











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
There is considerable evidence showing that studying at university can be a stressful experience for many individuals with stress being part of their daily life (Larcombe et al., 2016). The transition to university implies different psychological challenges over the years since individuals’ ideals, conflicts and distress will make individuals more vulnerable to personal difficulties (Castro, 2017). Additionally, this period of life is marked by the need of making important decisions for the future (Foret et al., 2012). Indeed, studies have shown that most university students experience stress or burnout (Larson, 2006; Misra & Castillo, 2004) which highlights the need for improving university students’ psychological well-being and performance. Especially the start and the end of the semester seem to be a risk period for increased stress (e.g., Pitt et al., 2018).
The prevalence of less severe mental disorders seems to be higher among students from the humanities and health sciences courses. It seems that the academic contents related to human subjectivity and the contact with individuals in suffering place these students in risk which can lead to higher levels of personal suffering and the development of some types of disorders (Andrade et al., 2016). The potential exposition to stress can lead to changes in emotions and cognitions causing anxiety and depression (Atkins & Hayes, 2019). For this reason, the development of intervention programs targeting stress and promoting relaxation seems to be important to promote the development and training of coping strategies more effective to deal with the university-related stress (Foret et al., 2012). In this sense, it urges to develop and implement programs that promote the personal, emotional and social development of the university students and not only their intellectual or professional performance (Castro, 2017; Chaló et al., 2016; Nunes & Garcia, 2010; Teixeira et al., 2007). This is especially important because learning processes are likely to be influenced by several external factors (Diniz, 2005; Ferreira et al., 2001).
Self-compassion as a way to happiness
Self-compassion can be defined as the individuals’ ability to “being touched by and open to one’s own suffering, not avoiding or disconnecting from it, generating the desire to alleviate one’s suffering and to heal oneself with kindness. Self-compassion also involves offering nonjudgmental understanding to one’s pain, inadequacies and failures, so that one’s experience is seen as part of the larger human experience” (Neff, 2003, p. 87). This concept emerges as an individual’s compromise to prevent or relieve suffer (Marques et al., 2018). According to Neff (2003), self-compassion entails three basic components: self-kindness, common humanity, and mindfulness. Self-kindness refers to the individuals’ ability to extend kindness and understanding to oneself, avoiding harsh judgment and self-criticism; common humanity refers to individuals’ ability to seeing one’s experiences as part of the human experience avoiding feelings of failure; finally, mindfulness refers to individuals’ ability to hold one’s painful thoughts and feelings in balanced awareness and avoid over-identification.
Paying attention to the present moment has been seen as a source of happiness since it tends to promote intra and interpersonal well-being (Marques et al., 2018). For instance, Neff et al. (2007) found that self-compassion is positively associated with happiness perception, optimism and positive affect, protecting individuals from anxiety and depressive symptoms. Also, Raes (2011) refers that self-compassion is an important protective factor against emotional problems since higher levels of self-compassion were associated with less depressive symptoms.
According to Ryff (1989), happiness results from the balance between several domains, namely self-acceptance, personal growth, purpose in life, positive relations with others, environmental mastery and autonomy. Fordyce (1983) beliefs that happiness is linked to a long-term general sensation of emotional well-being and life satisfaction and can be increased through the adoption of positive thinking and awareness of the present moment. This would contribute to avoid rumination and promote acceptance.
For all of these reasons, interventions targeting relaxation would be effective in reducing anxiety and stress by promoting positive emotions and the development of skills for dealing with physical and mental problems (Barnard & Curry, 2011; Marques et al., 2018). Moreover, self-compassion, meditation and harmonious breathing should be trained to promote positive health behaviors (Sirois et al., 2014).
Autogenic training
The autogenic training (AT) or “being yourself” (auto means self and genic means being) was originally developed by Johannes Schultz and was later refined with Wolfgang Luthe (Naylor & Marshall, 2007). It emerged as a result of the findings related to the therapeutic hypnosis and some authors suggest that the AT can induce a meditative state (Yurdakul et al., 2009). AT is seen as a way of intervention in the individuals’ development by focusing on primary prevention and skills, appearing as one of the main psychological treatment in group to improve individuals’ self-regulation skills (Krampen, 1996). Thus, it is recognized by the American Psychological Association as an effective mind-body therapy (Atkins & Hayes, 2019).
This technique promotes the process of self-knowledge with individuals adopting an active participation and responsibilization in their treatment (Carruthers, 1979; Houghton, 1996; Kanji & Ernst, 2000). This means that the AT beliefs in individuals’ internal resources for own self-healing and allows to be aware of individuals internal manifestations (Kanji, 2000).
The six-based exercises proposed by Schultz (1967) are still the core of the autogenic training and focuses attention on different parts of the body by using autosuggestion to repeat internal phrases that promote heaviness sensations, regulate cardiac activity, and control breathing. Relaxation is achieved using passive concentration that allows to contact mentally with the different parts of the body (Kanji, 2000; Kanji & Ernst, 2000).
This allows achieving three important aspects of relaxation: reduce muscle tension in the body, change the style or the way people think, and change the content of what they are thinking (Naylor & Marshall, 2007). Its regular practice allows adopting a new and well-succeed way of living and thinking (Kanji, 2000). Some benefits of the AT include achieve peace of mind, develop skills to deal with life challenges, emotional balance, improved health and well-being, development of coping skills and control of body responses to stress; in short-term, it helps to neutralize acute stress and fatigue, as well as to promote mental and physical rest (Kanji, 2000).
