











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Cutaneous pathergy is a phenomenon demonstrating an exaggerated wound response following minor trauma. While often associated with inflammatory conditions such as Bechet’s disease and pyoderma gangrenosum, carcinogenesis secondary to pathergy has been described1-3. We have previously described cutaneous eruptive post-operative squamous cell carcinomas (SCCs) exhibiting a pathergy-like reaction around surgical wound sites1. The pathogenesis for this process is not well understood. We have noted it to occur more frequently on the lower extremities. Recognition of this phenomenon may be perplexing to clinicians who do not encounter it regularly; it may represent a practice gap for plastic surgeons and dermatologists who perform cutaneous surgery. Herein, we report on two female patients with a multitude of pathergic SCCs demonstrating a dramatic response to our therapeutic regimen.
Report of two cases
Case 1
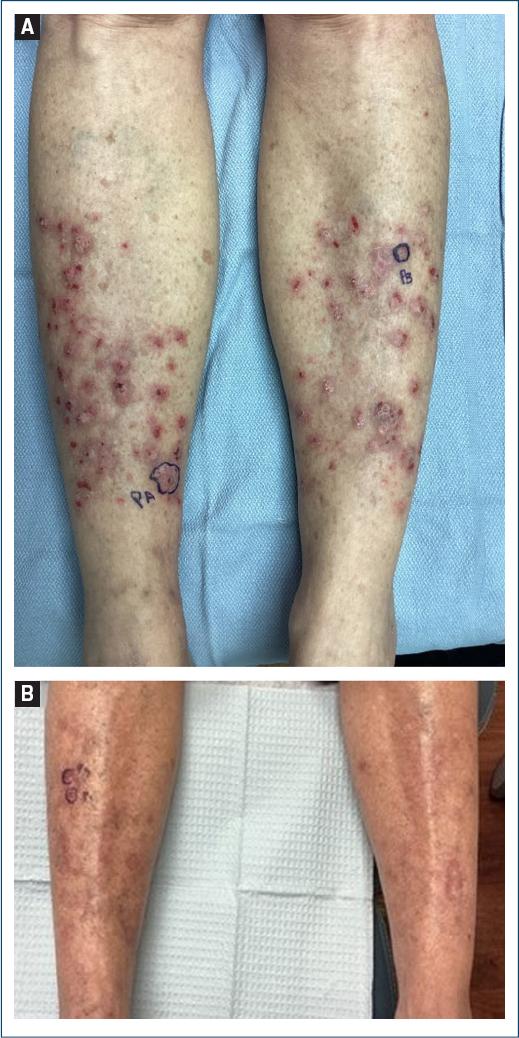
A 67-year-old woman presented with a 6-month history of > 50 erythematous plaques/nodules on her bilateral pre-tibial skin (Fig. 1A). The patient did not have any predisposing medical history or risk factors aside from having type II Fitzpatrick skin type. The lesions were tender and intensely pruritic. Concerning nodules were biopsied, with most demonstrating well-differentiated SCCs and others lichen simplex chronicus. The patient was diagnosed with pathergic SCCs. She was treated with our standard regimen of oral acitretin, 25 mg, 5 days/week, 0.1-0.5 mLs of 50 mg/mL intralesional fluorouracil weekly to biopsy-proven SCC, and 10-40 mg of intramuscular triamcinolone monthly. Lichen simplex chronicus was treated with triamcinolone 0.1% cream under occlusion and intralesional-triamcinolone. The patient was followed weekly until all SCCs resolved then transitioned to monthly visits. Acetretin was weaned to 10 mg with the goal of stopping once the patient remained cancer-free for 12 months. The patient tolerated the treatment regimen without side effects or signs of toxicity. At 8 months, only two stable non-malignant lichen simplex chronicus nodules remained (Fig. 1B).
Case 2
A 72-year-old woman presented with numerous erythematous keratotic nodules on her bilateral pre-tibial skin. She endorsed frequent trauma to this area. Concerning lesions were biopsied, all consistent with SCCs. The patient did not have any predisposing medical history or risk factors aside from having type II Fitzpatrick skin type. The patient was placed on a similar follow-up and treatment regimen of acitretin, intralesional fluorouracil, and intramuscular triamcinolone. Over the course of 3 years, 20 SCCs were treated with this regimen. The patient improved and remained SCC-free for 12 months prompting discontinuation of treatment. Within a month of stopping, the patient developed new lesions. An invasive SCC formed in the scar of a previous intralesional fluorouracil site. Mohs surgery was performed with negative margins (Fig. 2A). Two months afterward, the patient had prompt development of three new SCCs adjacent to the scar (Fig. 2B). The treatment regimen of intralesional fluorouracil was restarted with good response.

Discussion
The exact pathogenesis of pathergic SCCs remains unclear. Studies of pathergy favor an immune-mediated T-cell reaction, similar to a delayed-type hypersensitivity reaction, initiated through mechanically damaged epidermal and dermal components1,4. The reaction may vary depending on the involved condition, the type/severity of trauma, and ethnicity4.
Patients often describe chronic itching and recurrent trauma, including surgery. Pathologic changes may be initiated or exacerbated by external stimuli along with immune dysregulation, increased cell turnover, and microenvironment changes in the setting of chronic inflammation. The use of systemic steroid therapy in our treatment regimen stems from this intrinsic auto-inflammatory hypothesis. Moreover, SCCs has been observed to develop within other inflammatory disorders of the skin, including psoriasis, lichen planus, lichen simplex chronicus, herpes virus infections, and chronic wounds (Wolf’s isotopic response)5. The pathway to malignant transformation in these conditions is poorly understood6.
Treatment of benign pathergy-induced conditions is typically predicated on avoidance of additional skin trauma and amelioration of pruritus. Systemic, intralesional, and topical steroids are vital in halting the itch-scratch cycle seen with concomitant conditions such as lichen simplex chronicus/prurigo nodularis. The management of cutaneous malignancies, including SCCs, in this context, may pose a conundrum because traditional excision may not be suitable. In addition, patients in this setting often manifest with many lesions in poorly-perfused anatomic sites of the lower extremities6. Once pathergy is recognized, the non-surgical intervention appears to provide the best response in our experience. Besides intralesional injections of fluorouracil or methotrexate, many regimens also include systemic retinoids such as acitretin or isotretinoin. The rationale for the latter is that retinoids are known to affect epidermal turnover and keratinization. It is for this reason that they have also historically been used to manage psoriasis, another condition in which inflammatory, non-malignant, epidermal proliferation and pathergy occurs1-3. Aggressive combination therapy and close follow-up are necessary to properly manage this challenging clinical scenario.
Conclusion
Cutaneous pathergy represents a rare but significant mechanism in the development and propagation of eruptive squamous cell carcinomas, particularly in predisposed individuals with chronic inflammatory skin conditions or repeated trauma. The two cases presented underscore the diagnostic and therapeutic complexities of managing pathergy-associated SCCs, especially when arising on the lower extremities. Our experience highlights the utility of a nonsurgical, multimodal regimen combining systemic retinoids, intralesional chemotherapy, and corticosteroids to effectively control disease activity, reduce lesion burden, and manage underlying inflammatory triggers. Early recognition of this phenomenon is essential to avoid unnecessary surgical interventions, which may exacerbate the condition. As pathergic SCC remains an under-recognized entity, greater awareness and interdisciplinary collaboration between dermatologists, surgeons, and oncologists are crucial for optimizing patient outcomes in this challenging and often recurrent disease process.

