











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Disasters can be characterized as potentially traumatic events that have individual, political, and community impacts, generate stress, and are experienced collectively (McFarlane & Norris, 2006). Disasters can have different natural, human, and/or technological causes (McFarlane & Norris, 2006) and characteristics. However, crisis-inducing events share common features including sudden onset, being unpredictable and uncontrollable, involving significant destruction, human loss and/or suffering, and exceeding the coping capacity of the community they affect (Math et al., 2015). More importantly, disasters are considered such when they involve loss of life (and traumatic grief), threats to life, injury and fear, the experience of horror, and loss of finances, property, and resources (Norris & Wind, 2010).
As an epidemiological condition, such as infectious diseases, the term pandemic is defined with a wide geographical area that has several characteristics, such as the movement of the disease, high rates of contagion and explosiveness, minimal immunity of the population, novelty level, infectiousness, and contagiousness (Morens et al., 2009). For example, the new coronavirus-19 disease [COVID-19] is caused by infection with severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2] which includes the characteristics of a pandemic (Morens et al., 2009).
The COVID-19 pandemic can, therefore, be conceptualized as a disaster in the sense that it is a crisis-triggering event experienced by a significant number of individuals (Duan & Zhu, 2020) and communities, with severe consequences for individuals, families, communities, societies, governments, and economies (Benight et al., 2010; Duan & Zhu, 2020; Hoffman & Kruczek, 2011; Norris & Wind, 2010; Raphael & Maguire, 2010). Thus, understanding how individuals cope with this experience is critical to addressing current and future mental health challenges resulting from the pandemic.
In terms of post-disaster adaptation, there are two possible approaches: (1) identifying needs and returning to pre-disaster reality, and (2) identifying risk and protective factors for future negative events (Pérez-Sales et al., 2005). Focusing on the second point, interventions should consider strategies to prepare people for the challenges of disaster and strengthen them in the case of future events (Jacobs et al., 2016; Marsella et al., 2008; Reifels et al., 2013). Therefore, mental health must be at the forefront of interventions, not only in terms of symptom relief but also with the goal of long-term adaptive functioning and positive development (Cox & Perry, 2011; Raphael & Maguire, 2010; Shing et al., 2016). The importance of one’s self-perceptions of coping skills, self-management of emotions, effective decision-making, coping, resilience, hope, optimism, and self-esteem has been widely highlighted to post-disaster adjustment outcomes (Benight et al., 2010; Luthar et al., 2000; Morgado, 2020; Norris et al., 2002; Schulenberg, 2016) and in their importance in the meaning-making processes (Norris & Wind, 2010; Park, 2016; Schulenberg, 2016). Moreover, positive adjustment after a crisis has been associated with empowering individuals to take an active role in their recovery process (Morgado, 2020).
Some socio-demographic factors have been identified as risk or protective factors for higher levels of stress in the event of a disaster. For example, being female has been identified as a risk factor, as have lower income and education levels (Norris et al., 2002). In terms of age, middle-aged adults tend to be more affected than younger and older adults due to the stresses and roles of this developmental stage; that is because the amount of support they tend to provide in a disaster situation is significantly higher than the amount of support they receive (Norris et al., 2002). Middle-aged adults are often faced with the demands of their children, their parents, and their multiple roles, relationships, and careers, thus making them a particularly stressed cohort in everyday life (Barrett et al., 2014). Naturally, this influences how they respond to disasters. Middle-aged adults need to deal with the effects of a disaster on themselves in addition to the effects on their marital, parental, and child relationships, as well as their financial security and difficulties in the community (Norris & Wind, 2010). This makes this group more vulnerable to negative trajectories following a disaster. Other issues have been raised regarding the COVID-19 pandemic, including concern for specific groups, such as the elderly and patients with chronic illnesses, who may be particularly vulnerable to more severe forms of SARS-CoV-2, isolation, and lack of appropriate care if their caregivers are infected or need to be isolated (Rajukmar, 2020).
Family-related factors such as marital status, being a parent, and exposure to the plight of family members are also important to consider (Norris et al., 2002). Indeed, research has indicated that marital status can influence individuals differently. On the one hand, being married can cause stress due to concerns with one’s spouse. Oppositely, not being married may constitute a risk for stress due to a lack of intimate sources of support (Morgado et al., 2021; Norris & Wind, 2010). Having children has also been associated with a higher risk for mental ill-being, with mothers particularly at higher risk due to concerns about the safety and well-being of their children (Norris et al., 2002). However, a recent study in the context of COVID-19 found that having dependents was associated with better perceptions of quality of life (Morgado et al., 2021).
