











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Tubulointerstitial nephritis and uveitis syndrome (TINU) is a rare oculorenal inflammatory condition, whose pathogenesis remains unknown.1 An environmental factor may trigger an immune‑mediated response in an individual with a particular susceptible genetic background.2Both cellular and humoral immunity are thought to be involved. In most cases, TINU appears to be an idiopathic immune‑mediated process, sometimes apparently precipitated by drugs or infections.2 Renal prognosis of TINU is usually favorable, however recent studies have questioned this in the pediatric population.3 Controlling uveitis can be more challenging, leading to persistent uveitis or frequent relapses.2
CASE REPORT
A 12‑year‑old girl, previously healthy, presented with a month‑long history of asthenia, anorexia, weight‑loss (10% of total body weight), halitosis, occasional periumbilical pain, and sporadic vomiting, with no fever. Urine volume and color were normal. The patient denied taking any medication or drugs. Shortly before the beginning of symptoms, the patient had applied hair dye. The patient painted as a hobby and frequently mixed paints and paint thinners in an enclosed area.
On admission high blood pressure was detected (172/97 mmHg), with no other changes on physical examination. The patient had acute kidney injury, KDIGO 3 (serum urea 205 mg/dL; creatinine 14.4 mg/dL; glomerular filtration rate (GFR) 5 mL/min/1.73 m2), hyperchloremic metabolic acidosis (pH 7.28; HCO3‑ 11 mmol/L), normal potassium, calcium and phosphate, active urinary sediment (leukocituria, non‑nephrotic proteinuria, microhematuria and glicosúria). Microcytic hypochromic anemia (hemoglobin 9.5 g/dL) and elevated markers of inflammation (C reactive protein 11 mg/dL; erythrocyte sedimentation rate 76 mm/h) were identified. The patient was admitted to the pediatric nephrology unit and hemodialysis was per‑ formed for 10 days; during this time, diuresis was always preserved.
The kidney biopsy (Fig. 1) showed intense, diffuse, interstitial inflammatory infiltrate containing lymphocytes, neutrophils and eosinophils, with numerous tubules containing cellular detritus and neutrophils, suggestive of acute tubulointerstitial nephritis. Infections were excluded (HIV, hepatitis A, B, C and E, cytomegalovirus, Epstein Barr virus, adenovirus, herpes simplex I and II, Brucella, Bartonella, Rickettsia, Legionella, Toxoplasma, Chlamydia, Leishmania, Leptospirosis and Mycoplasma tuberculosis). Anti‑nuclear and anti‑dsDNA were negative. Complement levels were normal. Initial ophthalmologic exam was normal.
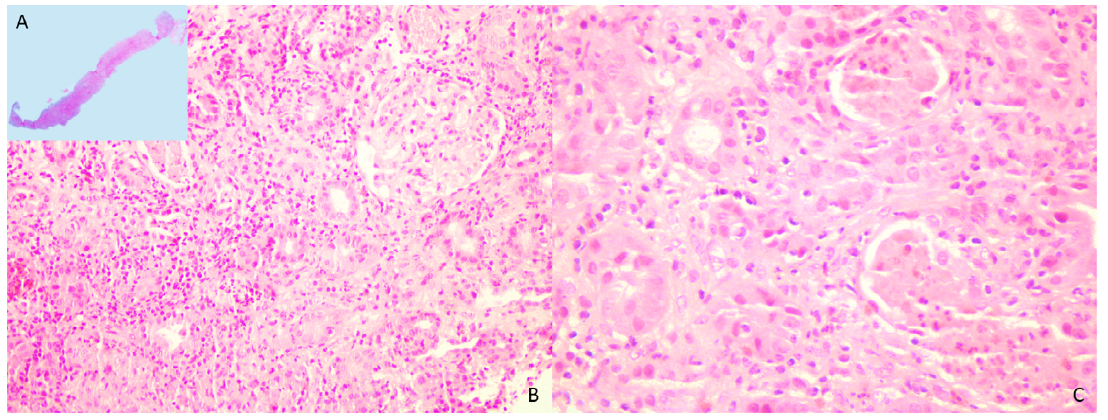
Figure 1. Histological sections of the renal biopsy, measuring 10 mm, which included only cortex with 6 glomeruli with no morphological changes (A‑H&E). A severe inflammatory infiltrated was diffusely present in the interstitium, composed of lymphocytes, neutrophils and eosinophils, scantily permeating the tubular epithelium (B‑H&E). Some tubules displayed degenerative changes, with cellular debris and presence of intratubular neutrophils (C‑H&E).
