











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
The global obesity epidemic presents substantial challenges in healthcare, notably in renal transplantation, where it significantly impacts patient management and outcomes. With obesity rates having tripled since 1975, more than 650 million adults worldwide suffer from obesity, complicating the eligibility and surgical management of kidney transplant recipients.1-3 This rising prevalence is mirrored in kidney transplant waiting lists, increasing not only the number of potential recipients but also complicating their clinical management due to associated comorbidities.
Obesity significantly impacts the clinical outcomes of kidney transplantation, reflecting in both the surgical risks and long-term viability of the graft.4-6The literature provides substantial evidence of the negative implications of obesity on transplant success rates, patient recovery, and long-term health management post-transplantation. Studies have consistently shown that obesity is associated with an increased risk of surgical complications. Scheuermann et al reported that obese recipients experience a higher rate of wound infections and delayed wound healing, directly impacting the immediate postoperative recovery period.7 Additionally, these patients exhibit a 1.5 times higher rate of delayed graft function compared to those with normal BMI, complicating early post-transplant management. The long-term outcomes for obese transplant recipients are equally concerning. Foucher et al. highlighted that obesity increases the risk of graft loss by approximately 20% within five years post-transplant.8 Similarly, Hill et al conducted a meta-analysis indicating that each unit increase in BMI above 30 kg/m² is associated with a 10% increase in the risk of graft failure and mortality over the long term.9
The increased incidence of post-transplant diabetes mellitus (PTDM) and cardiovascular diseases in obese recipients is well-documented.10,11Gadwal et al noted that obese recipients are more likely to develop PTDM, which can significantly affect overall patient health and graft survival. Cardiovascular complications remain the leading cause of mortality in transplant recipients, exacerbated by pre-existing obesity.
The management of obesity in kidney transplant candidates is comprehensively addressed in several clinical practice guidelines, which recommend tailored interventions to mitigate the risks associated with high BMI12-14: Developing Education Science and Care for Renal Transplantation in European States (DESCARTES) and Kidney Disease Improving Global Outcomes (KDIGO) Guidelines: These guidelines advocate for pre-transplant assessments that include cardiovascular evaluations and diabetes screening, recommending a reduction in BMI to below 30 kg/m² through lifestyle modifications, pharmacotherapy, or surgical interventions.15
European Renal Best Practice (ERBP) Guidelines: The ERBP guidelines suggest structured weight loss programs for candidates with a BMI over 35 kg/m², including possible bariatric surgery to ensure BMI reduction before transplant eligibility assessments. They also emphasize the importance of monitoring nutritional status to prevent deficiencies due to aggressive weight loss measures.16 Kidney Health Australia (KHA-CARI) Guidelines: These guidelines highlight that effective obesity management is essential, stating that while obesity should not automatically exclude patients from transplant consideration, it must be adequately managed to reduce post-transplant complications and improve transplantation success rates.17With a varying degree of non-uniform recommendations across the most recent guidelines, it often comes to each specific transplantation center to ascertain their own criteria and obesity management strategies. In our center, patients with obesity are encouraged to lose weight and given access to a multidisciplinary obesity management program to reach the cut-off criteria of BMI over 35 kg/m2 which excludes them from transplantation until further weight loss is achieved.