In the context of the COVID-19 pandemic, professionals at risk of infection are particularly vulnerable to traumatic stressors. Indeed, uncertainty about virus contagiousness and treatment effectiveness (Duan & Zhu, 2020; Zhang et al., 2020) along with the challenges associated with being infected or in contact with infected individuals (i.e., social isolation, stigma, discrimination; Rajukmar, 2020), may put all workers who interact with the public at higher risk of poorer mental health outcomes.
Although it is possible to identify some risk and protective factors concerning the COVID-19 pandemic, the definition of risk or protection should depend on the specific circumstances. Protective factors in one circumstance for a particular outcome may not be protective for another outcome or circumstance (Luthar et al., 2000). In this sense, it is important to expand the understanding of processes affecting vulnerable individuals in the current crisis due to the COVID-19 pandemic.
The transactional model of stress and coping (Lazarus, 1966, 1999) conceptualizes stress as a transaction between an individual and the environment in which they are situated. Such transactions include the cognitive, physiological, affective, and motivational systems. According to this model, the stress response arises from an individual’s cognitive appraisal of the environment or context (Folkman et al., 1986; Folkman & Lazarus, 1980, 1986, 1988). Accordingly, the experience of stress occurs across three distinct processes: (1) primary appraisal (perception of a threat to oneself), (2) secondary appraisal (preparation of a possible response to the threat), and (3) coping (execution of that response) (Folkman, 2012; Folkman et al., 1986; Folkman & Lazarus, 1980, 1986, 1988). In the research field of coping with stressful events, coping is described as a person’s “efforts to manage specific external and/or internal demands that are appraised as taxing or exceeding the resources of the person’’ (Lazarus & Folkman, 1984, p. 141). The specific study of coping strategies during stressful events, such as chronic or life-threatening illnesses or natural disasters involves describing and identifying how people think and what behaviors they exhibit during these stressful events (Carver, 1997; Carver et al., 1989).
According to the Behavioral Self-Regulation model (Carver, 1997; Carver et al., 1989; Carver & Scheier, 2000, 2012; Scheier & Carver, 1988), behavior is directed towards goals through a feedback process known as self-regulation. Thus, when individuals experience stressful events, they employ coping strategies to self-regulate their emotions and affect through a feedback loop (Carver et al., 1989). Carver and colleagues (Carver, 1997; Carver et al., 1989) have proposed a categorization of coping styles that acknowledges whether they are adaptive or maladaptive. Adaptive coping, which is viewed as the more effective way to manage stressful events includes active coping, seeking socio-emotional support, seeking instrumental support, positive reframing, planning, and acceptance. Maladaptive coping, which is considered a less effective style of dealing with stressful events, includes self-distraction, denial, substance use, behavioural disengagement, venting, and self-blame (Carver, 1997; Carver et al., 1989). Although Carver (1997) did not originally categorise religion or humour as either adaptive or maladaptive coping strategies, Meyer (2001) categorised both as. According to Folkman (2012), this distinction between adaptive or maladaptive coping strategies is controversial because there are situations in which individuals do not have control over the problem and, under these circumstances, strategies focused on coping with the emotion may be more effective than strategies focused on problem-solving.
Viral illnesses, such as severe acute respiratory syndrome, are not novel. Previous studies of this particular type of illness have shown that individuals exposed to the risk of viral infection developed anxiety-related disorders and psychological maladjustment (Lee et al., 2007; Mak et al., 2009). Moreover, studies of past health-related pandemics, such as the 2009 H1N1 pandemic, indicated that individuals with higher levels of intolerance to uncertainty also exhibited higher levels of anxiety, and this was mediated by cognitive appraisals and adopted coping strategies (Taha et al., 2013). Stress and psychological maladjustment occur when threats to well-being are appraised, particularly when individuals perceive that they have no control over events due to heightened levels of uncertainty associated with the situation and stressor (Folkman et al., 1986), such as the case for a viral infection pandemic. Therefore, difficulties in emotion regulation, and consequently the use of less effective coping strategies to deal with stressful events, have been associated with psychopathology, psychological maladjustment, and poorer quality of life (Aldao et al., 2010; Knowles et al., 2020; Kring & Sloan, 2009; Meyer, 2001). According to Epifanio et al. (2021), quality of life decreased significantly during the COVID-19 outbreak in Italy, and the authors suggest that the sudden change in habits, the lock-in period, uncertainty, and health concerns may contribute to this negative impact on subjective assessments of quality of life.
The World Health Organization defined quality of life as “individuals’ perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns” (The WHOQOL Group, 1995, p. 1403). Thus, the term quality of life is a subjective assessment that goes beyond life satisfaction or well-being to include a person’s perceived health status, psychosocial status, and other aspects of life (The WHOQOL Group, 1995, 1998; World Health Organization [WHO], 1996, 1998).
