











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Cutaneous metastasis is a common manifestation of the underlying visceral malignancy1. The incidence of skin metastasis varies from 2% to 9% in a primary malignant tumor2,3. Breast cancer is the most common cancer associated with cutaneous metastasis after melanoma4. This metastasis can result from lymphatic embolization, hematogenous, or from direct implantation5. It usually presents in the form of solitary to multiple nodules. Rarely, it can present in a zosteriform pattern with only a few cases, which have been described in the literature6. Out of this, only about twelve cases of zosteriform cutaneous metastasis due to underlying breast carcinoma have been described so far7.
Case report
Case 1
A 49-year-old female patient was referred from the oncology department to the dermatology outpatient department (OPD). The patient reported the appearance of multiple grouped vesicles and nodules on the right side of the breast associated with excruciating pain. She was a known case of Grade three infiltrating ductal adenocarcinoma of the right breast for 2 months, having T4N3M0 stage, for which she had undergone three cycles of Neo adjuvant chemotherapy with Epirubicin, Cyclophosphamide, and 5-Fluorouracil, and was due for the fourth cycle.
On dermatological examination, the patient had multiple grouped vesicles and nodules coalescing to form plaques in a dermatomal distribution, superimposed with erosions and crusting at some sites on the right side of the breast, associated with hyperpigmentation of surrounding skin along with peau d’ orange appearance around nipple and areola (Fig. 1A and B). The lesions measured 2-3 cm and were tender on palpation. The patient was treated for Herpes zoster with tablet Acyclovir 800 mg 5 times a day along with anti-inflammatory analgesic medications and tablet Amitriptyline/Pregabalin combination for neuropathic pain, but the lesions were persistent even after 14 days of treatment. On follow-up, similar lesions were found to be spreading over the right arm, right shoulder, and right inframammary region.
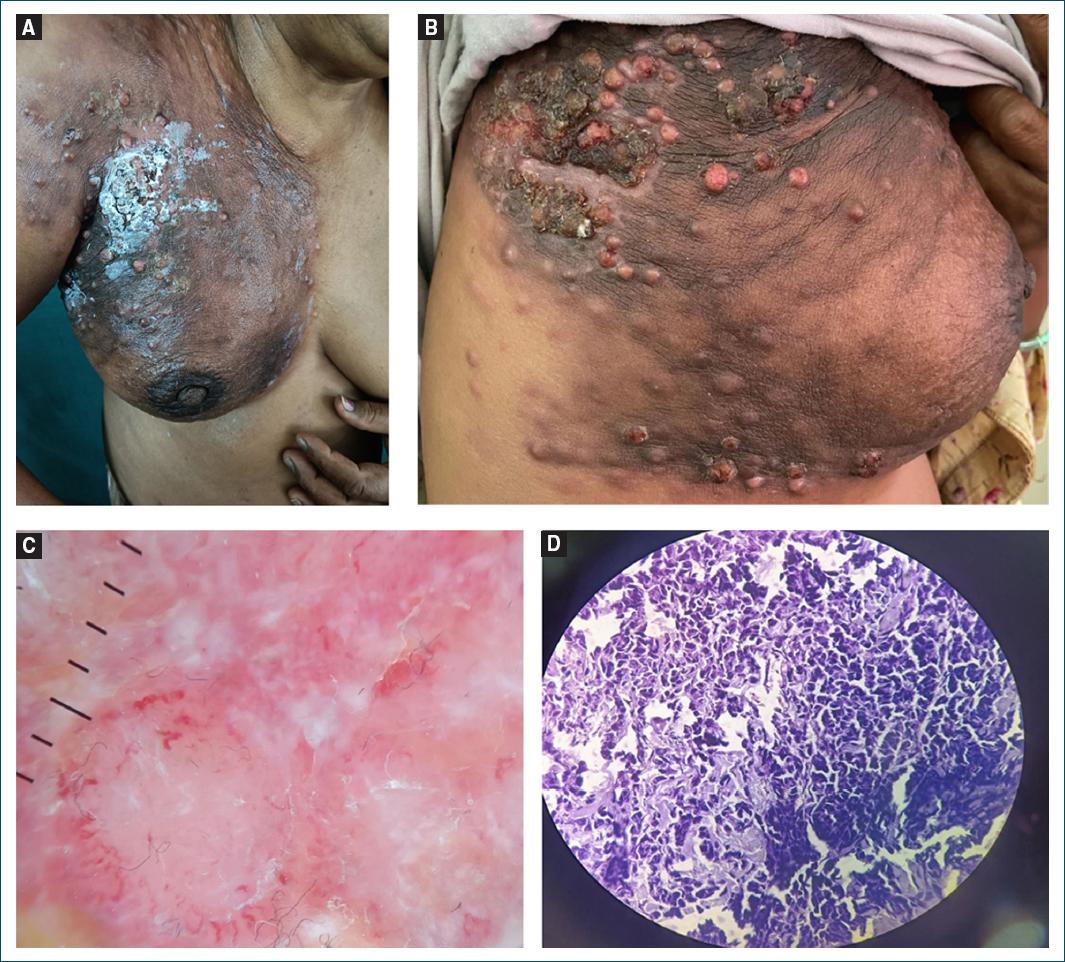
Figure 1 A: multiple crusted papulo-nodules with few vesicles on the right breast in a dermatomal distribution. B: close view of the lesions showing papulo-nodules in the same patient. C: ×10 magnification of DL4 dermoscope under polarized light: contact dermoscopy demonstrated yellow areas, polymorphic vessels, whitish bright lines, and structureless areas (depicted by black arrows). D: H&E ×40 showing dermal infiltration by hyperchromatic pleomorphic nuclei with increased nuclear: cytoplasmic ratio.
