











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Erythema induratum (EI), also known as nodular vasculitis, is a rare form of panniculitis characterized by erythematous nodules typically located on the lower limbs. Initially described as a hypersensitivity reaction to Mycobacterium tuberculosis (EI of Bazin)1,2, EI can also be associated with other diseases, drugs, or be idiopathic2.
This case report describes an unusual presentation of EI secondary to Pseudomonas aeruginosa bacteremia in an elderly patient with multiple comorbidities. This is a unique presentation that highlights the diverse etiologies of EI and the diagnostic challenges it presents.
Case presentation
An 84-year-old man with a history of chronic kidney disease on hemodialysis, cerebrovascular disease, atrial fibrillation, hypertension, hyperuricemia, and diabetes was admitted to the Nephrology Department due to left leg cellulitis and bacteremia caused by Pseudomonas aeruginosa.
After six days of hospitalization under targeted antibiotic therapy, dermatology was consulted due to persistent inflammatory lesions on the affected limb. Examination revealed edema, slight erythema, and increased local temperature, with five nontender, erythematous, centimetric nodules distributed in a sporotrichoid pattern on the anterior aspect of the upper third of the left leg and knee (Fig. 1). Differential diagnosis included infectious panniculitis and erythema nodosum.

Figure 1 Physical examination revealing edema, slight erythema, and five nontender, erythematous, centimetric nodules distributed in a sporotrichoid pattern on the anterior aspect of the upper third of the left leg and knee.
A deep skin biopsy of one nodule was performed. Histopathological examination (Fig. 2) revealed a mixed-pattern panniculitis, with a marked mixed inflammatory infiltrate, multiple neutrophils, abscess formation, multinucleated giant cells, leukocytoclasia, cytosteatonecrosis, focal granuloma formation, and some vessels with fibrinoid necrosis, with negative staining for bacteria, mycobacteria and fungi, favoring the diagnosis of EI.
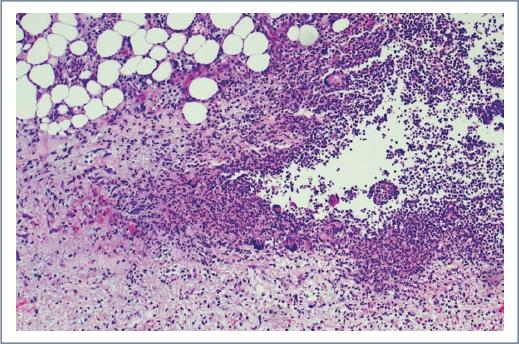
Figure 2 Histopathological examination (hematoxylin & eosin, 100x) of a deep skin biopsy revealing a mixed-pattern panniculitis, with a marked mixed inflammatory infiltrate, multiple neutrophils, abscess formation, multinucleated giant cells, leukocytoclasia, cytosteatonecrosis, focal granuloma formation, and some vessels with fibrinoid necrosis.
Complementary investigation for etiological study revealed elevated inflammatory markers (erythrocyte sedimentation rate of 68 mm/1st hour, c-reactive protein 3.25 mg/dL), a normal chest X-ray, negative serologies for human immunodeficiency virus, syphilis, hepatitis B and C, and a negative interferon-gamma release assay (IGRA) test.
The diagnosis of EI of Whitfield (or nodular vasculitis) secondary to P. aeruginosa infection was made. The patient showed overall improvement with targeted antibiotic therapy, including 17 days of piperacillin/tazobactam and 14 days of amikacin. The skin nodules ulcerated, giving place to painless superficial ulcers, with good response to local wound care.
Given the absence of symptoms associated with the skin lesions, the good response to local treatment, and the resolution of the associated infection, the patient remains under clinical surveillance and complete healing is expected.
Discussion
Erythema induratum is traditionally classified into three subtypes: associated with tuberculosis (Bazin type), associated with other diseases or drugs (Whitfield type), and idiopathic. Latent or active tuberculosis is the most commonly reported identifiable cause1,2. Differentiation between these subtypes relies on clinical history, physical examination and complementary investigations, as clinical and histological findings alone are indistinguishable2.
