











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Chronic kidney disease (CKD) is a global health problem that affects millions of people around the world.1 As a progressive disease, it poses physical, emotional and psychological challenges. Therefore, CKD requires a comprehensive dimension of care beyond the one provided by conventional medicine.2 Spirituality has emerged as a way of providing patients with a sense of purpose and connection throughout their illness. In healthcare, spirituality encompasses more than religious beliefs. It involves a search for meaning, purpose and transcendence in the patient’s life, as well as an experience of connection with oneself, others, nature or a higher power.3 This review highlights the importance of addressing spirituality in the treatment of patients with CKD and its role as a fundamental element of palliative care. By an analysis of the overlap between spirituality and CKD, this article attempts to demonstrate the way in which spiritual care is able to increase patient wellbeing, improve quality of life and inform a holistic, compassionate and holistic palliative care practice.
DEFINING SPIRITUALITY
Since the beginning of Medicine, spirituality has been an integral part of the treatment process. In Hammurabi’s code (18th century BC), one can read that “healing depends on holiness, law, herbal words and knife”. As science evolved over the centuries, it began to supplant what previously belonged to the unknown and was only explained by the divine, the spiritual, and the transcendent. Technical specialization and the growth of scientific knowledge have increasingly put spirituality aside in the treatment process. However distant from scientific and technological evolution, spirituality remains a profound and exclusively human experience, resulting from the combination of personal contexts, beliefs, neuro‑sensitive experiences, perceptions, cultures, and personal determinants. Spirituality also persists as a strong predictor of acceptancy and illness management and possesses therapeutic benefit, potentially impacting outcome.
Nevertheless, why is it so difficult to define spirituality?4 Historically, spirituality takes us to religiosity, beliefs and rituals that frame the interior experience in terms of seeking meaning and comfort on a journey of faith toward a higher being. However, in its diversity of expressions, it does not need to be exclusively related to religion. Spirituality can be, and is, a way of understanding and relating with the world, a mechanism for personal knowledge and a path for inner pacification.3 Many definitions for spirituality have been proposed, “spirituality can be understood as a search for the sacred, a process through which people seek to discover, hold on to, and, when necessary, transform whatever they hold sacred in their lives”,5or, “Spirituality is the personal quest for understanding answers to ultimate questions about life, about meaning, and about the relationship to the sacred or transcendent, which may (or may not) lead to or arise from the development of religious rituals and the formation of community”6or even, “Spirituality exists in testing and experiencing the depth of inner peace consistently”, Amit Ray. However, more important than looking for a consensual definition of spirituality, analysing its dimensions allows us to obtain a more precise interpretation of what it can be. It is a profoundly human characteristic, expressed individually, based on personal beliefs, practices, and experiences related to the desire for peace, connection, meaning, interpretations of life, and personal growth. It leads to the development of positive inner values and feelings.4 , 7 , 8By assuming this complexity of spirituality as an integrated human characteristic, healthcare science must highlight the importance of spirituality in the care of CKD patients.9A research by Kimmel et al emphasized the association between spiritual well‑being and better health outcomes, including improved quality of life and lower levels of depression and anxiety among CKD patients undergoing hemodialysis.8Also, Davison and Jhangir underscored the significance of spiritual beliefs and practices in helping patients navigate the complexities of CKD treatment, fostering a sense of meaning, acceptance, and peace amid illness-related challenges.10
ASSESSING SPIRITUALITY
In order to draw up a holistic care plan in any area of medicine, in particular in nephrology, it is essential to have a good knowledge of the patient, including their spiritual side.10 Since spirituality is a deep and personal subject, the healthcare provider needs to establish a relationship of trust with the patient, which requires sensitivity, empathy, understanding and tolerance.
Conversations can take the form of simple questions about the patient’s religious preferences or more structured spiritual stories led by chaplains. Open‑ended questions can also be used, allowing patients to fully express their spiritual beliefs and experiences. Patients who do not follow an organized religion can be asked questions such as: “What gives your life meaning?” or “How do you see your role in the overall scheme of society?” There are several well‑known tools that can help with these assessments, each with its advantages and limitations. The FICA Spiritual History7 and the SPIRITual History11 offer structured approaches to exploring the patient’s spiritual beliefs, the meaning of faith in their life, and how these elements affect their coping mechanisms. These tools help guide discussions about how illness affects the patient’s spiritual well‑being. The following figures summarize the essential spiritual assessment tools, highlighting their characteristics, strengths and limitations. These tools are often used in medical practice to respond to patients’ spiritual needs and support holistic care.