Dermoscopy revealed yellow areas, polymorphic vessels, whitish bright lines, and white structureless areas (Fig. 1C).
All routine investigations were within normal limits.
HPE of skin biopsy showed a dermis infiltrated by hyperchromatic pleomorphic nuclei with cells having increased nuclear:cytoplasmic ratio (Fig. 1D). Results were consistent with adenocarcinomatous metastatic deposits. Immunohistochemistry was negative for ER, PR and HER-2 neu, and positive for cytokeratin 7, indicating breast as the primary site of neoplasm.
Hence, the patient was diagnosed as Zosteriform cutaneous metastasis and referred to the oncology department for further management.
Case 2
A 54-year-old female patient was referred from surgery OPD to dermatology OPD.
The patient reported the appearance of multiple painful nodules on the left side of the chest along with a mastectomy scar mark on the left side of the chest.
She was a known case of infiltrating ductal carcinoma breast, T4N2M0, and had undergone five cycles of neoadjuvant chemotherapy followed by salvage mastectomy 4 months ago.
On dermatological examination, the patient had a few grouped vesicles with crusted plaques and nodules with ulceration over the left mastectomy scar site and surrounding skin extending onto the left lateral side and back in dermatomal distribution along with reddish-yellow plaque with superimposed crusts and nodular surface with peau d’ orange appearance on right side of chest (Fig. 2A and B).
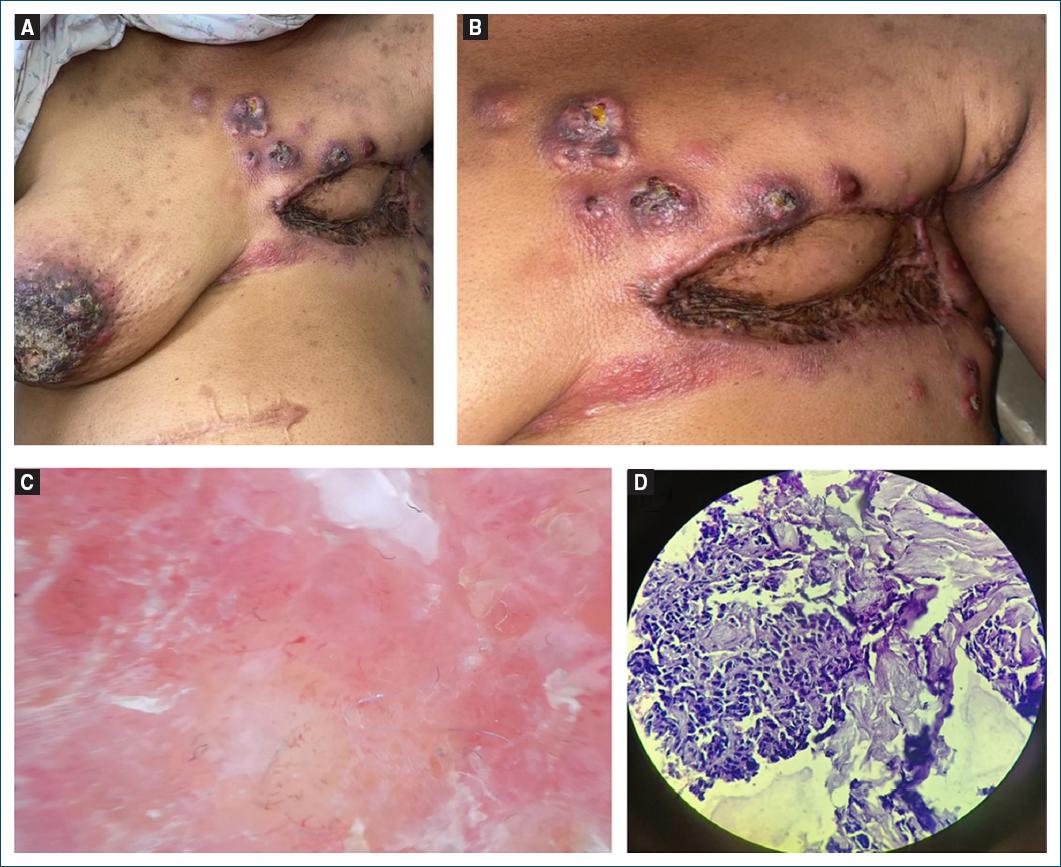
Figure 2 A: multiple grouped vesicles, papules, and nodules superimposed with crust on left breast in dermatomal distribution along with mastectomy scar. B: close view of the lesions showing the lesions in the same patient. C: ×10 magnification of DL4 dermoscope under polarized light: contact dermoscopy demonstrated multiple, discrete, polymorphic blood vessels with pinkish-white structureless areas and yellow areas (depicted by black arrows). D: H&E ×40 showing metastatic carcinomatous deposits.
Dermoscopy revealed multiple, discrete, polymorphic blood vessels with pinkish-white structureless areas and yellow areas (Fig. 2C).
Routine investigations were within normal limits.
Biopsy of the lesions was planned keeping Herpes zoster and zosteriform cutaneous metastasis as the two main differentials. HPE showed appearances consistent with metastatic carcinomatous deposits (Fig. 2D).
Immunohistochemistry was positive for ER, PR, cytokeratin 7, and negative for HER-2 neu, indicating breast as the primary site of neoplasm.
