










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
Print version ISSN 0872-0169
Port J Nephrol Hypert vol.27 no.4 Lisboa Dec. 2013
EDITORIAL
Evolution of the diagnostic criteria of T-cell-mediated rejection of renal allografts: Banff classification updates II
Muhammed Mubarak, Javed I. Kazi
Histopathology Department, Sindh Institute of Urology and Transplantation (SIUT), Karachi, Pakistan
ABSTRACT
The allo-specific immune responses to transplanted tissues or organs represent one of the most formidable challenges in the field of transplantation. Traditionally, cell-mediated alloimmune responses were considered the preeminent cause of rejection and have remained the focus of immunosuppressive drugs during the last several decades. More recently, attention has also been directed to the alloantibody-mediated damage and the innate immune system in initiating and effecting the immune injury to the transplanted organs. As a corollary to the above considerations, the earlier Banff classifications focused more on diagnosing and categorizing cellular rejection. There have occurred some significant changes in the cell-mediated rejection in recent Banff updates, but the changes are not as drastic or widespread, as those of the antibody-mediated rejection. Acute/active cell-mediated rejection may occur early or considerably late after renal transplantation. In this context, the terms of acute and chronic are not synonymous to their traditional connotations in pathology in terms of speed or duration of reaction. Acute rejection may occur many years after transplantation, and conversely, chronic changes may be present in the graft from the outset, derived from donor changes. Acute/active cell-mediated rejection, although markedly reduced in recent years, still remains one of the common causes of both acute and chronic renal allograft injury and dysfunction throughout the world. Luckily, a vast majority of cases of acute/active cell-mediated rejection respond rapidly and completely to the conventional anti-rejection treatment. In spite of this, it remains one of the most important causes of graft loss, especially in the long-term. Renal allograft biopsy still remains the gold standard test for an accurate diagnosis and categorization of cell-mediated rejection. A standardized approach to renal biopsy study is necessary if the full benefits of this invasive procedure are to be realized. Prior to the early 1990s, there were no uniformly accepted criteria for the diagnosis and classification of renal allograft pathology in general and rejection in particular. During early 1990s, a group of dedicated nephropathologists, clinicians and basic scientists set out to standardize the histopathological study of renal allograft biopsies for the uniform reporting of the pathological lesions across the world. These efforts have continued since then and have resulted in marked refinements in the diagnostic criteria and categories of rejection observed on renal allograft biopsies. The present paper forms the second attempt of the series to address the evolutionary changes in the diagnostic criteria and the classification of the rejection process on renal allograft biopsies as these took place over the years since the early 1990s.
An earlier paper described in detail the changes that occurred in the category of antibody-mediated rejection. In this paper, we will discuss the changes that have occurred in the diagnosis and categorization of cell-mediated rejection and the focus, as in previous paper, will be on the morphological findings as observed on renal allograft biopsies.
Key words: Banff schema; borderline changes; cell-mediated rejection; kidney transplantation; T cells.
The process of alloimmune rejection of the allografts represents one of the formidable challenges in the field of transplantation1. The rejection process may be mediated by the cytotoxic T lymphocytes or the antibodies, either solely or more commonly, in a variable combination of both. The components of the innate immune system also play an indispensable role in the rejection process at all stages of its evolution2.
Historically, the process of allograft rejection was classified into hyperacute, acute, and chronic types, depending on the speed and timing of the rejection development with no consideration of the underlying pathogenetic mechanisms2. Before the early 1990s, there was no single internationally agreed upon system for the standardized reporting of the pathological lesions on renal allograft biopsies3-9. Different renal transplant pathologists used different approaches for the diagnosis and classification of renal allograft pathology2-9.