Guided imagery
Relaxation can benefit from include exercises focused on mental images that through imagery contribute to reduce body response to stress. Imagery is considered be therapeutic in many cultures, since it provides a deep journey through the inner life that will lead to self-knowledge - it is the mind thinking about our inner reality through images (Kestenberg et al., 2014). Hernández et al. (2014) consider the breathing, the Schulz’s autogenic training (relaxation through mental control) and imagery (through mental sensations) are effective techniques in reducing anxiety.
According to Lynn and Rhue (1988) as cited in Özü (2010), the main aim of the guided imagery is to calm individual’s mind, promote individual’s skills to face negative emotions, and to improve individual’s sense of consciousness by using five senses. This will allow to teach individuals to induce inner power and eliminate negative emotions. These techniques are usually used in the initial phase of guided imagery since they facilitate the mind to be open to experiences, consciousness, and facilitate individuals’ processing skills of positive images. As highlighted by Morrison and Cometa (1977) as cited in Özü (2010), guided imagery can support other therapeutic techniques that aim to work individuals’ skills in different domains.
Apóstolo and Kolcaba (2009) using a guided imagery intervention with psychiatric inpatients with depressive disorders found that it contributed to increase patients’ comfort and decrease patients’ depression, anxiety, and stress over time. This guided imagery intervention included progressive muscle relaxation, imagine relaxing natural scene, imagine meetings with significant figures, and create positive, comforting, and serene images of the hospital; all these stimuli would contribute to easiness, safety, positive images, and elimination of disturbing thoughts. Also, Tugade and Fredrickson (2007) suggest that guided mediation practices aiming at inducing positive experiences can contribute to prolong positive emotional experiences with benefits for physical and mental health.
Positive Psychology
Positive Psychology (PP) was defined by Seligman (1999) as a science that emphasizes the understanding and promotion of individuals’ positive qualities such as optimism, courage, ethics, meaning in life, interpersonal skills and social responsibility. It examines the conditions that allow the optimal functioning of individuals allowing to improving quality of life and preventing psychopathology. It aims to develop individuals’ skills and not to correct their weaknesses (Seligman & Csikszentmihalyi, 2000).
This positive approach understands better the psychopathology, since it removes the focus from the symptoms treatment and directs their attention to the promotion of well-being (Marques et al., 2018). It aims to make life happier and more significant (Seligman, 2004). Thus, interventions based on this approach aim to promote positive psychological states such as gratitude, optimism, and mindfulness through systematic exercises (Nikrahan et al., 2016). These exercises represent a complementary strategy to promote mental health being used as a self-help strategy (Bolier et al., 2013). Relaxation is recognized as a way to promote positive emotions and experiences of calmness allowing the development of resources to improve health and achieve well-being (Estrela-Dias & Pais-Ribeiro, 2014).
Music and its therapeutic purpose
Music is part of the relaxation interventions that aim to reduce stress, anxiety, depression and psychological tension (Klainin-Yobas et al., 2015; Lufiego et al., 2017). This is because the human body has an innate predisposition to answer internally to sounds and rhythms from the external environment (Nunes-Silva et al., 2016). Since the beginnings of humanity music is used for healing purposes but musicotherapy only emerged in the 20th century, as a science that aims to understand the interaction between human being, music and their sound elements, as a way to promote quality of life (Nunes-Silva et al., 2012).
Studies have shown that music is likely to reduce anxiety (Karagozoglu et al., 2013) and stress, leading to happiness, tranquility and well-being. Thus, some types of music seem to keep mental health, having an important role in the emotional development of individuals (Nunes-Silva et al., 2012). It facilitates the release of endorphins and cortisol reduction, promoting well-being and inducing relaxation (Chanda, & Levitin, 2013; Khalfa et al., 2003; Koelsch et al., 2011). Thus, music is seen as a powerful tool to evoke emotions, especially positive ones.
Present study
The first aim of this study was to evaluate the efficacy of a relaxation protocol (that included autogenic training and guided imagery) in reducing depression, anxiety and stress among university students. It was hypothesized that participants of the experimental group would experience a reduction in depression, anxiety, and stress over time, in comparison to the active and passive control group.
The second aim was to examine the associations between self-compassion, subjective happiness, depression, anxiety, and stress and the importance attributed to mental health in the total sample at baseline. Additionally, we explored the moderation role of self-compassion. While the links between happiness and depression, anxiety, and stress is already described in the literature (e.g., Mason, 2015; Silva & Figueiredo-Braga, 2018) as well as the link between self-compassion and depression, anxiety, and stress (e.g., Muris et al., 2016; Van Dam et al., 2011), there is a gap in the literature regarding the potential moderator role of self-compassion in the link between subjective happiness and depression, anxiety, and stress. Because some studies have suggested that psychological suffering and well-being seems to vary according to levels of self-compassion (Ghali, 2015; Homan, 2016), we tested this hypothesis. We expected that the link between happiness and depression, anxiety, and stress would be stronger for those with lower levels of self-compassion.