The pandemic crisis due to COVID-19 was experienced as a mildly stressful event, with individuals more aware of their mental health status and quality of life (Zhang & Ma, 2020). Identifying coping strategies during stressful events like the COVID-19 pandemic is paramount to determining clinical and practical guidelines for promoting mental health and quality of life in survivors (Matthieu & Ivanoff, 2006). To our knowledge, few studies have considered the link between sociodemographic characteristics, adopted coping strategies, and their impact on quality of life (Pieh et al., 2020; Shamblaw et al., 2021). Nonetheless, past studies suggest an association between coping, relationship quality, depression, anxiety, and quality of life, and suggest there are several positive coping strategies for improving overall well-being during the pandemic (e.g., positive reframing).
Objectives
This paper presents an exploratory study of the coping strategies used by individuals with different sociodemographic characteristics during the COVID-19 pandemic mitigation phase in Portugal. The aim is to analyse how coping strategies differ according to sociodemographic variables and to investigate the relationship between coping strategies and quality of life. To this end, we hypothesise that there will be differences in coping strategies according to gender, age, marital status, level of education, the presence of children, and the degree of exposure to the virus during work. We also hypothesise that coping strategies will predict quality of life in all its domains (physical, psychological, social, and environmental).
Method
Participants
The sample for this study was a convenience sample. In total, 505 Portuguese residents, between 18 and 79 years old (mean age=42; SD=14.05) voluntarily completed the study protocol, which was made available online. Participants were ensured confidentiality and anonymity of all data. About 79% of the sample were women, 48% had a bachelor’s degree, and 51% were married or in a civil partnership. Of the 41% of participants who had children, 52% had children older than 12 years. Table 1 presents the sociodemographic characteristics of the sample. Only 14% of the participants acknowledged being at risk during work, and from that particular sample, about 48% worked in health services. Most participants were residents in Porto (25%), Lisbon (20%), Coimbra (17%), Braga (6%), and Setúbal (5%), with the remaining 27% from 15 other districts.

Measures
The research assessment protocol included three self-report questionnaires for assessing sociodemographic characteristics, coping strategies employed by participants during the pandemic, and quality of life.
The sociodemographic questionnaire enquired about individual characteristics (i.e., gender, age, education, work, family structure, etc.) and occupational circumstances during the COVID-19 pandemic. Occupational circumstances concerned the work situation before and during confinement (unemployed, employed, self-employed, student, retired, domestic, lay-off, medical discharge).
The short version of the Portuguese World Health Organization Quality of Life scale (WHOQOL-BREF; Vaz-Serra et al., 2006) is an adaptation of the World Health Organization Quality of Life Instrument. It comprises 26 items, answered according to a 5-point Likert scale, that assess one general factor on Health and Quality of Life along with 4 sub-domains: physical, psychological, social relations, and environment. The Portuguese version has been found to have good psychometric properties, with Cronbach alpha values ranging from .64 to .87 for the domains, and .92 for the overall scale (Vaz-Serra et al., 2006). In the current study, participants were instructed to answer according to their experience during the outbreak of COVID-19. The Cronbach alpha values across domains for the current sample were .75 for the physical domain, .79 for the psychological domain, .72 for the social relations domain, and .75 for the environment domain.
The Portuguese version of the Brief-COPE (Pais-Ribeiro & Rodrigues, 2004) is a self-report measure of 28 items that are answered on a 4-point Likert scale. These items assess 14 different coping strategies: active coping, planning, instrumental support, socioemotional support, venting, religion, positive reframing, self-blame, acceptance, denial, self-distraction, behavioural disengagement, use of substances, and humour. A high score in a given dimension means that the respondent uses that coping strategy often. This applies to both adaptive (i.e., active coping, planning, instrumental support, etc.) and non-adaptive (i.e., self-blame, denial, use of substances) coping strategies. The Portuguese version has shown to have good psychometric properties, with Cronbach alpha values ranging from .55 to .84, which is deemed appropriate considering that each scale only contains 2 items each (Pais-Ribeiro & Rodrigues, 2004). In the current study, participants were instructed to answer according to their experience during the outbreak of COVID-19. The Cronbach alpha values across subscales for the current sample were .81 for active coping, .79 for planning, .84 for instrumental support, .88 for socioemotional support, .91 for venting, .82 for religion, .75 for positive reframing, .76 for self-blame, .88 for acceptance, .82 for denial, .77 for self-distraction, .84 for behavioral disengagement, .89 for use of substances, and .77 for humor.