Traditional bariatric surgeries, such as gastric bypass and sleeve gastrectomy, have been commonly used to manage obesity in kidney transplant candidates. Gastric bypass surgery typically results in significant weight loss, often exceeding 30% of total body weight. However, it carries a risk of nutritional deficiencies and requires long-term nutritional monitoring.18 Sleeve gastrectomy, while slightly less effective in terms of total weight loss (about 25%-30% of total body weight), tends to have fewer complications and a shorter recovery time.19 Both procedures, however, involve significant alterations to the digestive system, which can complicate post-transplant medication regimens. Both surgeries have demonstrated efficacy in reducing comorbid conditions associated with obesity, such as hypertension and type 2 diabetes, which are critical in post-transplant health management.20 However, the invasive nature of these surgeries introduces risks such as leaks, infections, and long-term complications like malabsorption and vitamin deficiencies, which can impact the patient’s overall health and the success of the transplant. Furthermore, there may be a significant risk of immunosuppressant pharmacokinetic modifications related to these procedures as bypass-type of surgery induces malabsorption and decreased enterohepatic circulation, while the opposite is true in sleeve gastrectomy leading to increased concentration and decreased clearance of immunosuppressive drugs.5
A less invasive alternative, the endoscopic sleeve gastroplasty (ESG), has emerged as a promising alternative to traditional bariatric surgery for managing obesity.21,22ESG involves suturing the stomach from the inside to reduce its volume but does not remove any stomach tissue or alter the gastrointestinal anatomy. It has been shown to result in significant weight loss, about 15%-20% of total body weight, which is less than that achieved with traditional surgeries but with considerably lower risk and shorter recovery time. Importantly, ESG does not interfere with the absorption of medications, which is a crucial consideration post-transplant.23
Given its efficacy, safety profile and reversibility, endoscopic gastroplasty might be considered as the procedure of choice as a bridge to renal transplantation in patients with obesity. In this paper, besides proposing a protocol of ESG as bridge to transplantation we will also provide our own comparative data between laparoscopic sleeve and endoscopic sleeve to justify the latter’s use in this context.
Primary objectives
In this prospective single-center study, we propose a minimally invasive endoscopic approach for patients with end-stage kidney disease (ESKD) suffering from obesity as per the latest European (ESGE) and American (ASGE) Gastrointestinal Endoscopy societal guidelines.24 With this approach, we aim to assess the extent of weight loss and BMI change after ESG in this population as well as post-transplant complications such as:
Early complications, including delayed graft function (defined as needing at least one dialysis session within the first week after transplant), initial non-function, acute rejection, surgical site infection, wound dehiscence, perirenal hematoma, lymphocele, procedure duration and length of hospital-stay;
Late complications, including PTDM, hypertension, chronic rejection and hospital readmissions.
We will then retrospectively analyze previously transplant-ed patients that fit the inclusion criteria but were not sub-jected to ESG or any other obesity management strategy (control group), thus providing a population-match basis for the same metrics and statistical comparison to assert the extent of benefit from pre-transplant recipient obesity management.
Secondary objectives
These include the assessment of ESG failure to achieve significant weight loss as defined by loss of <5% of total body weight (%TBWL) and/or <25% of excess body weight (%EWL) as per ASGE’s guidelines on endoscopic bariatric procedures.25 If ESG failure is noted, we will then proceed to analyze the need for synergist use of glucagon-like peptide 1 (aGLP1) agonists and/or need for redo ESG or even conversion into laparoscopic sleeve gastrectomy on a case-by-case basis via multidisciplinary evaluation. Ultimately, we also aim to determine safety by monitoring procedure-related severe adverse events (SAEs), hospital stay, operative mortality and cause related mortality.
METHODS
Study design
This is a single-center, prospective cohort trial conducted at Unidade Local de Saúde Santa Maria, focusing on adult patients with ESKD and obesity with BMI range from 30 to 42 kg/m2, who will undergo ESG as bridge to renal transplant surgery. Recruitment, over a 2-year period, will begin in May 2025 and conclude in April 2027. All eligible patients will be followed for a minimum of 6 months after ESG before being recommended for transplantation if desired weight loss has been achieved. Follow-up will then mimic usual renal transplant patient’s post-operative assessment with clinical, biochemical, and imaging modalities being employed.