Method
Design
This randomized controlled trial followed CONSORT guidelines (2010). A parallel-group design with an equal randomization made by an independent observer by hand by ordering participants’ name and allocating them sequentially was conducted (allocation ratio of 1:1 patient for three groups: group 1 - intervention group, group 2 - active control group, and group 3 - passive control group). The allocation was performed twice because we recruited participants in two phases (one between 2019 May and July and the other between 2019 October and December). This was a no-blinded study (both participants and interventionists were not blinded to group assignment). The sample size was calculated based on the formula: n=[(Zα/2+Zβ)2×{2(ó)2}]/(μ1-μ2)2 (Sakpal, 2010). The stress subscale of DASS-21 was used considering the means and standard deviations of a similar intervention with the same population (Parcover et al., 2018). A sample size of 123 participants, 41 in each arm, was sufficient to detect a clinically important difference of 4,3 points assuming a standard deviation of 7 using a two-tailed t-test of difference between means with 80% power and a 5% level of significance.
Participants were assessed in three moments: baseline, at the end of the intervention (6 weeks later), and at the follow-up (4 weeks later).
Participants
One hundred and sixty-one students met the eligibility criteria and agreed to participate. Participants’ age ranged from 17 to 46 years (M=20.96 years, SD=3.66). Participants were assigned to the experimental group (n=55), the active control group (n=51), or the passive control group (n=55). Participation followed the Declaration of Helsinki.
Participants were recruited during classes between May 2018 and December 2019. Inclusion criteria were: being a university student; agreeing to participate and complete the three assessment moments.
Interventions
Experimental group. Participants in the experimental group participated in 6 weeklies, 20 min. sessions of a relaxation protocol based on the PP approach (music was not included in this protocol). This number of sessions was chosen based on previous studies (e.g., Atkins & Hayes, 2019).
The relaxation protocol focuses on two essential aspects namely guided imagery and diaphragmatic breathing. Goals were to promote the experience of more positive emotions and reduce the prevalence of depression, anxiety, and stress. The relaxation protocol emerges as a facilitator for the management of thoughts and negative emotions while positive psychology emerges as a facilitator of positive emotions and, consequently, psychological wellbeing.
The intervention consisted of three phases: phase 1 - Beginning of Relaxation, phase 2 - Body Awareness, and phase 3 - Guided imagery.
In phase 1 - Beginning of Relaxation, participants were asked to sit comfortably in the chair with their palms facing down. Then, were invited to close their eyes gently to decrease attention to external stimuli. Here participants were asked to focus on diaphragmatic breathing (i.e., a breathing that accentuates movement in the lower part of the belly, requires less effort and is predominant in states of rest, relaxation and during sleep; Elias, 2009) and guided imagery, as essentials issues for leading to relaxation. Examples of specific instructions given to participants during the sessions: “Inhale deeply through your nose, filling your abdomen and feeling the weight of the air. Visualize air coming through your nostrils and being transported to your lungs, promoting relaxation, well-being, health, energy and vitality to every cell in your system”.
In phase 2 - Body Awareness - six established exercises or techniques proposed by Schultz (1967) were applied: (1) induce heaviness by using verbal cues that suggest heaviness in the body; (2) induce warmth by using verbal cues that call attention to warmth; (3) reduce heartbeat by using verbal clues that call attention to the heartbeat; (4) breathing practice by using verbal cues focus on breath; (5) abdominal practice by using verbal cues focus on abdominal sensations; and (6) head practice by using verbal cues on the coolness of the forehead. Examples of specific instructions given to participants during the sessions: “Repeat 5 times inwardly to yourself: “My arms are pleasantly heavy and relaxed”, “My heart beats peacefully”, “My breathing is calm and balanced”, “I am completely calm and relaxed”.
In phase 3 - Guided Imagery - the objective was to promote the development of personal resources that could be used as coping strategies to improve health and individuals’ well-being, by focusing on positive emotions. Examples of specific instructions given to participants during the sessions: “Now that you feel totally calm, relaxed and safe as you breathe in, imagine the air entering your system. By bringing more oxygen, energy, and vitality to each of your cells, your organs, and systems, you also bring love, peace, well-being, joy, harmony, strength, health, and healing. As you exhale, imagine that you expel everything that imprisons you, tires you and wears you out, what you no longer want to keep in your life. Feel untied, freer, happier.”
Finally, a last phase was included to leave the relaxation state. Participants were guided to experience feelings of gratitude toward themselves for engaging in self-care; then, they were asked to return from the relaxation state, awakening gently the five senses.
To ensure intervention fidelity, an explicit treatment protocol (with the autogenic training and instruction to diaphragmatic breathing and guided imagery) was developed, and the intervention was carefully supervised by senior researchers, one of them with training in the therapeutic model.
Active control group. Participants assigned to the active control group participated in 6 weekly, 20 min. sessions of relaxing music. In the beginning of each session participants were asked to close their eyes and to do abdominal breathing so participants could make the most of that time. The music was chosen based on some characteristics that are essential to boost a relaxation state, namely: slow tempo and slow-moving melody, harmonious combination of instruments and sounds of nature (Khalfa et al., 2003; Nunes-Silva et al., 2012, 2016).
Passive control group. Participants assigned to the passive control group did not participate in any intervention, but they had the opportunity to receive the relaxation protocol training after completion of the study (i.e., in the beginning of the following school semester).
Measures
Sociodemographic questionnaire. Data on sex, age, scientific area of study and curricular year were collected. Participants were asked about the importance given to mental health in a seven points Likert-type scale. Participants from the intervention group, the active control group and the passive control group filled out a questionnaire at three times: baseline, 6 weeks post-intervention and 4 weeks follow-up.