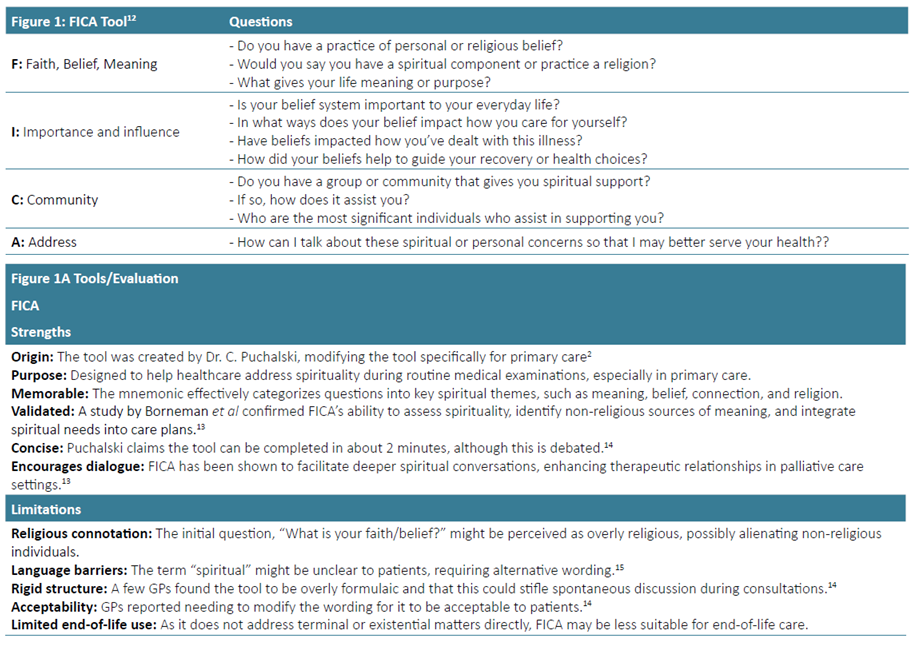
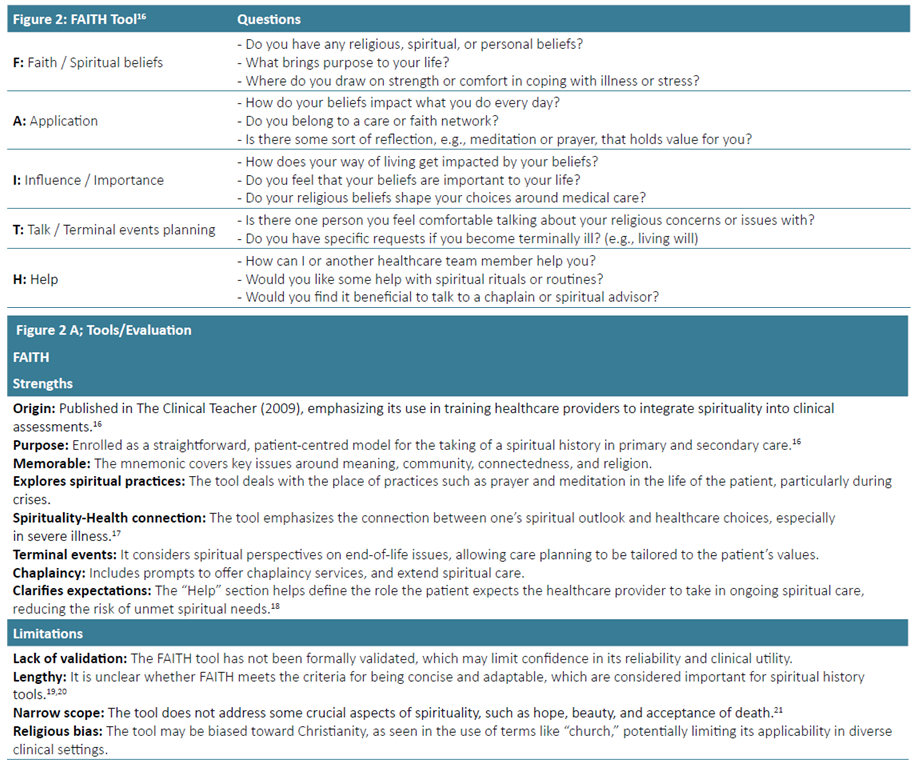
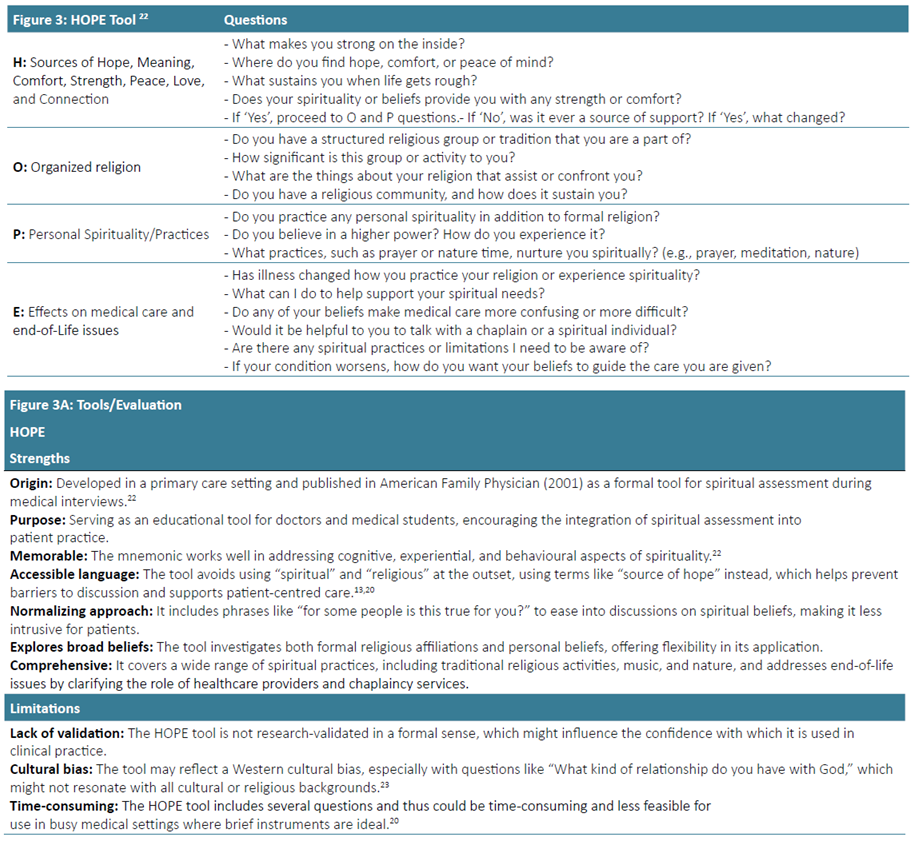
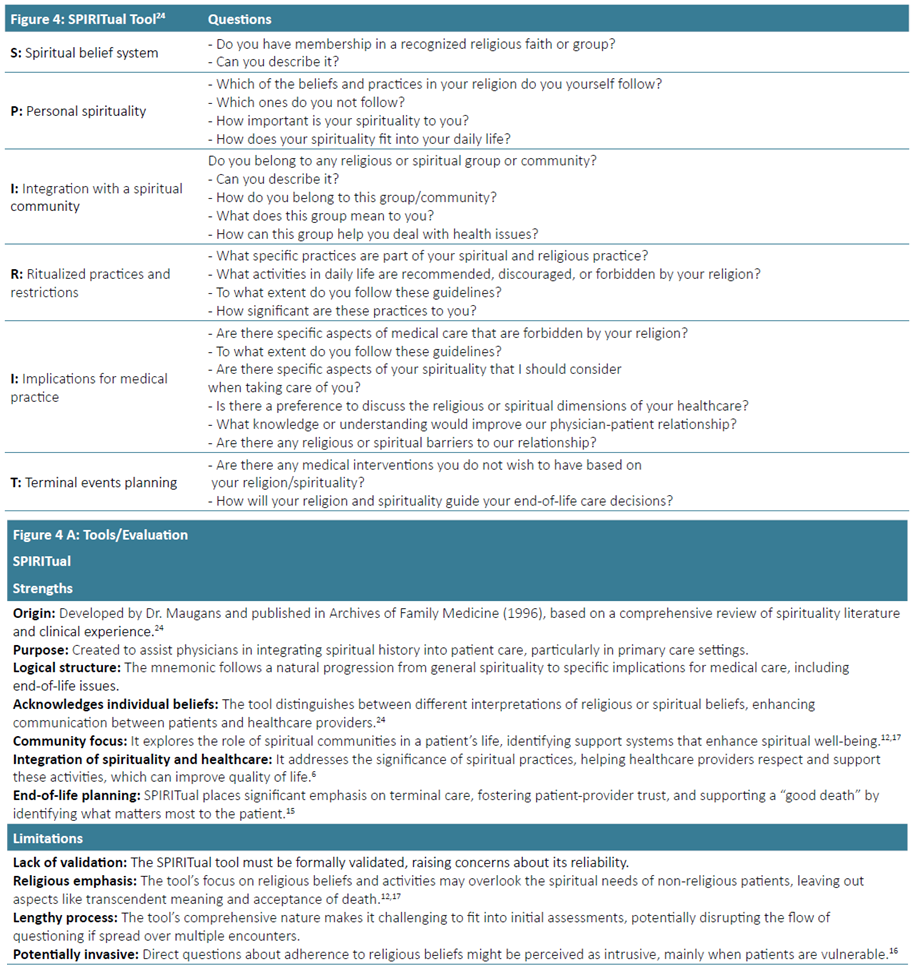
The figures above show different spiritual assessment tools, each with unique strengths that are appropriate for different aspects of nephrology care. The FICA Spiritual History is useful for quick assessments and can be seamlessly integrated into patient interactions once a trusting relationship has been established.7 On the other hand, the SPIRITual History, with its comprehensive examination of a patient’s spiritual beliefs, provides a wealth of information.11 While administering it effectively may require more time and a higher level of expertise, healthcare professionals can feel more informed and prepared when using this tool. Far from being mere formalities, spiritual assessments should be viewed as powerful tools to initiate meaningful dialogues. These conversations can explore how patients are coping with their illness, the personal transformations it has triggered, and their evolving self‑perceptions and relationships. As Hudson and Rumbold underscore,25 these tools should be used to assess and affirm the significance of spirituality