Study population
We plan to include individuals of adult age (minimum of 18 years of age) with ESKD and obesity with BMI ranging from 30 to 42 kg/m2. Despite the institutional cutoff of 35 kg/m2 for kidney transplant eligibility it has been proven that patients with obesity grade I, BMI 30 - 34.9 kg/m2, although transplant eligible, still benefit from structured weight loss programs leading to lower acute surgical complications as well as exerting a significant impact on graft longevity. Therefore, our aim is two-fold, not only to be able to include patients previously outside the cutoff for transplantation but also to improve transplantation results in patients with mild obesity. In addition, patients must be willing to undergo multidisciplinary evaluation and follow-up by the center’s multidisciplinary obesity team comprised of surgeons, endocrinologists, gastroenterologists, nutritionists and psychologists and comply with proposed behavioral modifications. Each patient has to obtain approval by all aforementioned groups as well as undergo an upper GI endoscopy with negative biopsy results for Helicobacter pylori or, in case of positivity, eradication has to be performed and a subsequent urea breath test with negative results has to be present in order to be considered eligible for inclusion. Patients with large hiatal hernias (>3 cm), gastroesophageal reflux symptoms, active peptic ulcer disease and previous oncological abdominal surgery are excluded (Fig. 1). Women of childbearing potential should have a negative urine beta human chorionic gonadotropin pregnancy test. All patients must be able to fully understand and give writ-ten informed consent.
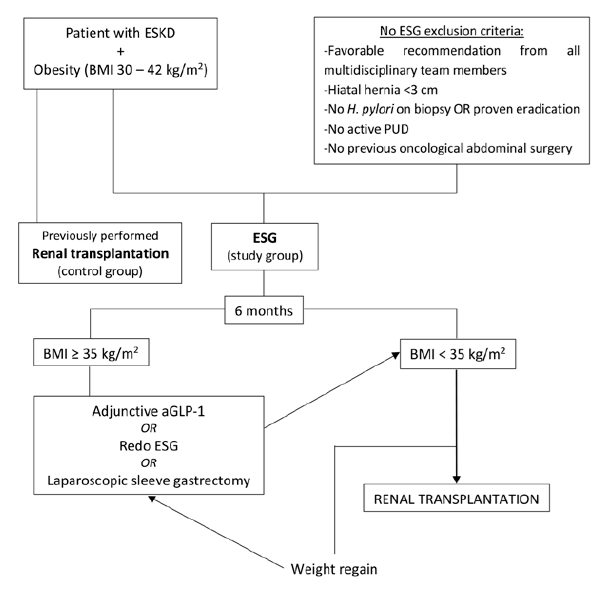
Study algorithm
Patients eligible for inclusion will undergo endoscopic gas-troplasty (Fig. 1) with a calculated necessary recruitment of 13 patients for this study group, which will then be compared retrospectively with previous renal transplant procedures performed on patients with obesity at our in-stitution. After ESG, patients will enter an obesity-related follow-up phase with regularly scheduled appointments with the nutritionist and endocrinologist, as well as the attending surgeon at 1 week, 1 month, 3 months and 6 months post-procedure. At this point weight loss and BMI change will be assessed with special consideration for those patients who had initial grade II obesity or grade III (up to 42 kg/m2). If the new resultant BMI is found to be less than 35 kg/m2 these patients will be referred for a kidney transplant and enter and new transplant-related follow-up according to already established institutional protocols.
If at the 6 months mark there was failure to achieve sufficient weight loss as defined by new BMI of more than 35 kg/m2 these patients will be considered on a case-by-case basis for adjunct synergistic therapy with GLP-1 agonists if only mild further weight loss is needed or referred for redo ESG or laparoscopic sleeve gastrectomy if moderate to severe weight loss is still in demand to meet the established cut-off or there has been significant weight regain. After successful weight loss has been established, patients will re-enter the transplantation route and resume normal follow-up.
Statistical analysis
Data analysis was conducted using SPSS software version 26 and G*power software version 3.26
The Shapiro-Wilk test was applied to all variables under study to assess normality of distribution. Nominal variables were expressed as absolute values and percentages and compared using the Pearson’s chi-square test with post-hoc correction according to Fisher’s exact test. Numerical variables were expressed as means ± standard deviation, if normally distributed, and subsequently compared with recourse to independent samples t test. Numerical data found to be non-parametric was expressed as median (minimum - maximum) and compared using the Mann-Whitney U test.