Depression, anxiety and stress. The Depression, Anxiety, and Stress Scale (DASS-21; Lovibond & Lovibond, 1995; Portuguese version: Pais-Ribeiro et al., 2004) was used to measure depression, anxiety, and stress. The DASS-21 is composed by 21 items divided into three subscales: depression (7 items), anxiety (7 items), and stress (7 items). Items are rated on a Likert-type scale from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). Depression, anxiety, and stress scores are calculated using the sum of the items, with higher scores indicating higher depression, anxiety, and stress symptoms. Cronbach’s α in our study was .84 for depression, .81 for anxiety, and .88 for stress.
Self-compassion. The Self-Compassion Scale (SCS; Neff, 2003; Portuguese version: Castilho & Gouveia, 2011) was used to measure self-compassion and its three basic components: self-kindness, common humanity, and mindfulness. The SCS is composed by 26 items and comprises six subscales: self-kindness (5 items; item example: “I try to be loving towards myself when I’m feeling emotional pain”), self-judgment (5 items; item example: “When times are really difficult, I tend to be tough on myself” - reversed), common humanity (4 items; item example: “When things are going badly for me, I see the difficulties as part of life that everyone goes through”), isolation (4 items; item example: “When I’m feeling down, I tend to feel like most other people are probably happier than I am” - reversed), mindfulness (4 items; item example “When something upsets me I try to keep my emotions in balance”), and over-identification (4 items; item example “When I’m feeling down I tend to obsess and fixate on everything that’s wrong” - reversed). Items are rated on a Likert-type scale from 1 (almost never) to 5 (almost always). Subscale scores result from the mean of subscale items. Cronbach’s α in our study was .93.
Subjective happiness. The Subjective Happiness Scale (SHS; Lyubomirsky & Lepper, 1999; Portuguese version: Pais-Ribeiro, 2012) was used to measure subjective happiness. It is composed by four items, two ask participants to characterize themselves using rating relatives to peers, and two offer participants descriptions of happy and unhappy individuals asking them to rate the extent to which each item describes them. Cronbach’s α in our study was .79.
Data analysis
Data were analyzed using SPSS version 26. Means and standard deviations were used to characterize the sample as well as to examine the study variables for the total sample and for each group (intervention, active control group and passive control group). α was set at 0.05 (two-tailed).
