











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Rhizobium radiobacter is an aerobic, motile, non‑spore‑forming gram‑negative bacteria ubiquitous of the soil and an opportunistic pathogen to humans.1 It mostly affects immunocompromised individuals, including those with malignancies, transplant recipients, under immunosuppressive medication, with human immunodeficiency virus infection and end‑stage kidney disease.2 This agent can cause several types of infection, including catheter‑related infections, peritonitis in peritoneal dialysis (PD), urinary tract infections, endophthalmitis, endocarditis, pneumonia and brain abscesses.3 Its ability to adhere to silicone surfaces makes medical devices a risk factor for infection3,4yet, there are reports of infection in healthy individuals with no medical devices.2,3Despite the seriousness of these infections and the frequent need for medical device removal1, this agent has low virulence3 and a good prognosis when appropriate antibiotic therapy is timely initiated.1 In terms of antibiotic susceptibility, cephalosporin, piperacillin‑tazobactam, carbapenems and ciprofloxacin are some of the alternatives.1,2
It is well known that peritonitis is one of PD’s Achilles’ heel, contributing substantially to morbidity, mortality and technique drop out.5 The diagnosis requires at least two of the following findings: clinical evidence of infection (abdominal pain and cloudy fluid), dialysis effluent with a cell count over 100 cells per µL with more than 50% polymorphonuclear leukocytes and positive effluent culture.5 Most cases are caused by bacteria, 45%‑65% gram‑positive and 15%‑35% gram‑negative.6 According to the 2022 International Society of Peritoneal Dialysis (ISPD) guidelines, empiric antibiotic therapy should be started as soon as possible, covering both gram‑positive and gram‑negative organisms according to local sensitivity, and once antibiotic sensitivity test (AST) is known, antibiotic therapy should be adjusted. In terms of catheter removal, the guidelines recommend it when there’s a failure to clear PD effluent in five days of appropriate antibiotics (refractory peritonitis), with the option of a longer period of antibiotic therapy if cell counts are diminishing.5
We present a case report of a PD‑related peritonitis caused by Rhizobium radiobacter, the fourth case reported in Portugal.
CASE REPORT
A 36-years-old male presented to the emergency department (ED) with abdominal pain that started in the previous hours. He had a personal history of systemic erythematous lupus and stage 5 chronic kidney disease under automated PD with an extra exchange (“PD plus”), he was not taking any immunosuppression, had no technique-associated complications or soil contact. At presentation, he also mentioned new onset of cloudy fluid. His physical examination in the ED was noteworthy for generalized abdominal pain without signs of peritoneal inflammation and no inflammatory signs on the catheter exit site, he had a temperature of 37.7ºC, blood pressure of 152/101 mmHg, heart rate of 91 bpm and peripheral oxygen saturation of 100%.
His laboratory results showed no elevation of inflammatory parameters (leucocytes 3890/uL, reactive protein C 0.95 mg/dL) and peritoneal fluid analysis revealed 6688 polymorphonuclear (PMN) cells per mm3 (95% of total cell count). An abdominal radiography proved a well‑positioned catheter and an absence of subdiaphragmatic free gas. The patient was diagnosed with PD‑related peritonitis. Microbiologic samples of blood and peritoneal fluid were collected, and the patient was started empirically on intraperitoneal vancomycin and ceftazidime.
He was evaluated in the PD unit the next day, with an improvement of both the symptoms and PMN count on the effluent fluid (Fig. 1). He was reevaluated three days later, maintaining cloudy fluid despite improvement of abdominal pain and cytologic values. On day five after the symptoms started, Rhizobium radiobacter was isolated in the effluent fluid, but no AST was provided, given the lack of AST breakpoint for this agent in both the European Committee on Antimicrobial Susceptibility Testing and Clinical and Laboratory Standards Institute guidelines. Vancomycin was switched to oral ciprofloxacin and ceftazidime was continued, according to the literature available.
Five days after the change in antibiotics, the patient maintained abdominal discomfort, cloudy fluid and recrudescence of PMN on the effluent (PMN), meeting the criteria of refractory peritonitis and indication for PD catheter removal. On day ten after symptom onset, the catheter was removed, and oral ciprofloxacin and intravenous ceftazidime were kept for another 14 days.
The patient remained on hemodialysis with a tunneled catheter for a year by choice and returned to PD after that period.
DISCUSSION
Rhizobium radiobacter PD‑related peritonitis poses both a diagnostic and management challenge since it is a rare pathogen, with only 32 published cases, capable of adhesion to medical devices and without AST breakpoints in both the European Committee on Antimicrobial Susceptibility Testing and Clinical and Laboratory Standards Institute guidelines. These characteristics make the antibiotic choice difficult and rely on a literature review, composed mostly of case reports.
The first case report of PD‑related peritonitis caused by Rhizobium radiobacter dates 1985,8 since then more case reports have come to light, three of which from Portugal.4,9The most recent literature analysis dates 2022 and compiles 16 reports of one or more cases.6 We have identified five more cases previous to 2022 not included in this analysis,8-11and, since 2022, two cases have been published.12 In total, there are 23 articles and 32 cases of peritonitis due to Rhizobium radiobacter, including ours (Table 1).