A p-value of < 0.05 was considered statistically significant. Sample size calculation was based on Cohen et al27 findings regarding the adjusted odds ratio (aOR) of 0.53 for delayed graft function outcomes of kidney transplant recipients who underwent bariatric surgery before transplant, compared to controls who have not. A rough approximation method to estimate Cohen’s d from the given odds ratio using the formula: yielded an effect size of 1.15. Sample size calculations were then computed into G*power software with alpha of 0.05 and power of 0.8 which resulted in a total sample size of 26 patients, which in an allocation ratio of 1:1 would lead to an n of 13 for each study arm.
The same process was repeated for Buemi et al28relative risk (RR) of 1.93 for delayed graft function in obese kidney transplant recipients, reaching an effect size of 1.19, which when plotted into G*power with the same assumptions, came to an equal total amount of 26 participants. A propensity score matching strategy will be employed between the retrospective control group and the prospective cohort in order to improve the study’s internal validity.
PROCEDURE
An institutional protocol is already established, and all patients will follow the same steps, being admitted to hospital the night before the procedure and completing a 6-hour solid food fasting and 2-hour clear liquids fast beforehand. Proton pump inhibitors are also started pre-operatively and a one-time 8 mg dexamethasone bolus administered pre-operatively along with 2 g cefazolin. The procedure is carried out in an operating room under general anesthesia. With the patient securely intubated and positioned in the supine position, an initial diagnostic upper endoscopy is performed to confirm that no findings belonging to the exclusion criteria are found. Next, an overtube is inserted over the scope and the OverStitch6 device (Apollo Endosurgery, Austin, TX) coupled to an Olympus double channel therapeutic endoscope is passed to the stomach with CO2 insufflation.
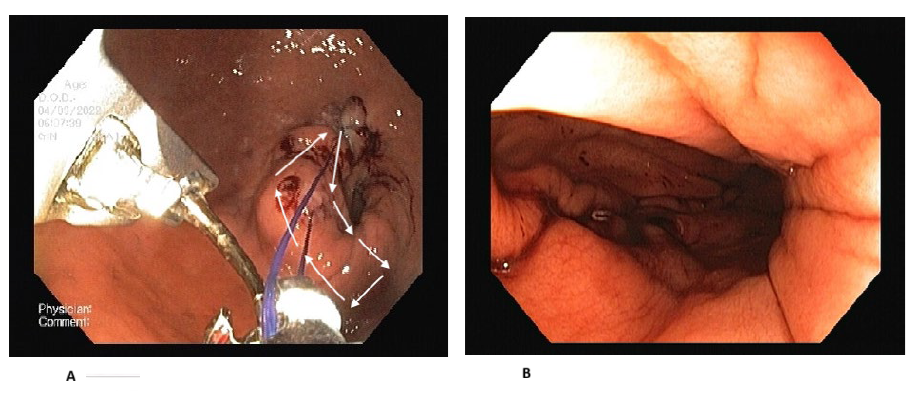
Transmural, full-thickness suturing, using 2-0 polypropylene material, is started at the level of the incisura angularis, following a square-shaped pattern from the anterior wall to the greater curvature and posterior wall before turning back to the region of the first stitch application. After the first suture is applied, a z pattern suture is applied along the greater curvature to shorten it. Two to three more square sutures are applied to the body of the stomach until the body-fundus transition is reached, with a total application of 4-6 sutures (Figs. 2A and 2B). At the end of the procedure, the over-the-scope device is removed, and another diagnostic upper endoscopy is performed to confirm patency of the gastric lumen and to perform gastric lavage.
Post-operatively, patients are medicated with standard intravenous analgesia using paracetamol and antiemetics such as ondansetron. All patients are kept overnight and discharged the next day in the absence of adverse events, having received dietetic advice from the nutritionist.
Pre‑trial procedure choice analysis
As the application of ESG as a bariatric and metabolic bridge for kidney transplantation has not yet been thoroughly investigated, we conducted an internal review of weight-loss results, severe adverse events and associated length of hospital stay for both endoscopic and laparoscopic sleeve previously performed in our center for patients living with obesity who were not candidates for kidney transplant. A 6-month follow-up was considered as the endpoint of this interim analysis due to adequate weight loss across the population at study at this time. We also believe that this endpoint, besides potentially providing enough weight-loss to draw benefit for kidney transplant recipient will also cause minimal impact in further delaying patient access to transplantation.
