men than in women), with a higher prevalence in men compared to women. These findings confirm previous studies indicating that KS is more common in men and diagnosed at older ages3.
In a retrospective study carried out by Resende et al. between January 2001 and December 2013, cases from the Egas Moniz Hospital and the Centro de Dermatologia Médico-Cirúrgica de Lisboa were analyzed. The study included 91 patients, 67% of whom belonged to the classic subtype, 30.8% to the epidemic subtype, 1.1% to the endemic subtype, and 1.1% to the iatrogenic subtype5. Compared to our results, the percentages of the epidemic and iatrogenic subtypes were similar. However, there was a considerable increase in the prevalence of the endemic subtype and a decrease in the classic subtype. Given that both studies used similar methodologies and were carried out in similar geographical areas (both belonging to the Lisbon metropolitan area), about a decade apart, these differences-particularly the higher proportion of endemic subtype cases in our cohort (23.6% compared to 1.1%) can be explained by the recent migratory flow.
In addition, a retrospective study conducted by Russo et al. in Italy between 1993 and 2022 analyzed 86 patients. Of these, 43.02% were classified as belonging to the classic subtype, 33.73% to the epidemic subtype, 3.49% to the endemic subtype, and 19.77% to the iatrogenic subtype4. Compared to our study, the Italian study reported a higher percentage of cases classified under the iatrogenic subtype. This difference can be explained by the fact that our hospital is not a transplant center, thereby limiting the number of epidemic subtype cases followed in our hospital. In the last decade, there has been a decrease in cases of iatrogenic KS, which can be explained by new-generation immunomodulators that reduce the immunosuppressive status of patients and enable the optimization of the dose of immunosuppressive medications6.
The epidemic subtype demonstrated the highest frequency of visceral involvement in our cohort (Table 2), reflecting its aggressive clinical behavior as previously described in the literature7. This observation highlights the impact of immunosuppression in HIV-positive patients, contributing to more advanced and disseminated disease presentations characteristic of this subtype. The exclusively cutaneous involvement in other subtypes (classic and iatrogenic) suggests that these subtypes may have less aggressive behavior in terms of visceral dissemination, which is consistent with the expected clinical profile.
The time from the onset of lesions to diagnosis was longer in the endemic subtype. This may be attributed to the lower level of health literacy observed in this population or to greater difficulty in accessing health care.
There was a great heterogeneity in the therapeutic modalities used, which shows the great complexity of treating KS and the need to adapt the treatment to each subtype, as shown by the predominance of ART in the epidemic subtype, surgery in the classic subtype and chemotherapy in the endemic subtype (Table 3).
Table 3 Distribution of therapeutic modalities by subtype
| Treatment | Classic | Endemic | Epidemic | Total |
|---|---|---|---|---|
| RT | 1 | 1 | 0 | 2 |
| CT | 0 | 4 | 0 | 4 |
| RT + CT | 1 | 3 | 0 | 4 |
| ART | 0 | 0 | 7 | 7 |
| ART + CT | 0 | 0 | 11 | 11 |
| Surveillance | 2 | 1 | 0 | 3 |
| Surgery | 10 | 2 | 0 | 12 |
| Cryosurgery | 1 | 0 | 0 | 1 |
| Surgery + cryosurgery | 1 | 0 | 0 | 1 |
| ART + cryosurgery | 0 | 0 | 1 | 1 |
| Surgery + RT | 1 | 0 | 0 | 1 |
| Shaving + electrosurgery | 0 | 1 | 0 | 1 |
| Total | 17 | 12 | 19 | 48 |
RT: radiotherapy, CT: chemotherapy, ART: anti-retroviral drug.
The preference for surgery as the primary treatment in the classic subtype reflects the option of localized therapies for lesions associated with this subtype, which generally exhibit a slower and more localized progression. In contrast, for the epidemic subtype, the majority of patients underwent a combination of ART and CT, although a notable proportion underwent ART alone. ART monotherapy in patients with disease limited to the skin can significantly reduce the size of the lesions and achieve complete remission in 35% of cases within 39 months of treatment8. However, in cases involving more extensive skin disease or with visceral involvement, it is necessary to combine systemic drugs such as doxorubicin or paclitaxel. The limited use of radiotherapy in our cohort may be explained by the anatomical distribution of the lesions. As radiotherapy is most effective for localized symptomatic lesions, its role is more limited in cases of widespread disease. In addition, in patients with extensive lower limb involvement, radiotherapy may be less practical. Furthermore, resource availability and institutional treatment protocols may limit the routine use of radiotherapy, and alternative local therapies, such as surgical excision, have been preferred for isolated lesions in accessible areas.
Our study has some limitations, such as being retrospective and unicentric. As it included cases from 2009 onwards, there was a lack of information, which made statistical analysis challenging.
Conclusion
This study highlights there is still a considerable delay between symptoms onset and diagnosis of SK, and that it is not homogeneous between the subtypes. Treatment should be adjusted on a case-by-case basis and adapt to the subtype and extent of the disease. For many years, systemic therapy was represented by chemotherapy, but with the emergence of translational research, it can currently count on immunotherapy and targeted therapies with promising results. Immune checkpoint inhibitors, such as pembrolizumab and nivolumab, have shown promising efficacy. Combination approaches, including ipilimumab with nivolumab and pembrolizumab with lenvatinib, aim to improve disease control. Ongoing trials are also evaluating nivolumab with pomalidomide and cabozantinib, as well as dostarlimab in epidemic KS9.