Procedure
The study protocol was submitted to the Ethical Committee of the (blinded for review purpose) University, and to the Portuguese Psychology Board, within the scope of research support during the COVID-19 pandemic. The inclusion criteria for study participation were being an adult (aged 18+) and living in Portugal. All relevant information for the participants’ informed consent was presented before the beginning of the questionnaire (informed consent form), and participants only completed the self-report measures after consenting to participate. The email address of the principal investigator was available if participants wanted to clarify any issues before, during, and/or after their participation. No information that would allow participants to be identified was requested. Participants were required to fill the self-report, online questionnaire anonymously, and this took about 10-15 minutes to complete. Data collection occurred between the 7th and the 23rd of May, 2020, a period when the Portuguese population was still mostly confined due to the pandemic, but progressively starting to return to some activities. The study was advertised through personal and institutional mailing lists, through the Portuguese Psychology Board mailing list, and social media channels (LinkedIn, Facebook, Instagram, Blogs). Volunteers did not receive any compensation for their participation.
Data analysis
Data were analysed with IBM SPSS version 26.0. First, six MANOVAs were conducted, each considering a different sociodemographic characteristic as the independent variable. These variables were: gender (male vs. female), age group (18-24, 25-34, 35-44, 45-54, 55-64, and 65+), marital status (single, married/in a civil partnership, and divorced/separated), education level (basic education, secondary education, bachelor, master, and. doctorate), responsibility for dependents (having dependents vs. not having dependents), and risk of infection at work (risk vs. no risk). For all six MANOVAs, the dependent variables were the different coping styles assessed by the Brief-COPE (active coping, planning, instrumental support, socioemotional support, religion, positive reframing, self-blame, acceptance, denial, self-distraction, behavioural disengagement, use of substances, and humour).
An absence of multivariate outliers was confirmed through the assessment of Mahalanobis Distances among participants. 10 scores above the critical chi-square value for each analysis (χ 2 =36.12, df=14, p=.001) were removed. An analysis of a scatterplot matrix between the dependent variables confirmed that linearity was met for each group of the MANOVA. Multicollinearity was checked through correlations among the dependent variables. The highest correlation between dependent variables was between active coping and planning at .69, confirming the absence of multicollinearity (Field, 2018).
We checked the equality of covariance matrices using Box’s M significance levels. In most tests, significance was above .05, indicating homogeneity of covariance. Where significance was below .05 (exposure to the risk of infection at work), group sizes included more than 30 participants each, making MANOVA robust against violations of this assumption (Allen & Bennett, 2008).
Next, three regression models were performed to test the predictive role of coping strategies on quality of life dimensions. For each model, different coping strategies were included as predictors and WHOQOL-BREF dimensions were considered outcome variables. A stepwise approach was chosen due to the exploratory nature of the study (Field, 2018).
All assumptions for these analyses were met. An analysis of standard residuals was performed to identify outliers, and this indicated that six participants needed to be excluded. After removal of these outliers, analyses of standard residuals confirmed that the data contained no outliers (Std. Residual Min=-3.29, Std. Residual Max=2.71). Tests to see if the data met the assumption of collinearity indicated that multicollinearity was not a concern in any of the models tested (Tolerance values from .98 to .77; VIF ranged from 1.02 to 1.31). The data also met the assumption of independent errors (Durbin-Watson values=1.52, 1.62, 1.65) except for the regression model where the environment dimension was the outcome variable (Durbin-Watson=.002). This resulted in the elimination of the regression model where environment was the outcome variable. The histograms of standardised residuals indicated that the data contained approximately normally distributed errors, confirmed with the normal P-P plots of standardised residuals, and the scatterplots of standardised residuals showed that the data met the assumptions of homogeneity of variance and linearity.
Results
Differences in coping strategies according to gender, age, marital status, education level, having children, and level of exposure to the virus during work
The first MANOVA revealed a statistically significant difference in coping strategies based on participants’ gender (male vs. female), F(14,440)=3.43, p<.0001; Wilk’s Λ=.90; η 2 =.10. There were significant gender differences in emotional support [F(1,453)=8.41; p=.004; η 2 =.02], religion [F(1,453)=5.71; p=.02; η 2 =.01], self-blaming [F(1,453)=4.83; p=.03; η 2 =.01)], venting [F(1,453)=6.93; p=.01; η 2 =.02], self-distraction [F(1,453)=5.51; p=.02; η 2 =.01], and behavioural disengagement [F(1,453)=7.01; p=.01; η 2 =.02]. Women had higher scores in emotional support, religion, venting, self-distraction, and behavioural disengagement, whereas men had higher scores in self-blaming.