The patient was diagnosed as zosteriform cutaneous metastasis due to underlying malignancy and referred to the surgery department for further management.
Discussion
Breast cancer is the most common tumor associated with cutaneous metastasis (excluding melanoma) in clinical practice. The incidence of cutaneous metastasis in carcinoma breast is about 24%8.
Various morphologies of breast carcinoma are seen, some of which are commonly encountered such as single to multiple erythematous infiltrating papules and nodules or ulcers. Other rare variants are carcinoma erysipeloides, carcinoma en cuirasses, carcinoma telangiectaticum, alopecia neoplastica, metastasis to the inframammary crease, and zosteriform metastasis (as in the abovementioned cases)4. Dermoscopy showing vascular structures within a cutaneous nodule in patients with known underlying cancer (as in our case reports) should raise suspicion for cutaneous metastasis as it suggests angiogenesis9.
Histopathology of cutaneous breast carcinoma may show interstitial, nodular, mixed interstitial and nodular, or inflammatory carcinoma10, while that of Herpes zoster shows multinucleated keratinocytes, acantholytic cells known as Tzanck cells with distinct nuclear inclusions, perineural infiltrate of lymphocytes and neutrophils, sometimes associated with intraneural involvement11. Biopsy, thus helps in confirming the diagnosis.
Treatment options of cutaneous metastasis include systemic chemotherapy, surgical resection, and radiation.
The prognosis of a patient with cutaneous metastasis depends primarily on the behavior of the underlying tumor and its response to treatment. In breast carcinoma, immunohistochemistry plays a very important role in deciding the treatment and prognosis.
Cutaneous metastasis from breast cancer usually occurs in later stages4. However, if the underlying malignancy is not known, cutaneous metastasis can rarely present as the initial sign of the cancer. In either case, it shows poor response to treatment.
Conclusion
The above cases highlight the importance of differentiating herpes zoster from zosteriform cutaneous metastasis as it is a great mimicker of the former.
Since zosteriform metastasis is not so commonly seen, it is likely to be missed. In the elderly and cases of known underlying malignancy, zosteriform cutaneous metastasis should always be kept in mind though herpes zoster becomes the first differential due to the immunocompromising nature of the disease.
Biopsy is vital to confirm the diagnosis though dermoscopy aids in raising the suspicion.