in daily healthcare. This ensures that spiritual issues are not overlooked but are instead acknowledged and addressed as a crucial part of the patient’s overall care plan. While these tools are vital in identifying the spiritual needs of CKD patients, their true value is realized when the clinician applies them with empathy and cultural sensitivity. When used effectively, these tools guide the development of care plans that holistically address the physical, emotional, and spiritual dimensions of patient care in nephrology. This approach ultimately enhances the quality of life for patients facing chronic kidney disease, underscoring the significant role of the clinician in patient care.
SPIRITUAL NEEDS IN PATIENTS WITH CHRONIC KIDNEY DISEASE
Spirituality is an increasingly recognized domain for patients with chronic kidney disease (CKD), with clear importance to this patient population. Davison et al, in a prospective cohort analysis involving 327 CKD patients, found that a significant portion of these patients experience profound spiritual distress, with over two‑thirds reporting at least one spiritual need. Common concerns included finding hope, meaning in life, and peace of mind. These spiritual needs were not limited to any specific demographic group, suggesting that all CKD patients may have unmet spiritual needs. By routinely assessing and addressing these spiritual concerns as part of comprehensive CKD care, healthcare providers can significantly improve patient’s quality of life and support their emotional and psychological well‑being during the challenges of chronic illness, thereby underscoring the importance of their role in patient care.10
The studies cited show the importance of a holistic approach in which the spirituality of patients and their caregivers is considered alongside the physical and psychological care of CKD. Spiritual assessments are essential as part of routine care, allowing caregivers to ensure that the patient’s emotional and spiritual needs are met and thus improve the overall well‑being of the patient and their family, who are also affected by CKD.26
SPIRITUALITY, QUALITY OF LIFE, AND MOOD
Quality of Life (QOL) is a broad concept that includes not only physical health, but also social connections and purpose in life, as well as mood problems such as anxiety and depression. Patients with CKD often exhibit low QOL, displaying elevated levels of anxiety and depression.