The next MANOVA revealed statistically significant differences in coping strategies based on participants’ age group (18-24, 25-34, 35-44, 45-54, 55-64, 65+), [F(70,2060.82)=2.39, p<.0005; Wilk’s Λ=.69; η 2 =.07]. Age had a statistically significant effect on active coping [F(5,445)=6.13; p<.0005; η 2 =.06], planning [F(5,445)=4.50; p=.001; η 2 =.05], instrumental support [F(5,445)=3.20; p=.008; η 2 =.04), religion [F(5,445)=6.32; p<.0005; η 2 =.07], positive reframing [F(5,445)=4.33; p=.001; η 2 =.05], denial [F(5,445)=6.11; p<.0005; η 2 =.06], and self-distraction [F(5,445)=3.70; p=.003; η 2 =.04]. Younger participants (18-24 years old) showed lower scores in active coping than all other age groups, showed lower planning scores than participants between 35 and 64 years old, and showed lower instrumental support than participants aged 35-64. Likewise, participants aged 18-35 showed lower religion scores than middle aged adults (45-64), and lower positive reframing scores than participants aged 45-64. Older participants (55-64 and 65+ years old) showed higher denial scores compared to younger adults (18-44), and 65+ adults had higher self-distraction scores than those aged 35-34 and 45-54.
Statistical analyses revealed a significant difference in coping strategies based on marital status (single, married/in a civil partnership, divorced/separated) [F(42,1303.05)=2.02, p<.0005; Wilk’s Λ=.83; η 2 =.06]. Differences were significant for active coping [F(3,452)=3.39, p=.020; η 2 =.02], planning [F(3,452)=3.93, p=.01; η 2 =.03], instrumental support [F(3,452)=3.55, p=.02; η 2 =.02], emotional support [F(3,452)=3.24, p=.02; η 2 =.02], religion [F(3,452)=5.82, p=.001; η 2 =.04], positive reframing [F(3,452)=2.92, p=.03; η 2 =.02], and denial [F(3,452)=4.58, p=.004; η 2 =.03]. Those that reported being married or living in civil partnership had significantly higher scores in all the aforementioned coping strategies compared to single participants.
Statistically significant differences were found in coping strategies based on the education level of participants (basic education, secondary education, bachelor, master, and doctorate) [F(56,1694.23)=1.53, p=.01; Wilk’s Λ=.83; η 2 =.05] with differences found in denial [F(4,448)=4.46, p=.002; η 2 =.04], behavioural disengagement [F(4,448)=4.88, p=.001; η 2 =.04], and humour [F(4,448)=3.00, p=.02; η 2 =.03]. For denial and behavioural disengagement, those with a master’s degree displayed lower scores than those with basic and secondary education. Likewise, those at doctorate level showed higher humour scores than those with basic education.
The next MANOVA did not reveal a statistically significant difference in coping strategies based on participants’ responsibilities towards dependents (having dependents vs. not having dependents) [F(14,442)=1.35, p=.17; Wilk’s Λ=.96; η 2 =.04].
Finally, we identified statistically significant differences in coping strategies based on exposure to risk of infection at work (risk vs. no risk) [F(14,439)=1.91, p=.02; η 2 =.06], specifically in active coping [F(1,452)=4.47, p=.04; η 2 =.01], planning [F(1,452)=10.85, p=.001; η 2 =.02], instrumental support [F(1,452)=5.91, p=.02; η 2 =.01], and self-blaming [F(1,452)=7.43, p=.01; η 2 =.02]. Specifically, participants exposed to risk at work had higher scores in all strategies compared to those who were not exposed.
Coping strategies as predictors of quality of life
To assess the extent to which coping strategies predict variance in quality of life, we conducted several multiple linear regression analyses (stepwise method). Results are shown in Table 2. For the physical domain of quality of life, approximately 24% of the variance was explained by behavioural disengagement (β=-.20, p<.001), active coping (β=.25, p<.001), self-blaming (β=-.13 p=.002), denial (β=-.12, p=.008), substance use (β=-.02, p=.013), and positive reframing (β=.10, p=.038).