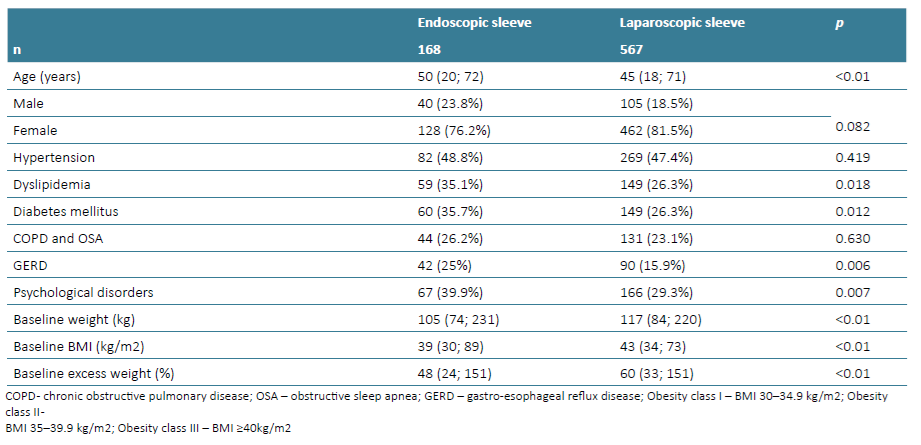
Regarding sleeve gastrectomy, 567 consecutive patients with obesity underwent this procedure in an outpatient setting as per institutional and departmental protocol between 2019 and 2022. Cases were retrospectively analyzed and the occurrence of staple-line leak was identified in 20 of those patients (Tables 1 and 2). As for ESG, 168 patients were prospectively operated between 2021 and 2024 under a similar institutional protocol with 3 serious adverse events (gastric perforation with extramural suturing of the abdominal wall) being identified (Tables 1 and 2).
RESULTS
The first patient will be enrolled in May 2025 and results are expected by April 2027.
As for the results of our interim analysis regarding procedure selection based on 567 patients submitted to laparoscopic sleeve gastrectomy and 168 who underwent endoscopic sleeve gastroplasty, we observed a significant difference in age with a median age of 50 (20; 72) in the ESG group compared to 45 (18; 71) in the laparoscopic sleeve group (p<0.01). Gender distribution was skewed towards female but homogenous between groups (p=0.082) (Table 1).
Regarding comorbidity analysis, ESG patients were found to carry significantly higher numbers of coexisting conditions like dyslipidemia (p=0.018), diabetes mellitus (p=0.012), gastroesophageal reflux disease (GERD) (p=0.006), and psychological disorders like depression and anxiety (p=0.007). Differences in prevalence of arterial hypertension and chronic obstructive pulmonary disease (COPD) with or without obstructive sleep apnea (OSA) between groups were found to be non-significant with p=0.419 and p=0.630, respectively.
Baseline weight-related metrics were all significantly different (p<0.01) with the ESG group presenting median initial weight of 105 (74; 231) kg, median initial BMI of 39 (30; 89) kg/m2 and median excess body weight of 48 (24; 151) % while for the surgical sleeve group median initial weight was 117 (84; 220) kg, baseline median BMI was 43 (34; 73) kg/m2 and median excess body weight of 60 (33; 151) % (Table 1).