Studies show that approximately 20% to 50% of individuals with CKD are affected by depression and the higher level of depression leads to increased morbidity and mortality.27,28Spirituality in patients with other chronic illnesses was found to improve quality of life (QOL) and lower levels of depression and anxiety. However, the information about spiritual care in patients with CKD is quite limited. A study from Finkelstein et al indicated that spirituality plays a crucial role in both groups, the spiritual well‑being of CKD patients on dialysis and cancer patients being comparable.29
In a study with CKD patients, in particular those in dialysis treatment, Watnick et al showed that depression is more severe than in cancer patients, revealing the heavy psychological burden of living with a chronic disease requiring life-sustaining treatment.30 For those reasons, CKD patients, benefit more from spiritual care that helps them to maintain hope and well‑being throughout their lives. On the other hand, spiritual care in cancer patients, is more important for end‑of‑life preparation and reconciliation.
The above findings are supported by the review from Murtag et al, demonstrating that in CKD patients’ anxiety and depression are more dominant than in patients with cancer, due to the prolonged nature of CKD treatment and its profound effect on decreasing patient´s quality of life.31
SPIRITUALITY AND CLINICAL OUTCOMES
In patients with other chronic illnesses, spirituality is associated with lower mortality and rehospitalization,32 but there is less evidence in patients with CKD.
Like other chronic illnesses, in CKD, spirituality appears to be associated with a lower risk of mortality. The study by Spinale et al, found that higher levels of spirituality were significantly associated with improved survival among hemodialysis patients. Specifically, patients with higher spirituality scores had a 51% lower risk of mortality. The study suggests that the beneficial effects of spirituality on survival may be partially mediated by increased social support.33Faith is a concept closely related to spirituality and religion, yet distinct, given it is a more personal, subjective, and deeper relationship to hope and, for some, to God.34A longitudinal study by Bruce et al using data from 3558 CKD patients over a long period, aimed at investigating the impact of religion on the mortality of CKD patients. Results show that patients attending religious events at least once per week exhibit a lower risk (about 21%) of all‑cause mortality, indicating that regular participation in religious acts should have a positive effect on survival This beneficial effect of spirituality is further enhanced for patients in treatment compliance in end-stage renal disease (ESRD).35 Freire de Medeiros et al highlighted that religiosity was positively correlated with adherence to dialysis sessions among hemodialysis patients, illustrating how spiritual practices can reinforce commitment to life‑sustaining treatments.36 Moreover, Fradelos et al demonstrated that spiritual well‑being among ESRD patients undergoing hemodialysis is in general, moderate but displays wide variations depending on each individual’s profile. Several other factors have also influence such as place of residence, marital situation, educational degree, and how strongly is patients believe in God.37
SPIRITUALITY ACROSS THE STAGES OF KIDNEY DISEASE
Spirituality is essential along the journey for patients with CKD and ESRD. It provides vital support through the progression of the kidney disease from early stages to dialysis, potential transplantation, and finally in the end‑of‑life care. When kidney starts to fail, spirituality often acts as a key source of emotional strength and purpose, which is a precious help for the patients to deal with the anxiety and depression that commonly result from a serious diagnosis.35,38For patients who had a kidney transplant, spirituality continues to be vital in the healing process. In addition to physical recovery, patients have complex emotional reactions such as gratitude to the donor, anxiety and ethical questions about receiving an organ from another human being. These are deep personal feelings, where spirituality often provides tools to face the associated emotions, promoting acceptance and resilience.39,40Spirituality also tends to influence adherence to post‑transplant routines, as patients will view their health maintenance as a means of honouring the gift they have received.40 Spirituality is an important part of the final stages of life as an important means of support and comfort, not only for patients but also for their families. It also provides guidance when families face difficult decisions about treatment options and at the challenging time of end‑of‑life planning. It also promotes acceptance, comfort and closure at the end of life. 10
SPIRITUALITY AND CAREGIVER SUPPORT