Table 2 Multiple linear regression models (Stepwise)
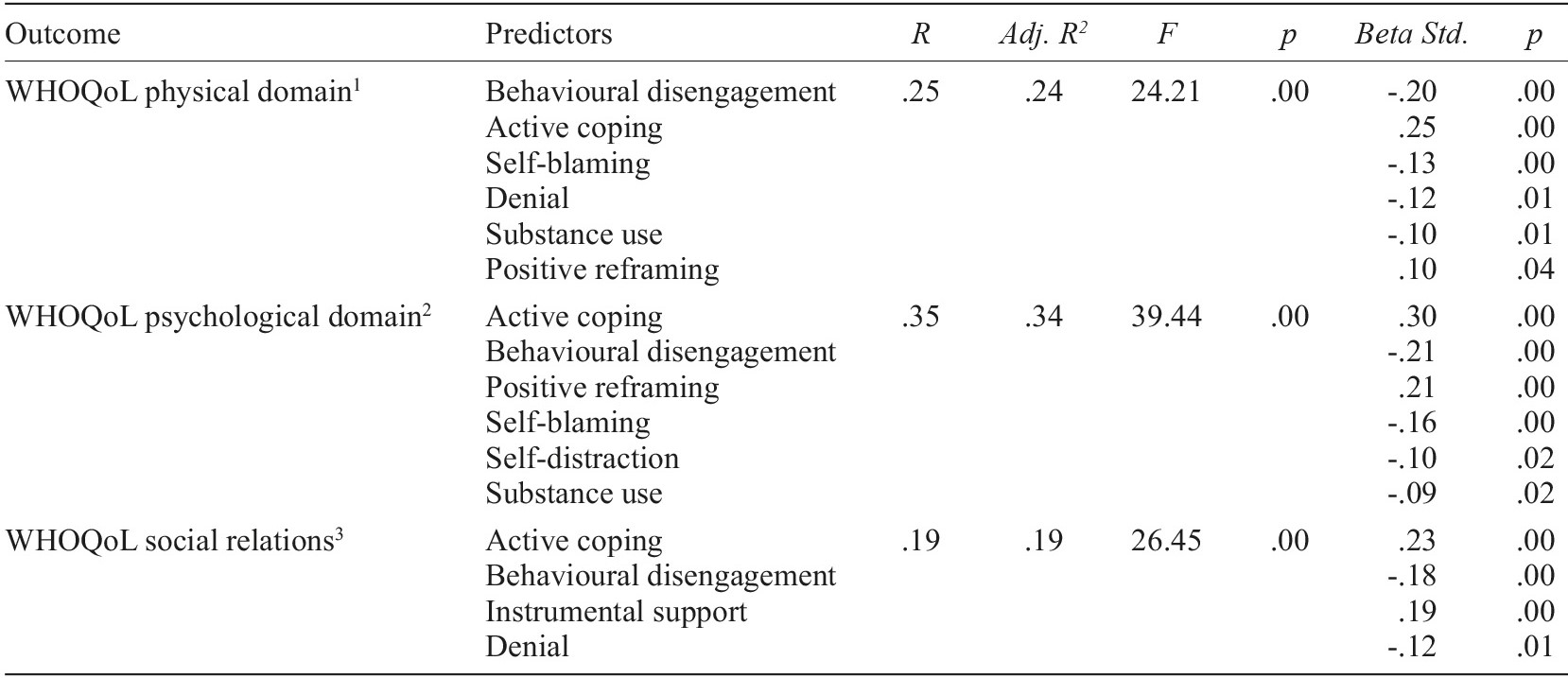
Note. 1Excluded variables (predictors): planning, instrumental support, emotional support, religion, acceptance, emotional expression, self-distraction, humour; 2Excluded variables (predictors): planning, instrumental support, emotional support, religion, acceptance, emotional expression, denial, humour; 3Excluded variables (predictors): planning, emotional support, religion, positive reframing, self-blaming, acceptance, emotional expression, self-distraction, substance use, humour.
For the psychological domain, about 34% of the variance was explained by active coping (β=.30, p<.001), behavioural disengagement (β=-.21, p<.001), positive reframing (β=.21, p<.001), self-blaming (β=-.16, p<.001), self-distraction (β=-.10, p=.015), and substance use (β=-.09, p=.019).
Finally, roughly 19% of the variance of the social relations domain was explained by active coping (β=.23, p<.001), behavioural disengagement (β=-.18, p<.001), instrumental support (β=.19, p<.001), and denial (β=-.12, p=.009).
Discussion
The present study aimed to investigate how coping strategies during the COVID-19 pandemic mitigation phase in Portugal differ according to sociodemographic characteristics. Although several socio-demographic differences were found, we found that they explained only a small quantity of variance in coping strategies (η 2 between .01 and 07).
Results showed that women used more emotional support, religion, venting, self-distraction, and behavioural disengagement coping strategies, while men used more self-blaming coping strategies during the mitigation phase of COVID-19 in Portugal. Other studies indicate that women tend to be more vulnerable and use more maladaptive coping strategies in crisis and disaster situations (Norris et al., 2002). The current study suggests that despite some maladaptive coping strategies (e.g., venting, self-distraction, and behavioural disengagement), women also use adaptive coping strategies such as seeking emotional support and engaging in religion, which are considered effective and positive strategies for coping with the pandemic situation (Carver, 1997; Carver et al., 1989; Meyer, 2001). Previous studies have found that women tend to seek more emotional support during stressful events compared to men (e.g., Ashton & Fuehrer, 1993). The findings also add empirical evidence that men are more likely to use self-blame coping strategies than women. This suggests a possible influence of cultural beliefs associated with men’s obligation to care for and protect the family as they provide the necessary resources to deal with critical situations (Matias et al., 2012). Self-blame has been considered an important dimension related to the development of psychopathology, especially depressive disorders (Zahna et al., 2015).