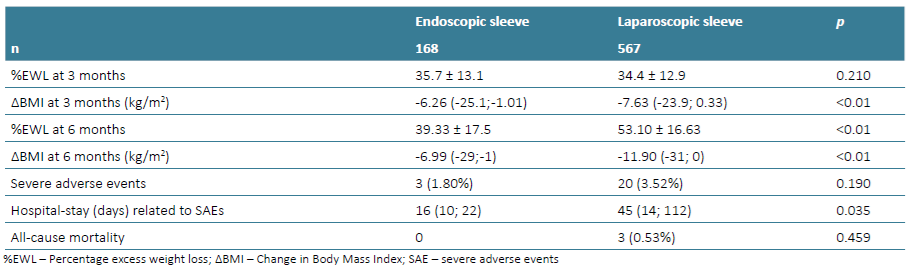
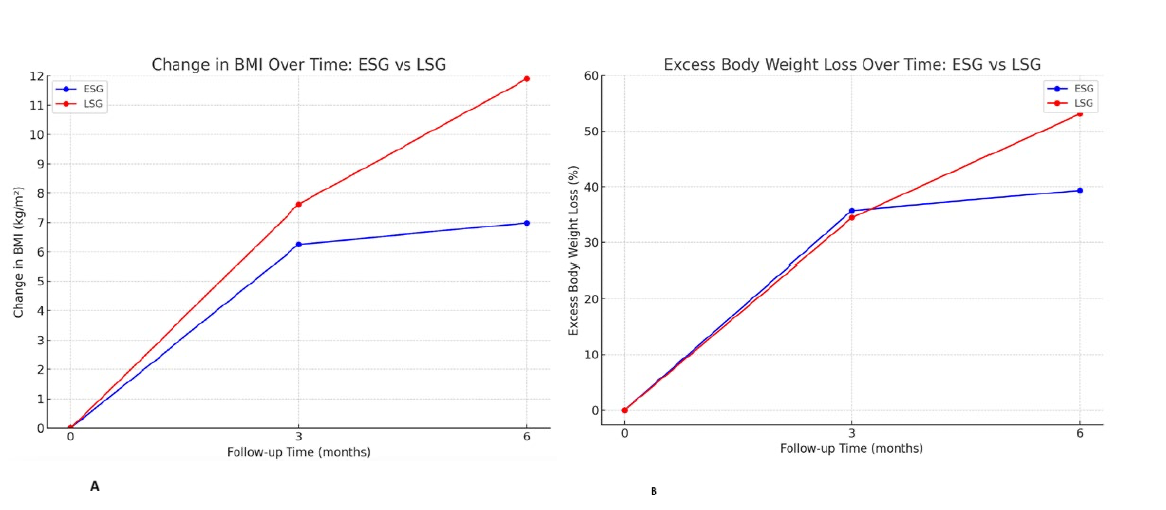
Excess weight loss (EWL) and BMI change were calculated at 3 and 6 months post-operatively with %EWL at 3 months showing no difference between the groups with mean of 35.7 ± 13.1% for ESG and 34.4 ± 12.9% for the laparoscopic group (p=0.210). BMI change at during the same period revealed a median loss of -6.26 (-25.1; -1.01) kg/m2 in the endoscopic procedure group and -7.63 (-23.9; 0.33) kg/m2 in the laparoscopic group (p<0.01) (Figs. 3A and 3B, Table 2). At 6 months the mean %EWL and BMI change for ESG was 39.33 ± 17.5 and -6.99 (-29; -1) kg/m2 respectively while for the laparoscopy group the same metrics were 53.10 ± 16.63 and -11.90 (-31; 0) kg/m2 (p<0.01) (Figs. 3A and 3B, Table 2).
Severe adverse event (SAE) occurrence in the endoscopic procedure in the form of gastric perforation with extramural suturing of perigastric structures was observed in 3 (1.80%) while SAE for the laparoscopic sleeve in the form of staple line fistulas were accounted in 20 (3.52%). Despite non-significance in SAE occurrence rate (p=0.190), the associated hospital stay for each group revealed significance with median of 16 (10; 22) days for ESG and 45 (14; 112) days for sleeve gastrectomy (p=0.035) (Table 2).