To examine the efficacy of the intervention group and compare differences among groups over time (first aim), Multilevel Modeling (MLM) was used. MLM is a useful method to examine data with repeated measurements and organized in nested levels. Two-level multilevel models were used to examine the effect of the relaxation protocol on depression, anxiety, and stress: measurement occasions (level 1) nested within individuals (level 2).
To examine the relationship between study variables (second aim), Pearson correlations and regression analyses were used. To examine the moderating role of self-compassion in the association between subjective happiness and depression, anxiety, and stress, the PROCESS macro (Model 1 - simple moderation) (Hayes, 2018) was used. In this model, we included subjective happiness as independent variable, depression, anxiety, and stress as dependent variables, and self-compassion as moderator.
Results
Recruitment
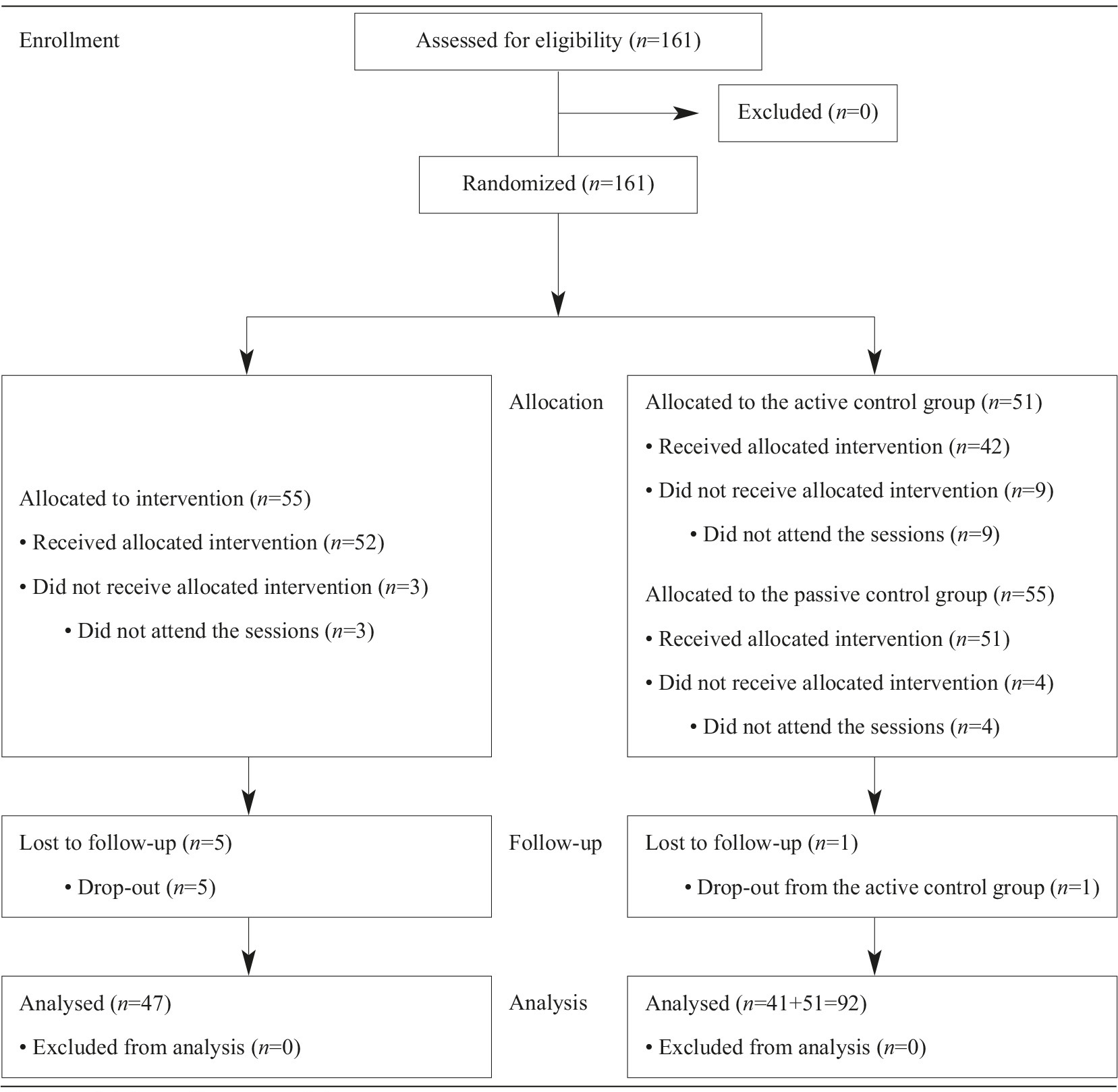
Participants were assessed for eligibility during May 2018 and December 2019. A total of 161 participants consented to participate and were randomized with 55 participants being allocated to the intervention group, 51 to the active control group and 55 to the passive control group. During the study, eight participants from the intervention group, ten from the active control group and four from the passive control group withdrew from the study (e.g., lack of time and difficulty in combining the AT with school activities). The final number of participants included in the analysis was 139; 47 in the experimental group, 41 in the active control group and 51 in the passive control group (see Figure 1). The overall inclusion rate was 85% for the intervention group; 80% for the active control group and 93% for the passive control group. Figure 1 shows the flow diagram that is available for reporting an RCT (Moher et al., 2012).
Descriptive results
Baseline demographic characteristics for each group are presented in Table 1. Most of the participants were women (90.6%), with a mean age of 20.96 (SD=3.65; range 17-46). In terms of curricular year, 12.9% (n=18) were in the 1st year, 8.6% (n=12) were in the 2nd year, 63.3% (n=88) were in the 3rd year, 14.4% (n=20) were in the 4th year, and 0.7% (n=1) were in the 5th year. Most of the participants were attending a degree in human and social sciences (80.6%; n=112), while the remaining were attending a degree in life and environment sciences (19.4%; n=27). Means and standard deviations for each dependent variable follows:
Table 1 Sample characteristics
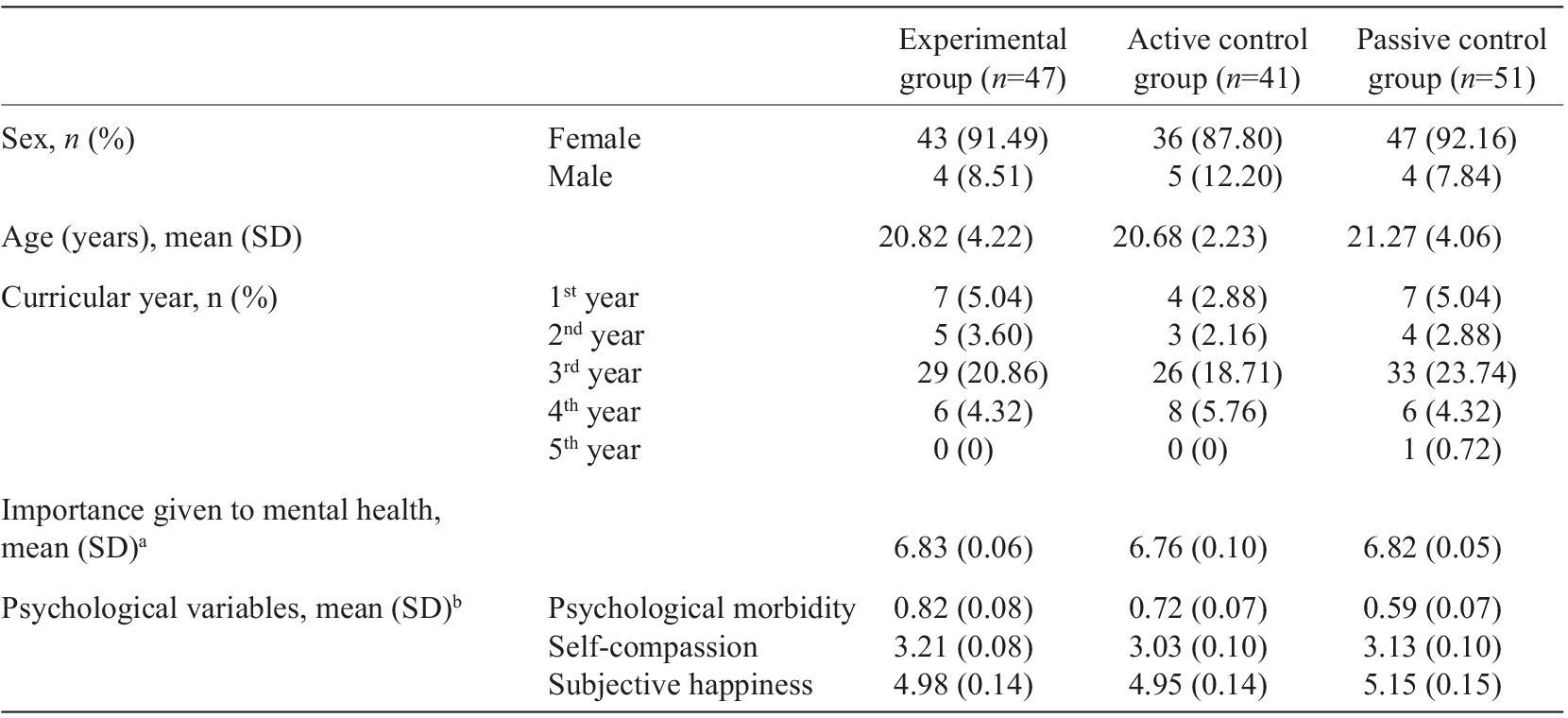
Note. aA higher score indicates more importance attributed to mental health (range 1-7); bHigher scores indicate higher levels of depression, anxiety, and stress (range 0-3), higher levels of self-compassion (range 1-5) and higher levels of perceived happiness (range 1-7).
