











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Nasal reconstruction after surgical excision carries substantial cosmetic relevance due to the central and highly visible position of the nose on the face1. Successful nasal reconstruction requires meticulous attention to color and texture match, contour, and the symmetry of nasal subunits2. Island flaps offer excellent color and texture compatibility as well as tissue conformity; however, the limited mobility of the nasal subcutaneous tissue often restricts their use2. Among the possible modifications of the island flap, the use of a unilateral myocutaneous pedicle has been described3. This unilateral pedicled myocutaneous island flap enhances flap mobility while preserving its reliable vascular supply4. Despite previous descriptions in the literature, case series focusing exclusively on unilateral pedicled myocutaneous island flaps for nasal tip reconstruction remain limited.
The surgical technique is described as follows. The procedure begins with identification of the lesion and surgical margins (Fig. 1A). The course of the facial artery and, subsequently, the angular artery can be visualized. Flap vascularization is provided by branches of the angular artery that accompany the fibers of the transverse nasal muscle (musculus nasilis, pars transversa).
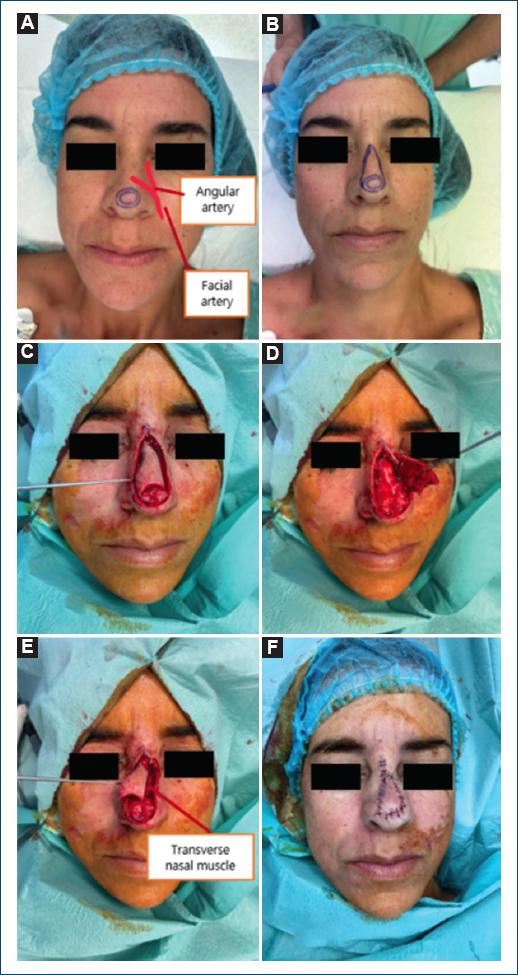
Figure 1 Corresponding to case 1. Surgical steps of the unilateral pedicled myocutaneous island flap for nasal tip reconstruction. A: pre-operative marking of the lesion and margins, with the anatomical course of the facial and angular arteries indicated. B: design of the triangular skin island superior to the defect. C: circumferential incision outlining the Island flap. D: creation of the deeper incision on the side opposite the pedicle, extending to cartilage or bone. E: identification and preservation of the transverse nasal muscle fibers forming the myocutaneous pedicle. F: final result after advancement and V-Y closure.
A triangular flap is then designed superior to the defect, ensuring that the base of the triangle corresponds to the defect diameter, while the flap length should measure approximately 3 times the defect diameter (Fig. 1B). An incision is made around the flap, creating an island configuration (Fig. 1C). Importantly, the incision along the side containing the intended muscular pedicle is limited to the subcutaneous tissue, thereby preserving muscle integrity. On the side opposite the pedicle, a deeper incision is made down to the nasal cartilage or bone, transecting the transverse nasal muscle (Fig. 1D).
Flap elevation is performed in two distinct planes: first, undermining of the lateral nasal wall ipsilateral to the muscular pedicle within the subcutaneous plane up to the nasofacial sulcus; second, undermining of the flap inferior to the transverse nasal muscle along the lateral nasal wall to the nasofacial sulcus.
The flap is then advanced to cover the defect (Fig. 1E), and closure is performed in a V-Y fashion (Fig. 1F).
Methods
This was a retrospective, observational, single-center study including clinical cases of surgical reconstruction of nasal tip defects performed over a 2-year period (2024-2025) at the Unidade Local de Saúde de Almada-Seixal. All reconstructions were carried out using a unilateral pedicled island myocutaneous advancement flap. Procedures were performed under local anesthesia on an outpatient basis, with no need for hospital admission.
Results
A total of five patients were included in this series, comprising four women (80%) and one man (20%). The mean age at the time of surgery was 63.8 years. One of the reconstructions was performed following tumor excision with Mohs micrographic surgery. Histopathological analysis was available for all five cases. In every patient (100%), the excised lesion corresponded to a basal cell carcinoma.
Case 1: A 41-year-old female with a basal cell carcinoma on the nasal tip. This case was used to illustrate the flap design in the introduction (Fig. 1). Primary closure would have generated excessive tension and an undesirable elevation of the nasal tip. An acceptable esthetic outcome was observed at 1 month postoperatively (Fig. 2).