DISCUSSION
The proposed study addresses a significant unmet need in the pre-transplant optimization of patients with obesity and end-stage kidney disease. Obesity is a well-recognized barrier to renal transplantation, not only increasing perioperative morbidity but also impacting long-term graft survival and patient mortality.3,7-9Despite mounting evidence, there remains a lack of standardized strategies for managing obesity in this population, with transplantation centers often left to define their own eligibility criteria and weight loss pathways.12,14Endoscopic sleeve gastroplasty presents an innovative and minimally invasive approach that may overcome several limitations associated with conventional bariatric surgery. Compared to laparoscopic sleeve gastrectomy, ESG offers a superior safety profile, a shorter recovery period, and no significant impact on the pharmacokinetics of immunosuppressive drugs, a critical consideration in the post-transplant setting.5,6
Our interim analysis, comparing ESG with LSG in a non-transplant candidate population, reinforces ESG’s viability with short-term results at 3 months being identical in terms of weight loss. While LSG achieved greater absolute BMI reduction and percentage of excess weight loss at six months, ESG demonstrated a significantly shorter hospital stay in cases of severe adverse events (SAEs), whose occurrence was also less frequent despite not reaching statistical significance. These findings are consistent with recent systematic reviews and expert consensus reports advocating ESG as an effective alternative to surgery in selected patients.1,6The retrospective control cohort in this study allows for a critical comparison against historical transplant outcomes in obese patients who did not undergo any structured obesity intervention. Prior literature has shown that the absence of pre-transplant weight management strategies correlates with an increased incidence of delayed graft function, wound complications, and long-term graft failure,3,7-9which will be contrasted to the results obtained by this trial. The proposed BMI inclusion ranging from 30 - 42 kg/m2 stems from our internal analysis of ESG weight loss results which showed a median BMI change of -6.99 (-29; -1) kg/m2 at 6 months post-procedure. Hence, the maximum allowable BMI for inclusion of 42 kg/m2, in order to confidently predict acceptance for transplant wait-listing. By facilitating BMI reduction to below the transplant eligibility threshold (35 kg/m²), ESG could significantly enhance transplant accessibility and improve post-transplant outcomes in those already eligible but laden with obesity. Moreover, the inclusion of glucagon-like peptide-1 (GLP-1) agonists as adjunctive therapy in ESG non-responders introduces a scalable and pharmacologically supported alternative before resorting to more invasive options.
Recent consensus guidelines support the synergistic role of GLP-1 agonists in enhancing weight loss when endoscopic therapies fall short of efficacy targets.24,25Beyond weight loss, ESG may confer metabolic benefits that translate into lower risks of post-transplant diabetes mellitus and cardiovascular events; two leading causes of morbidity in this population.10,11ESG-induced weight loss has been associated with improved glycemic control, lipid profiles, and blood pressure regulation, all of which may synergistically reduce transplant-related complications. While ESG yields slightly lower weight loss percentages compared to surgical options, its favorable risk-to-benefit ratio and its ability to be performed without anatomical disruption make it an attractive bridge strategy. It may also allow for repeat procedures or reversibility, characteristics that are of particular importance in a population with chronic illness, polypharmacy, immunosuppression and potential future need for abdominal surgeries.6,21
This protocol not only proposes ESG as a viable intervention but also integrates a structured follow-up with potential pharmacologic escalation, endoscopic revision and surgical conversion pathways for either failure to achieve significant weight loss or in case of weight regain, thus reflecting a patient-centered approach to obesity management. This tiered model of care is aligned with recommendations from the DESCARTES, KDIGO, ERBP, and KHA-CARI guidelines, which all emphasize individualized, multidisciplinary strategies.10,13,16,17
Limitations of this study include the non-randomized design and the reliance on retrospective controls. However, the defined inclusion criteria, rigorous follow-up, and comprehensive adverse event monitoring strengthen the study’s internal validity. The two-year recruitment period and planned long-term follow-up will provide robust data on the durability of weight loss, transplant eligibility achievement, and post-operative outcomes.
In conclusion, this study has the potential to reposition ESG as a transformative, minimally invasive modality that can significantly reduce barriers to transplantation for people with ESKD living with obesity. Should the outcomes support our hypothesis, ESG could be integrated into pre-transplant evaluation pathways, ultimately improving equity and outcomes in kidney transplantation.