Depression. Paired-sample t tests indicated significant differences between depression at baseline and depression after intervention [t(138)=3.12, p<.01] and between depression at baseline and depression at follow-up [t(138)=2.33, p<.05]. Participants presented higher depression at baseline (M=.55; SD=.51) in comparison to after intervention (M=.43; SD=.47) and to follow-up (M=.46; SD=.46).
Anxiety. Paired-sample t tests indicated no significant differences between anxiety at baseline and anxiety after intervention [t(138)=1.46, p=.146] neither between anxiety at baseline and anxiety at follow-up [t(138)=1.53, p=.127].
Stress. Paired-sample t tests indicated significant differences between stress at baseline and stress after intervention [t(138)=2.19, p<.05] and between stress at baseline and stress at follow-up [t(138)=2.15, p<.05]. Participants presented higher stress at baseline (M=1.05; SD=.67) in comparison to after intervention (M=.93; SD=.64) and to follow-up (M=.93; SD=.63).
Levels of self-compassion (M=3.12; SD=.63) and levels of subjective happiness (M=5.03; SD=.98) were below the mean - considering the mean of the Likert scale. The importance given to mental health was high (M=6.81; SD=.46).
Aim 1 - Intervention main effects
Depression
Base model. In the first step a base model was estimated with no predictors. In this model, depression was estimated by its mean (M=.48), a specific term representing within-subjects variability (=.13) and an error term associated with each observation (=.10). Intra-class coefficient was .551 which justifies the exploration of predictors of change in individuals’ depression.
Unconditional model. This model adds the time as predictor of changes in individuals’ depression. Results revealed a significant change in depression over time (-.05, p<.05) (see Table 2). Depression reduced 0.05 units and their global mean increased 0.57. The analyses over time reduced the estimate of the error variance of 9.7% (from .103 to .093) showing that the time explained some of the observed variance in the depression. As this variance is statistically different from 0 (p<.001), other predictors should be examined.
Table 2 Results from MLM analyses regarding Psychological Morbidity
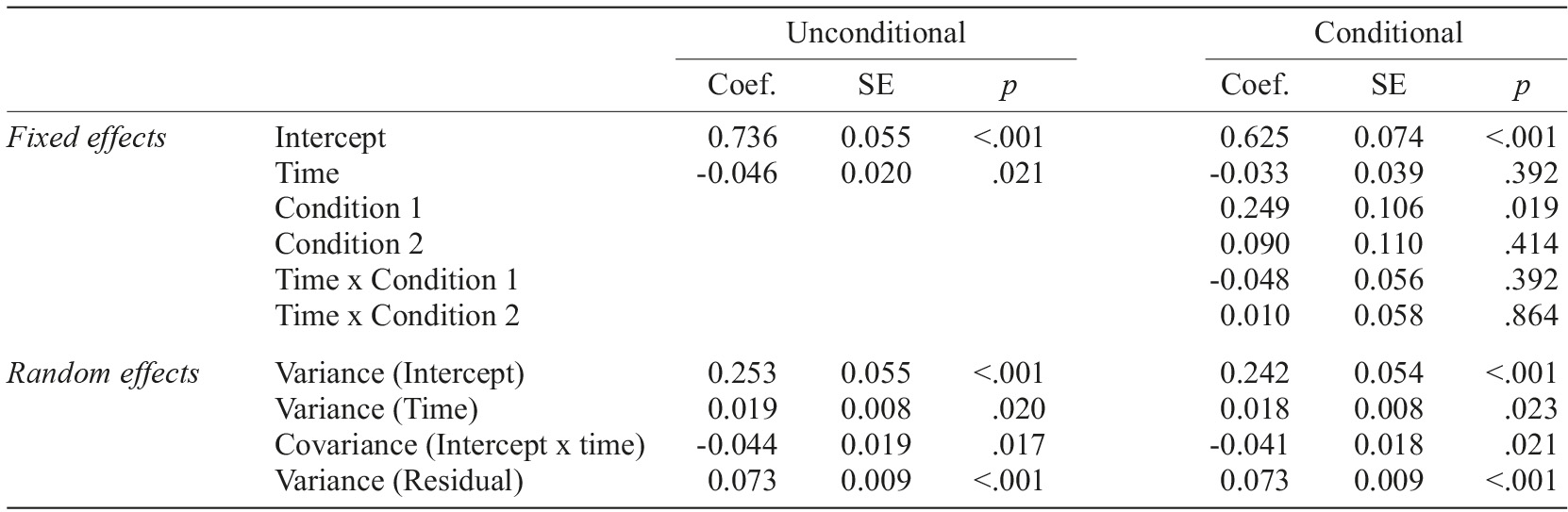
Note. Condition 1 - intervention group; Condition 2 - active control group; Passive control group was used as reference.