Caregivers, as being the main caretakers, but also facilitators and promoters of physical, psychological and social support gained increasingly more importance in healthcare systems. Social and governmental recognition of informal caregivers was an important step to guarantee that those who choose to assume this role are, somehow, supported. These caregivers are many times, close family members who dedicate a substantial part of their lives taking care of the patient. Caregivers gain more importance as chronic illness increases, as patients become more fragile, dependent, and incapable of taking care of themselves, and as fewer institutions become capable of responding to all the needs arising from these chronic conditions. In chronic disease, particularly CKD, in addition to medical consultations and exams, hemodialysis treatments, or even hospital admissions, there is a huge need for daily out‑of‑hospital care, which includes medication management, adapted nutrition, mobility, hygiene care, physical comfort and monitoring psychological distress. Caregivers find themselves, many times, enrolled in an emotional and psychological challenge as they must support the patients with constant availability, empathy, and love. Through this, sentiments of anxiety, exhaustion, burnout, and stress are very common among caregivers.5 This is the context where spirituality can play a significant role in providing support to both patients and caregivers.2 Spirituality can be a strong connection tool between caregivers and patients, as an important and therapeutic weapon to be used in consonance with clinical and personal care.9 By having a more profound knowledge of the patient, caregivers can become vectors of resilience and coping mechanisms in order to help face this challenging disease. It can provide a sense of well‑being, bring purpose and meaning through all disease path phases, increase vital strength‑both physical and emotional‑ reduce stress, prevent burnout and engage compassionate care and ethical conscience, bringing together patients and caregivers.43 Spirituality could also promote an approach to caregivers and patients with more extensive community support, through group networks
On the other hand, from the perspective of the caregiver himself, spirituality strategies can bring comfort, strength and hope, becoming important self-caring resources and providing emotional support for self‑pacification in their caregiving role.41,42
The spiritual dimension can also enable the caregiver to pacify the patient when dealing with end‑of‑life decisions, for example, stopping haemodialysis, managing expectations and emotionally preparing patients and their families for the terminal illness and end of life - the most common fear among CKD patients and caregivers45,46and even mourning after death.
FUTURE DIRECTIONS
Realizing that spirituality is a powerful therapeutic weapon is as urgent as necessary. In this perspective, it becomes important to create awareness to integrate physical care with spiritual care in healthcare facilities. 48As a future perspective, we propose the following points as emerging pillars to take into account when building a more effective offer in the spirituality field:
1) Holistic patient-centred care: only with a complete understanding of the human being that transcends not only the disease and its implications, but also a comprehensive approach to the patient’s fears, desires, beliefs, and aspirations, could one offer an effective treatment for chronic disease and suffering by acting in different human dimensions.47
2) Multidisciplinary integrated care: training and building teams that comprehend transdisciplinary approach with clinical professionals and promoters of spiritual well‑being (religious, mindfulness, meditation, arts, among others) capable of guaranteeing physical and spiritual support, will improve patients’ acceptance of the disease, adherence to treatments and reduce anxiety, sadness, pain or other manifestations of suffering.
3) Spiritual assessment tools: development of questionnaires or other tools that measure spiritual dimensions and assess their impact on well‑being, in the context of chronic disease, which would help define a patient’s therapeutic plan by integrating these results into clinical decisions.43 The definition of a potentially measurable vital sign as “spiritual well‑being level” would allow for assessing the need for intervention or evaluating the response rate to proposed spiritual interventions.
4) Awareness and recognition: implementation of training programs on spirituality to create an open culture and empower professionals, caregivers, and family members on how to approach and ensure that spirituality is also integrated and respected in the patient’s therapeutic process.
These four pillars seek to broaden the horizons of those who care, to a more attentive and deep knowledge of human suffering dimensions. It is from this comprehensive, focused, and empathic approach to the patient, that ideas and actions could born, creating more therapeutic perspectives, and integrating spirituality as a powerful and effective weapon, to help chronic kidney disease patients.
CONCLUSION
We live in an unprecedented era of technological advancement, where medical breakthroughs and artificial intelligence provide excellent tools for managing advanced diseases such as CKD. However, even during this cyber revolution, it is clear that patient care is about much more than technology. The human touch, compassion, and spirituality are indispensable tools for those suffering. Literature shows that responding to the spirit‑connecting us to the meaning of life‑ improves the quality of life, reduces anxiety, and improves the relationship between healthcare providers and patients. True excellence in healthcare comes from integrating technology and humanity, science and compassion, reason and transcendence. And no machine can ever replace a gesture of presence, a listening ear, or a shared hope.