In this study, there were also differences in coping strategies according to age. Younger participants and older participants scored lower on several coping strategies for dealing with the COVID-19 pandemic mitigation phase than middle-aged participants. These results are surprising, as middle-aged adults tend to be at higher risk in a crisis (Norris et al., 2002). However, it is noteworthy that the sample collection occurred during the mitigation phase of the pandemic, and not during the lockdown phase, which was a more critical period. Younger individuals may have had difficulty coping with this crisis (Moreira et al., 2021; Wang et al., 2020) because they do not yet have as much life experience and do not play as many roles in their daily lives, which may have contributed to less effective strategies for coping with stressful events. Younger participants may struggle more with online college courses and working from home (Moreira et al., 2021), which can be extremely stressful. Social contact and support are also impaired, and some of the younger participants may be home alone or with older relatives, which may interfere with their ability to seek emotional support or to share their emotions and feelings. Older participants scored higher on avoidance strategies such as denial and self-distraction. These results may be related to the specific characteristics of the COVID-19 pandemic, in which older people are a particularly vulnerable population (Qiu et al., 2020; Rajukmar, 2020). Information about infection rates and mortality rates for those over 70 years old may have contributed to a greater denial of the situation and the use of distraction strategies to avoid dealing with the perceived risk of having severe manifestations of the disease in the event of infection (Agha, 2021). In addition, the novelty of the virus during this particular pandemic constantly implies new information about the evolution of the disease process. Older people may have more difficulty seeking and keeping abreast of new information, which may reinforce adopted denial and self-distraction coping strategies (Rajukmar, 2020).
There was also evidence of the benefits of being married or in a civil partnership when coping with COVID-19. This subgroup showed higher scores in using coping strategies to manage the crisis compared to single participants. This finding is consistent with previous findings that emphasize that younger individuals (18-25 years) are less likely to engage in active coping. It is expected that younger individuals were single compared to older individuals. It is possible that married individuals, as well as older individuals, were more likely to seek social support and actively address their difficulties than younger and single individuals. At the same time, participants who were married or in a civil partnership also used more denialist coping strategies, which is a maladaptive dimension (Carver, 1997; Carver et al., 1989; Meyer, 2001). Again, this finding is consistent with findings that older individuals (55+ years) are more likely to use denialist coping strategies. Likely, these older individuals were also married. Avoidant coping strategies, such as denial, allow individuals to handle and avoid the crisis and unwanted thoughts and emotions, easily. However, denialist coping strategies have been associated with mental health problems (e.g., depression, anxiety, and stress) during the COVID-19 pandemic (Agha, 2021). Therefore, we hypothesise that denial is used as a coping strategy to avoid the need to change and to maintain daily routines, and prevent experiencing unwanted and uncomfortable emotions and thoughts.
Statistically significant differences in coping strategies were found as a function of participant education level. These findings corroborate Norris et al.’s (2002) study in which this variable was related to the use of positive coping strategies. In the present study, participants with higher levels of education tended to cope with the crisis COVID-19 using less avoidant coping strategies (denial and behavioural shutdown) and more humour. Higher levels of education may be associated with a variety of opportunities and experiences and may help individuals develop an adaptive and positive repertoire of coping strategies (Vitulić & Prosen, 2016). Several factors have been identified as protective factors during the quarantine period, including gardening, regular physical activity, having access to healthy food, involvement in psychological and psychiatric interventions remotely (Moreira et al., 2021), and limited access to inadequate information (Brooks et al., 2020). Well-educated individuals may have the opportunity to be exposed to demanding and challenging events during their educational and career path, or to have easy access to healthy food and a healthy lifestyle, or even to maintain their mental health through intervention (Brooks et al., 2020; Moreira et al., 2021; Paulino et al., 2020). All of these factors may help participants respond in a constructive and resilient manner to this particular stressful and traumatic event.
No statistically significant differences were found in coping strategies based on participants’ responsibilities to their relatives. This is consistent with a recent study in Portugal that also found no differences in mental health outcomes due to the number of roommates, including family or relatives (Pereira et al., 2020). Although a recent study in the context of COVID-19 found that having relatives to care for was associated with better perceptions of quality of life (Morgado et al., 2021), in the current study participants’ coping strategies were not influenced by the presence of relatives.
Results also indicated that people exposed to workplace risk used more coping strategies (active coping, planning, instrumental support) compared to those who were not exposed, as in the study by Cai et al. (2020). The COVID-19 context may allow these workers to develop or use more proactive coping strategies than those who were forced to stay home. Nonetheless, those who were exposed to risk at work also had higher self-blame scores, which can be interpreted because they took an active role in the pandemic and were at greater risk of becoming infected and infecting others (i.e., family, colleagues, neighbours; Moreira et al., 2021).