Conditional model. This model adds the condition (i.e., intervention group, active control group or passive control group) as predictor of change in individuals’ depression. When the condition was added as predictor, the time was no longer a significant predictor of changes in individuals (=-.04; p=.25) and the global mean of depression reduced to .53. None of the conditions showed a significant interaction with time (p=.58 e p=.98). It is important to note that the variance error did not change (.093).
Anxiety
Base model. In the first step a base model was estimated with no predictors. In this model, anxiety was estimated by its mean (M=.48), a specific term representing within-subjects variability (=.15) and an error term associated with each observation (=.10). Intra-class coefficient was .594 which justifies the exploration of predictors of change in individuals’ anxiety.
Unconditional model. This model adds the time as predictor of changes in individuals’ anxiety. Results revealed a non-significant change in anxiety over time (-.03, p>.05) (see Table 2). The analyses over time reduced the estimate of the error variance of 32% (from .103 to .070) showing that the time explained some of the observed variance in the anxiety. As this variance is statistically different from 0 (p<.001), other predictors should be examined.
Conditional model. This model adds the condition (i.e., intervention group, active control group or passive control group) as predictor of change in individuals’ anxiety. When the condition was added as predictor, the global mean of anxiety reduced to .45. None of the conditions showed a significant interaction with time (p=.50 e p=.28) and only one significant interaction between the intervention group and the passive control group was found (=.27; p=.05) (see Table 2). This means that anxiety increased 0.27 units in the intervention group when compared to the passive control group. It is important to note that the variance error did not change (.070).
Stress
Base model. In the first step a base model was estimated with no predictors. In this model, stress was estimated by its mean (M=.97), a specific term representing within-subjects variability (=.14) and an error term associated with each observation (=.14). Intra-class coefficient was .649 which justifies the exploration of predictors of change in individuals’ stress.
Unconditional model. This model adds the time as predictor of changes in individuals’ stress. Results revealed a significant change in depression over time (-.06, p<.05) (see Table 2). Stress reduced 0.06 units and their global mean increased 1.09. The analyses over time reduced the estimate of the error variance of 50% (from .144 to .072) showing that the time explained some of the observed variance in the stress. As this variance is statistically different from 0 (p<.001), other predictors should be examined.
Conditional model. This model adds the condition (i.e., intervention group, active control group or passive control group) as predictor of change in individuals’ stress. When the condition was added as predictor, the time was no longer a significant predictor of changes in individuals (=-.02; p=.62) and the global mean of stress reduced to .87. None of the conditions showed a significant interaction with time (p=.21 e p=.66) and only one significant interaction between the intervention group and the passive control group was found (=.41; p=.01) (see Table 2). This means that stress increased 0.41 units in the intervention group when compared to the passive control group. It is important to note that the variance error did not change (.072).
Aim 2 - Associations among study variables
A positive significant association was found between self-compassion and subjective happiness (r=.46, p<.01). Negative significant associations were found between self-compassion and depression (r=-.47, p<.01), anxiety (r=-.33, p<.01), and stress (r=-.48, p<.01) and between subjective happiness and depression (r=-.48, p<.01), anxiety (r=-.41, p<.01), and stress (r=-.44, p<.01). The importance given to mental health was negatively associated with self-compassion (r=-.22, p<.01) and positively associated with subjective happiness (r=.23, p<.01). No association was found with depression, anxiety, and stress.
In terms of predictors, self-compassion (ß=-.32, p<.01) and subjective happiness (ß=-.34, p<.001) were both significant predictors of depression [F(2,136)=30.70, p<.001], explaining 30% of its variance. Self-compassion (ß=-.18, p<.05) and subjective happiness (ß=-.33, p<.001) were both significant predictors of anxiety [F(2,136)=16.23, p<.001], explaining 19% of its variance. Finally, self-compassion (ß=-.36, p<.001) and subjective happiness (ß=-.28, p<.01) were both significant predictors of stress [F(2,136)=28.62, p<.001], explaining 30% of its variance.
To better understand the associations among study variables, a moderation model was tested. Subjective happiness was included as independent variable, depression, anxiety, and stress were included as dependent variable, and self-compassion was included as moderator. Results showed that self-compassion did not moderate the association between subjective happiness and depression (interaction term=.04, p=.513), anxiety (interaction term=.05, p=.373), or stress (interaction term=.04, p=.615).
Discussion
The aim of the study was to examine the efficacy of a relaxation protocol on depression, anxiety and stress in a sample of university students (aim 1); additionally, it was also an objective to explore the relationship between depression, anxiety, and stress, self-compassion and subjective happiness (aim 2).
With regard to the first aim, the hypothesis was not confirmed. Participants in the relaxation protocol group did not experience less depression, anxiety or stress. On the contrary, when the three groups were compared (from pre-test to follow-up), significant differences were only found between the experimental group and the passive control group only in anxiety and stress, but in the opposite direction. Indeed, participants in the experimental group experienced growth in anxiety and stress (but not in depression). This is a surprising result since previous studies have found positive effects of the AT in both university students (Kanji et al., 2006; Lim & Kim, 2014; Scholz et al., 2016) and other populations (Farnè & Gnugnoli, 2000; Farnè & Jimenez-Muñoz, 2000; Murakami et al., 2006; Yurdakul et al., 2009). In one study, no differences were found between participants in the AT and participants in the control group (Atkins & Hayes, 2019). However, we did not find any study in which depression, anxiety or stress become higher after the AT.