Table 1 Clinical cases of peritonitis in peritoneal dialysis patients caused by Rhizobium radiobacter
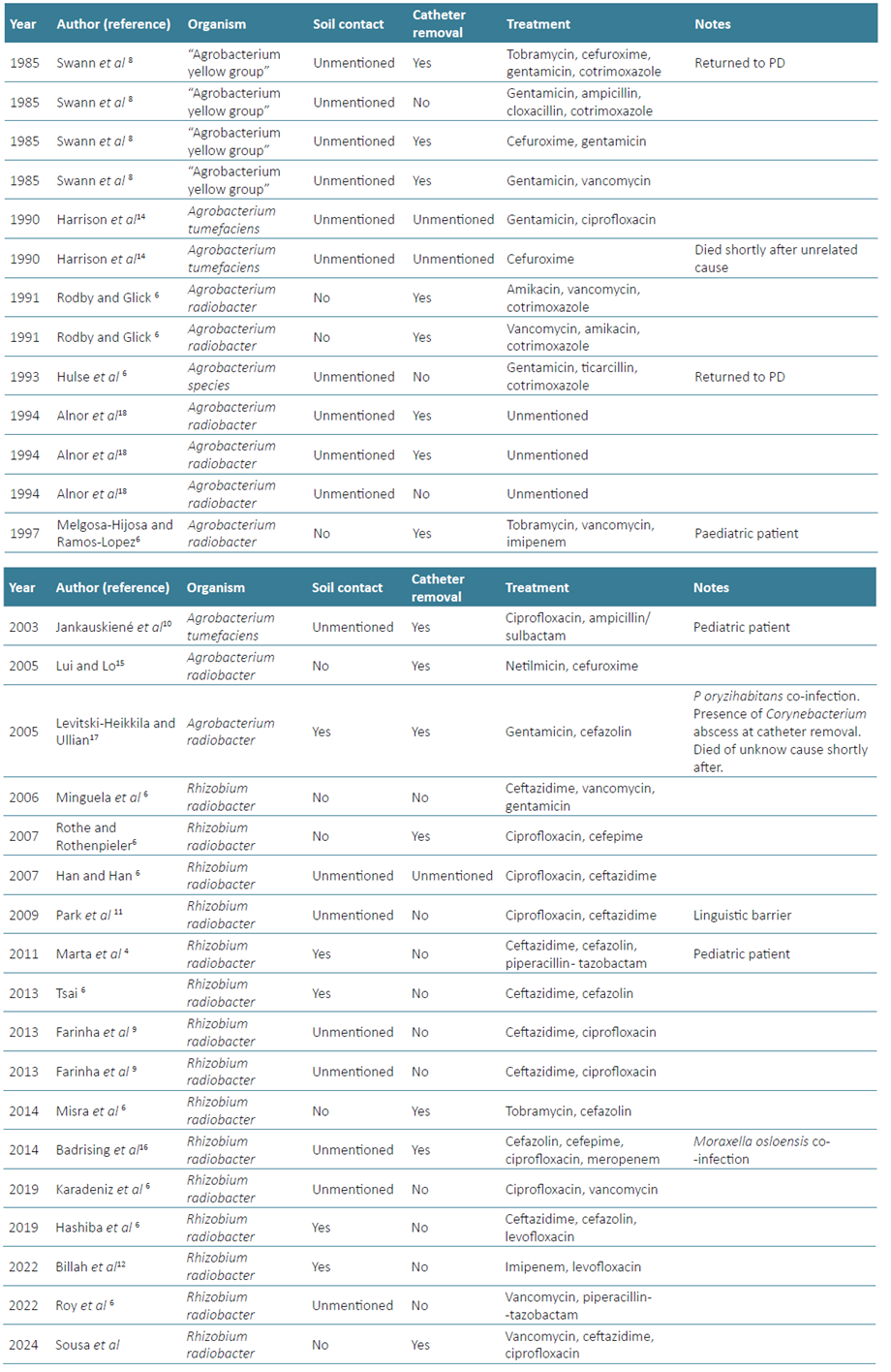
Unlike most of the other published cases, we were not provided an antibiogram of this agent. Only Karadeniz et al were not provided with an antibiogram, they started the patient on empirical intraperitoneal vancomycin and oral ciprofloxacin with good clinical response, completed a 14‑day antibiotic course and were able to keep the catheter.13 We based the decision to switch vancomycin to ciprofloxacin on the fact that Rhizobium radiobacter is a Gram‑negative agent in the available literature, and we also took antibiotic stewardship into consideration. Monotherapy was attempted in only one of the published cases,14 and considering the available literature, it becomes clear that most of the patients who kept the catheter were treated with a cephalosporin and fluoroquinolone, so ciprofloxacin added to ceftazidime.
In our case, given the maintenance of symptoms and rise in effluent’s PMN after ten days of antibiotic therapy, five of which with appropriate antibiotic therapy, we decided to remove the catheter, based on the ISPD guidelines.5
Given the frequent relapses even after initial antibiotic response and appropriate antibiotic choice,6,15catheter removal was frequently required (n=15, 47%). Yet, there are also a substantial number of reports where it was possible to maintain it (n=14, 44%). The differences in other risk factors, antibiotic resistance and initial antibiotic choice, as well as the route of administration, previous antibiotic pressure and the simultaneous isolation of other agents,16-18may be why catheter maintenance varies so greatly amongst authors.
Interestingly, despite being a ubiquitous bacterium of the soil, in 21 of the 32 published cases, it is not mentioned whether the patient has had soil contact (66%). Considering the ones in which it is mentioned, soil contact was present in five of the 11 cases, suggesting the importance of this factor to raise suspicion for this infection.
In summary, the number of PD-associated peritonitis caused by Rhizobium radiobacter rises each year, reinforcing the need for AST breakpoints and clinicians’ awareness of this agent, especially those dealing with PD patients. Combined antibiotic therapy using cephalosporin and fluoroquinolone seems to be the best treatment option when AST is not available. Although catheter removal was common when this agent was first identified, given the frequent relapses, almost half the patients were able to keep the catheter. Further literature analysis of sensitivity testing and antibiotic duration is important to establish the best practice when dealing with this agent.