Another major finding of the study was that coping strategies significantly predicted quality of life, with considerable explained variance across physical, psychological, and social domains. As expected, approaching coping strategies were positively associated with quality of life while avoidant coping strategies were negatively associated with quality of life (Shamblaw et al., 2021). In particular, active coping and positive reframing were positive predictors of physical and psychological quality of life. For avoidant coping strategies, behavioural disengagement was a strong negative predictor of quality of life in all domains, with many other strategies of the same type making negative contributions to individuals’ quality of life (self-distraction, denial, substance use, and self-blame). We found that humour, religion, planning, socioemotional support, venting, and acceptance were not significant predictors of quality of life.
These results highlight the role that different coping strategies may have on different domains of quality of life in a situation such as the COVID-19 mitigation phase. In particular, instrumental support was only significantly associated with the domain of social relationships, highlighting the relevance of practical information, help, and advice (Brooks et al., 2020) for social quality of life (but not for the physical and psychological dimensions). In the context of the COVID-19 mitigation phase, positive reframing was significantly associated with psychological quality of life, but this was not the case for either planning or emotional support. This finding suggests the relevance of strategies based on reframing the current situation rather than making plans for an unpredictable situation or even receiving compassion or emotional support from others.
Overall, these findings suggest that proximal and pragmatic coping strategies that focus on taking action and overcoming COVID-19 challenges may prove particularly useful for physical, psychological, and social quality of life amid the pandemic. In particular, positive reframing is an important strategy for psychological quality of life, while instrumental support contributes to quality in social relationships. According to Folkman’s (2012) assumption, in situations where individuals do not have control over the problem, emotion-focused coping strategies may be more effective than problem-solution-focused strategies. Although our results support the effectiveness of problem-solution focused strategies during a period of uncertainty and lack of control, we must also consider that the current sample was recruited during a return to normalcy and after a period of total community lockdown in which uncertainty was higher.
The present study has some limitations and the results should be generalized with caution. For example, the current study had a cross-sectional design, meaning no evidence of temporal relationships or causality can be inferred. In addition, this study was conducted using an online survey sample. Only individuals who had internet access and were comfortable with web surveys were able to participate. Further, outcome variables were assessed using self-report questionnaires, so only self-perceived experiences were available. The sample consisted mainly of women and of participants with higher levels of education, which suggests it may not be fully representative of the general population in Portugal. Individuals with easy access to the Internet, familiarity with Web surveys, and higher levels of education may exhibit a particular profile of coping strategies and self-regulatory processes directly related to emotion regulation that differ from population norms. Finally, the sociodemographic questionnaire did not include questions about working from home, current or past infection with SARS-COV-2, interaction with infected patients at intensive care units, or other psychosocial characteristics that might influence adopted coping strategies and quality of life. Nevertheless, the current study represents a first attempt to assess the coping strategies adopted by Portuguese residents during a stressful event such as the COVID-19 pandemic and to understand how this affects one’s perceived quality of life.
Conclusion
The current study evaluates how people cope with stressful events during a catastrophic event (COVID-19) and highlights the role of effective and active coping strategies in promoting perceived quality of life. The results also emphasize the negative role of behavioral disengagement strategies on perceived quality of life. We found that middle-aged individuals with higher levels of education and higher workplace risk exposure were most likely to use effective and adaptive coping strategies. Women were more likely to use adaptive and maladaptive coping strategies, except for self-blame, which was more prevalent in men. Overall, active coping was the strongest and most positive predictor of the physical, psychological, and social domains of quality of life, followed by behavioral disengagement as a negative predictor of quality of life. Individuals who focus on doing something about the current situation to improve their emotional, physical and social status appear to have better levels of quality of life. Mental health prevention and recovery plans related to the pandemic COVID-19 must update their goals, interventions, and strategies based on empirical and current research. Health systems and organizations involved in mental health recovery are encouraged to promote stress management programs and workshops that encourage individuals to use their resources to cope with stressful situations, focusing particularly on empowerment strategies. In addition, psychological first aid interventions target adaptive coping strategies, so the current findings may be useful for informing future interventions with individuals reporting emotional and related disorders associated with COVID-19 experiences. Personal and posttraumatic psychological growth needs to be explored and analyzed following the COVID-19 pandemic mitigation period. Further studies should seek to examine groups at risk of using less effective coping strategies to provide guidelines for mental health programs and psychological first aid services. Health professionals should pay particular attention to coping strategies such as self-blame and denial, and assess how younger and older adults cope with social isolation to enhance their ability to seek emotional and social support. Because the current study occurred during a time in which little was known about COVID-19, but also when the first lockdown in Portugal appeared to be ending, the current study highlights an important point: a proactive approach to current challenges promotes a positive perception of quality of life amid the pandemic COVID-19.