Oral prednisolone (80 mg/day, 0.85 mg/kg/day) was started (8 days after admission) and complete eviction of paints and hair dyes was recommended. Renal function improved progressively until discharge (18 days after ad‑ mission ‑ serum urea 145 mg/dL; serum creatinine 1.78 mg/dL; GFR 41 mL/min/1.73 m2) and during follow‑up as an outpatient. Prednisolone was slowly tapered.
Four months after the first symptoms, the patient developed eye redness, pain, photophobia and decreased visual acuity. The prednisolone dose at this time was 5 mg/day. Anterior bilateral uveitis was identified and the diagnosis of TINU was established. Eye inflammation persisted with topical steroids associated with systemic steroids. The patient started methotrexate (the dose was progressively increased up to 20 mg weekly subcutaneous), with no response. Resolution of eye inflammation was achieved after adding adalimumab (40 mg subcutaneous every 2 weeks with loading dose). Oral prednisolone was suspended 12 months after presentation. There was complete recovery of renal function after 17 months (serum urea 23 mg/dL; creatinine 0.64 mg/dL; GFR 110 mL/min/1.73 m2). The patient maintains normal renal function, normal urinary sediment, no proteinuria, normal blood pressure and absence of ocular inflammation with methotrexate (20 mg weekly) and adalimumab (40 mg every 2 weeks) two years after presentation.
DISCUSSION
TINU syndrome is defined as the occurrence of tubulointerstitial nephritis and uveitis in the absence of other systemic diseases.2,4
To date, the exact pathogenesis of TINU remains elusive; the current accepted hypothesis proposes that an environmental factor may trigger an immune‑mediated response in an individual with a particular susceptible genetic background.2 This immune mediated process may be triggered by drugs or infections, although in many cases no cause is identified (idiopathic TINU).5
This disorder is under‑recognized.5,6TINU is both a pediatric and an adult disease.4 There is a female predominance, although it is less pronounced in the pediatric population (55% females in the pediatric population); patients have being reported among most ethnic groups.1 Acute tubulointerstitial nephritis (AIN) often precedes uveitis.5 In the patient described, there was no inflammation on initial ophthalmologic examination, and uveitis was diagnosed 4 months later when the systemic corticosteroids where being tapered.
The AIN in TINU typically presents with fever, weight loss, fatigue and malaise.5 Other symptoms may be present, including anorexia, abdominal or flank pain, arthralgias or myalgias, many of which were present in this patient.5 The AIN in the context of TINU is often described as self‑limited and with a good prognosis, with patients rarely needing dialysis.5,7This was not the case in the patient reported.
Renal outcomes in children with TINU have been poorly described in the literature to date.3 In a cohort of 46 patients incomplete recovery of renal function (defined by an eGFR <90 mL/min/1.73 m2 and/or proteinuria and/or HBP and/or treatment with an antiproteinuric or antihypertensive drug) occurred in 76% at one‑year follow‑up, and in 63% at final follow‑up (median follow‑up of 2.8 years).3 Recurrent uveitis was not associated with poor renal outcome.3 The long‑term renal prognosis seemed to be strongly correlated with kidney impairment at di‑ agnosis.3 The patient described in this report, although presented with serious kidney impairment that required dialysis, had complete recovery of renal function after 17 months. In the same cohort patients with incomplete recovery of renal function at the final follow‑up already had a significantly lower eGFR at 1 year when compared with patients that had complete recovery of renal function, suggesting that the first few months after diagnosis are essential for the prognosis of kidney function.3
The role of steroids in the treatment of AIN has remained controversial, although they remain the mainstay of renal therapy in idiopathic AIN and TINU.8,9Multiple studies in adults have focused on this, with contradictory results.8 Pediatric studies are scarcer: a prospective study with 17 children with AIN (14 with uveitis) showed that prednisone sped up renal recovery, but there was no significant difference in renal function between groups after 6 months.10 The ideal doses and duration of steroid treatment are still up for debate.9 A retrospective study with 61 adults with drug‑induced AIN suggested glucocorticoids should be started within 2 weeks to avoid fibrinogenesis in the interstitium and permanent renal damage.11 Authors of another study with a cohort of 25 patients with biopsy‑proven acute tubulointerstitial nephritis (a subset of them with TINU) reported that the shorter the time period between the first symptoms and treatment with steroids, the better the renal function during follow‑up, suggesting that the timing of treatment is important for renal prognosis.12 Nevertheless, no evidence‑based criteria exist for the ideal timing of initiation, dose or duration of corticosteroid treatment for TINU.