Case 2: A 52-year-old female with a basal cell carcinoma on the nasal tip. Reconstruction was performed following Mohs micrographic surgery. A good esthetic outcome was documented at 2 months postoperatively (Fig. 3).

Figure 3 Corresponding to case 2. A: pre-operative identification of the lesion and surgical margins. B: intraoperative view demonstrating the intermediate stage of flap advancement using the unilateral pedicled myocutaneous island flap. C: final esthetic outcome at 2 months postoperatively.
Case 3: A 71-year-old female with a basal cell carcinoma on the nasal tip. A good esthetic outcome was achieved at 3 months postoperatively (Fig. 4).

Figure 4 Corresponding to case 3. No pre-operative photograph of the initial lesion is available. A: immediate post-operative appearance following reconstruction with a unilateral pedicled myocutaneous island flap. B: esthetic outcome at 3 months postoperatively.
Case 4: A 75-year-old female with a basal cell carcinoma on the nasal tip. An excellent esthetic outcome was obtained 2 months after surgery (Fig. 5).

Figure 5 Corresponding to case 4. A: pre-operative identification of the surgical margins and flap design. B: immediate post-operative appearance following reconstruction with a unilateral pedicled myocutaneous island flap. C: excellent esthetic outcome at 2 months postoperatively.
Case 5: An 80-year-old male with a basal cell carcinoma on the nasal tip. An acceptable esthetic outcome was noted at 3 months postoperatively (Fig. 6).

Discussion and conclusion
The unilateral pedicled myocutaneous flap is a variant of the island flap with excellent mobility and a reliable vascular supply provided by the angular artery, a branch of the facial artery1.
Myocutaneous pedicles broaden the indications for island flaps by enabling an alternative source of perfusion. However, their design and elevation are technically demanding2.
The main advantages of this flap include its robust vascularity, substantial mobility, and excellent color and texture match with the surrounding skin5, while generally avoiding undesirable elevation of the nasal tip1.
The main disadvantages relate to its geometric configuration, which may result in a more conspicuous scar.
In this case series, the mean patient age was relatively young (63.8 years), underscoring the need for meticulous attention to reconstructive planning and execution, particularly in esthetic subunits such as the nasal tip. Although the sample size is limited, the consistent post-operative outcomes across all cases support the reliability and versatility of this flap design. Our findings reinforce that this flap is particularly advantageous in younger patients or in those where distortion of the nasal tip must be minimized.
Overall, the unilateral pedicled myocutaneous island flap provides a reliable, safe, and versatile option for reconstruction of distal nasal dorsum and nasal tip defects, particularly when tissue mobility is limited and preservation of nasal contour is essential.