Erythema induratum typically affects adult women and presents with subcutaneous erythematous nodules on the posterior aspect of the lower legs, which can ulcerate and heal with scarring and lipoatrophy1,2. Systemic symptoms are generally absent2. Diagnosis requires an incisional biopsy for histopathological and microbiological examination to exclude infectious panniculitis2,3.
The histopathological hallmark of EI is a lobular panniculitis with necrosis and a mixed granulomatous infiltrate with vasculitis1,2. The inflammatory infiltrate is mixed, containing lymphocytes, plasma cells, histiocytes, neutrophils, and eosinophils, with extravascular foci of fibrinoid necrosis2,4. The vasculitis may involve various vessel types in the subcutaneous septa and/or lobules2.
Treatment primarily involves addressing the underlying disease, together with symptomatic treatment including nonsteroidal anti-inflammatory drugs, rest, elevation, and compression1,2. Successful treatment of the underlying condition usually leads to the resolution of EI1,2,4.
In the described clinical case, the leg nodules subsided along with the improvement of the systemic infection following antibiotic administration, suggesting that EI was caused by P. aeruginosa infection. This diagnosis was supported by the negative IGRA test and negative microbiological stains, excluding tuberculosis and infectious panniculitis, respectively. However, the location of the nodules on the anterior leg and knee, and the fact that the patient was an elderly man, are atypical for this diagnosis, posing a diagnostic challenge.
The main differential diagnosis considered was infectious panniculitis secondary to P. aeruginosa, a rare cause. In our case, despite negative histopathological stains, skin cultures were not performed. Another important differential diagnosis to consider in the context of Pseudomonas bacteremiawas ecthyma gangrenosum, but the absence of blister formation or necrotic ulcers ruled out this option.
The patient shows a favorable clinical evolution, with resolution of the underlying infection, progressive healing of the leg ulcers, and no recurrence of nodules.
Literature reports 12 cases3,5-9 of infectious panniculitis secondary to P. aeruginosa (Table 1). However, to our knowledge, this is the first reported case of EI secondary to P. aeruginosa, and it’s therefore important to highlight the clinical presentation and management of this rare cause of EI.
Table 1 Summary of the reported cases of infectious panniculitis secondary to Pseudomonas aeruginosa
| Author and year | Patient’s gender and age | Clinical presentation |
|---|---|---|
| Gosnell H et al. 2021 | Male, 57 years | Diffuse, erythematous subcutaneous nodules, and several necrotic ulcerations surrounded by erythematous halos, on the abdomen, upper, and lower extremities |
| Yendo et al. 2022 | Female, 44 years | Erythematous nodules on the upper back, chest, face, arms, and breasts |
| Penz et al. 2010 | Female, 72 years | Ulcers on the right leg and a nodule on the right thigh |
| Moyano et al. 2011 | Female, 63 years | Erythematous nodules, some with pustules on the surface |
| Bagel et al. 1986 | Female, 56 years | Erythematous subcutaneous nodules, pustules, and hemorrhagic blisters on the extremities |
| Patterson et al. 1989 | ND | No information available |
| Roriz et al. 2014 | Female, 80 years | Multiple ulcers on the right lateral malleolus and inflammatory nodules on the left thigh |
| Roriz et al. 2014 | Male, 50 years | Inflammatory nodules on the left leg, with some infracentimetric cutaneous ulcers |
| Roriz et al. 2014 | Female, 70 years | Inflammatory nodules on the right limb |
| Aleman et al. 1999 | ND | Erythematous subcutaneous nodules on the posterior surface of the right leg |
| Picard et al. 2011 | Female, 82 years | Multiple painful red-purple nodules on the right leg and inguinal lymphadenopathy |
| Saito et al. 2024 | Male, 11 months | Erythema in the right abdomen and left lower leg |
Conclusion
This case report emphasizes the importance of considering EI in the differential diagnosis of inflammatory skin lesions in patients with P. aeruginosa bacteremia. Comprehensive clinical evaluation, histopathological examination and exclusion of common infectious agents are crucial for accurate diagnosis and management. The successful resolution of the patient’s skin lesions with appropriate antibiotic therapy highlights the importance of treating the underlying cause in EI. This case adds to the limited literature on nontuberculous etiologies of EI and emphasizes the need for awareness of its diverse presentations and etiologies.