One possible explanation for this finding may be related to the experience of secondary effects after relaxation, as suggested by Lazarus and Mayne (1990). According to these authors, relaxation training may induce unpleasant sensations such as weight, heat, tingling, numbness, dizziness, feelings of physical and psychological vulnerability, irritability, fear of losing control and paradoxical increase in tension. Also, in another study (Heide, 1981), most of the participants of a relaxation intervention (with both an active and a passive method to induce relaxation) experienced an increase in tension.
Other authors suggest that participants’ previous experience, beliefs and expectations may influence negatively the results obtained with relaxation training by generating anxiety. The lack of experience can lead to questions regarding the method itself and its efficacy. According to Goldberg (1982), the assessment of participants’ expectations is an important step because positive expectations are likely to promote the training of the technique and, consequently, lead to better results. This author also refers that the assessment of mental state to evaluate self-regulatory techniques may be a problem because participants may pretend they are involved when they are not. Additionally, a brief exposure to the technique, which was the case of this intervention, can also lead to null or even negative outcomes (Abuín, 2016). As Luthe (1963) refers, the autogenic training is not suitable for individuals with a lack of motivation to improve their well-being. While the participation in our sessions was voluntary, some issues or personal characteristics may put into question their adherence to this relaxation practice (e.g., concentration ability) as found in a previous study (Houghton, 1996).
Moreover, while the intervention of this study followed the six exercises originally proposed by Schulz, other exercises were also included (e.g., breathing, guided imagery). Thus, this intervention was adapted which can limits the results obtained. Also, the interventionist experience with autogenic training can be an issue. According to different authors (Goldberg, 1982; Kanji & Ernst, 2000), results are influenced by the experience of the interventionist. In this study, despite the supervision of two seniors, the interventionist had little experience in autogenic training which can impact the results.
It is important to note that follow-up assessments occurred in a critical period for university students, that is at the end of the semester when they have to do final evaluations and deliver final academic works. It is possible to argue that the potential benefits of the intervention could be outshined by this challenging period. Also, at the beginning of the study, participants did not experience clinically significant depression, anxiety or stress, which makes it difficult to improve their psychological well-being.
With regard to aim 2, we found that self-compassion and subjective happiness were associated with depression, anxiety, and stress. These results are in accordance with the literature. For instance, Barnard and Curry (2011) found, in a sample of American university students, that self-compassion, life satisfaction and subjective happiness were positively associated, and that life-satisfaction and subjective happiness were likely to facilitate self-compassion. Also, Bluth and Eisenlohr-Moul (2017) found that mindfulness (a component of self-compassion) is likely to reduce rumination that is usually linked to anxiety, depression and stress. Thus, by directing individuals’ attention to the present moment and to physical sensations, depression, anxiety and stress would be reduced.
Finally, contrary to our expectations, self-compassion did not moderate the association between subjective happiness and depression, anxiety, or stress. This result can be related to the low levels of depression, anxiety and stress and the moderate levels of self-compassion and subjective happiness experienced by the participants. Thus, future studies should explore the moderator role of self-compassion in a sample with clinically significant depression, anxiety and stress.
Limitations and future directions
It is important to acknowledge the limitations of the present study. First, the protocol employed was brief since it included only six sessions. While some studies have shown that very brief interventions can be effective (e.g., see Kanji & Ernst, 2000 for more details), other authors suggest that at least eight to 12 sessions are needed to allow participants to learn the technique and lead to positive benefits (e.g., Linden, 1994). It is possible that for these specific participants and context, this number of sessions can be insufficient to produce benefits - but this is only one possible explanation. For this reason, future studies with university students should test the efficacy of longer interventions. Also, in order to be effective, it is recommended that participants train the technique on a regular and daily basis (Abuín, 2016; Krampen, 1996). In this study, no control was made regarding participants’ training of the technique outside the session (e.g., at home). Additionally, the autogenic training was offered in a group format. What may makes it difficult to adequate the intervention to the individuals’ needs and characteristics.
In terms of methodology, the efficacy of the study was assessed only using self-report measures, which can lead to participants’ biases. Future studies should assess its efficacy also using a qualitative approach (e.g., interviews with participants to explore perceived benefits or (un)helpful aspects of the therapy). Additionally, other variables should be included; while this protocol seems ineffective in improving depression, anxiety, and stress, it could contribute to improve other areas of psychological functioning in university students (e.g., emotion regulation, resilience, among others). For this reason, future studies should explore how this protocol impacts other variables.
Finally, most of the participants were women which limits conclusions with the minimum required of 41 participants in one arm of the RCT. Therefore, future studies should include larger and more heterogeneous samples (including more men) in each arm and, eventually, explore the moderating role of sex in the efficacy of relaxation training men and women may differ in their reaction to the relaxation protocol.
Conclusion
This study did not gather evidence on the efficacy of the relaxation protocol in reducing depression, anxiety and stress among university students. However, further studies are needed to better assess the potential benefits of relaxation within this population. Studies with larger samples, samples with clinically significant depression, anxiety or stress, and longer interventions will offer a more definitive view of the effects of this technique.