Regarding ocular manifestations, TINU‑related uveitis typically develops between 2 months prior up to 14 months after the acute tubulointerstitial nephritis, but ocular symptoms may not always be present.2,5,13Asymptomatic uveitis occurred in up to 50% of patients in prospective studies.2 Ocular inflammation might be controlled with high doses of corticosteroids initiated because of the renal disease and occur with systemic corticosteroid taper or withdrawal, as was the case with this patient.2 Most patients with TINU have sudden‑onset non‑granulomatous bilateral anterior uveitis, characterized by redness, pain and photophobia, also consistent with this patient’s clinical picture.2 However, a broad spectrum of manifestations is reported in the literature, including posterior uveitis, panuveitis, and granulomatous anterior uveitis.2 Ophthalmologists must be alert to the possibility of TINU when confronted with a patient with uveitis. Blood pressure should be evaluated, and blood and urine tests should be performed.1
Although TINU affects children and adults, there are some differences between these two groups: children seem to have a more severe course of uveitis with more frequent relapses and are slightly less likely to develop acute kidney injury; on the other hand, adults more frequently develop chronic kidney disease.4 There is no known pathophysiological explanation for the increased relapse and possibly chronic course of ocular disease in children.4 So far, in this patient eye inflammation has remained controlled with methotrexate and adalimumab, and renal function remains normal. There were no relapses two years after initial presentation.
As TINU is a rare disease, treatment is not standardized, and controlling the uveitis can be challenging.2 Topical corticosteroids and cycloplegic agents are the first line treatment for anterior uveitis, however in the acute phase of anterior uveitis in TINU, up to 80% of patients will require systemic corticosteroid therapy.2,5It has been shown that in 70% of patients with TINU, systemic corticosteroid therapy does not seem to be sufficient to prevent recurrences of uveitis.14,15The next step in the treatment ladder for refractory disease and/or corticosteroid sparing effect is immunosuppressive therapy with methotrexate (MTX), mycophenolate mofetil or cyclosporine A.16 There is no reported significant difference in terms of therapeutic effectiveness of the different immunosuppressants.2 Methotrexate is the typical first‑line therapy in most pediatric patients with chronic non‑infectious uveitis, because it is well‑tolerated in children and has fewer side effects.16 A meta‑analysis of the efficacy of methotrexate in childhood chronic autoimmune uveitis revealed that approximately 75% of patients showed an improvement in intraocular inflammation with methotrexate.17 Biologics like infliximab or adalimumab play an important role in controlling refractory uveitis and can also be considered first line treatment in conjunction with methotrexate in children with severe uveitis at diagnosis. They should be used in conjunction with methotrexate to reduce the formation of drug‑neutralizing antibodies.16
Two major acquired risk factors have been proposed for TINU: drugs and infection. Among drugs, those that have been more frequently implicated are non‑steroidal anti‑inflammatory agents (NSAIDs) and antibiotics.1 However, a few issues exist when evaluating these associations between environmental risk factors and the onset of TINU: most of the studies focusing on TINU are retrospective and therefore subject to recall bias, the proposed risk‑factors are very common in the general population, and these risk‑factors may coexist making it difficult to assess their relative contributions.1,5,7
Acute interstitial nephritis has been associated with a wide variety of drugs, as well as with toxins and auto‑ immune diseases. Drug‑induced AIN is thought to have an immunologic base, a hypersensitivity reaction rather than resulting from direct toxicity from the drug.18 Notably, some drugs that have been associated with acute interstitial nephritis have not been linked to TINU (e.g. proton pump inhibitors), which might suggest a distinct pathogenic mechanism for ocular and renal injury among these different drug classes.1 Interestingly, drugs that are most frequently reported as potential causative agents for acute interstitial nephritis and TINU are not those that have strong evidence of causing isolated drug‑induced uveitis, suggesting differing mechanisms of induction of uveitis between isolated drug‑induced uveitis and TINU.1
Other toxic agents, such as hair dyes containing paraphenylenediamine (PPD) and industrial paint thinners, have been associated with kidney injury.19-21Our patient’s frequent contact with hair dyes and paint thinners raised the question of whether they had any role as a trigger for TINU in this case; however, the hair‑dyes used did not contain PPD and a cause‑effect cannot be established.
CONCLUSION
The prevalence of TINU may be underestimated, particularly among pediatric patients with acute interstitial nephritis, in whom uveitis may be asymptomatic. Therefore, it is important to raise awareness for this entity, which is heterogeneous not only in clinical presentation but also in its renal and ocular effects. In this patient the renal involvement was severe at presentation and renal replacement therapy was required, but there was a complete recovery of renal function with prednisolone treatment. The uveitis was only controlled with biologic agents but has been inactive during the last two years. A combined follow‑up of pediatric nephrology and ophthalmology is essential for the care of these patients.