The Banff classification represented the first attempt to formulate an international, consensusbased and structured classification system for the diagnosis and categorization of renal allograft biopsy pathology with a particular focus on the development of the morphological criteria for the diagnosis and classification of rejection9-14. In this regard, the first Banff meeting was held at Banff, Alberta, Canada on August2-4, 1991 and the first publication that narrated the outcome of the meeting appeared in 1993 and is known as Banff 93 classification12. Subsequent follow-up meetings have taken place every two years, mostly in the original country of the meeting but, more recently, in some other places of the world, to fine tune and adapt the classification to the latest progresses and advances in the field of transplant pathology13,14. Most of the meetings have been followed by updates and revisions in the form of papers in international peer-reviewed journals of nephrology and transplantation13-15. There have occurred marked changes in both the nomenclature and the classification of the rejection process, but the basic structure of the Banff schema has remained the same2,10,13-15. The first major and significant reshuffling of the original Banff classification occurred in 1997 with the merger and combination of Banff 93-95 classification and the National Institutes of Health (NIH)-sponsored Collaborative Clinical Trials in Transplantation (CCTT) modification, the two most widely used classifications in both clinical trials and centre practice at that time15,16.
Since then, Banff 97 working classification of renal allograft pathology has served as an international foundation for both the routine reporting of renal transplant pathology and the international clinical trials2,14.
It is apparent from a perusal of the earlier versions of the Banff schema that the main focus of these was on the diagnosis and categorization of acute/active cell-mediated rejection12,15. In fact, this focus on cellular rejection overshadowed the characterization and recognition of antibody-mediated rejection (ABMR) in the earlier days of the Banff meetings2. However, more recently, with an increasing recognition and reporting of ABMR, major and drastic changes have occurred in the diagnostic criteria and classification of this category2,17-21. On the other hand, the category of cell-mediated rejection has lagged behind in this context. In fact, the most important changes in this category also occurred during the early Banff meetings12,15,16. More recent updates have made only minor changes in the nomenclature of the category, rather than any drastic changes in the morphological criteria or subcategorization of this entity.
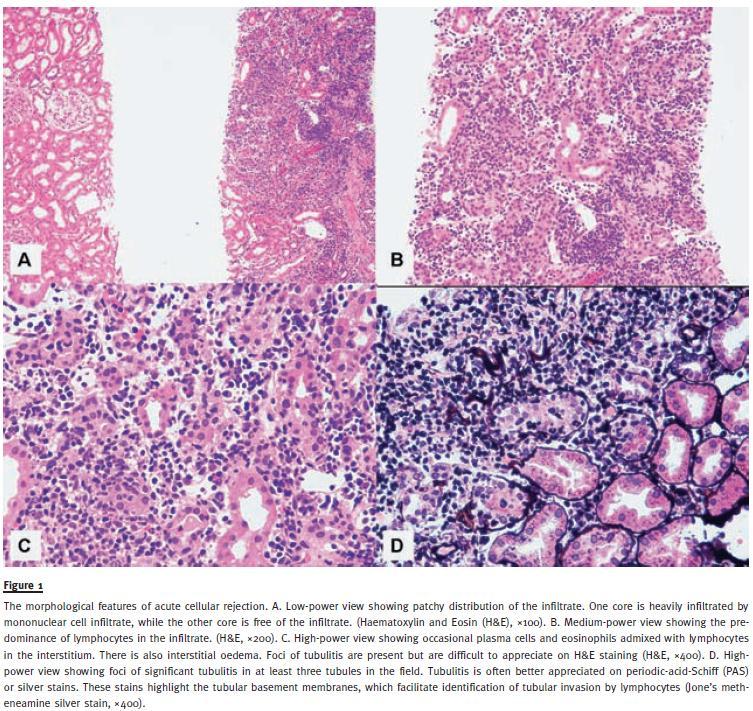
As noted above, the main focus of the first Banff classification was on the diagnosis and classification of acute/active cell-mediated rejection12. This type of rejection is characterized by infiltration of mononuclear cells, mostly T lymphocytes and macrophages, firstly in the interstitium, followed by attack of these cells on the tubules or the larger vessels (Fig. 1).
Thus, the targets of cellular rejection are different from those of ABMR. Prior to Banff classification, the presence of a few lymphocytes anywhere in the biopsy was usually considered as an indication of rejection. However, Banff made several important and new contributions to the diagnosis and standardization of morphological criteria of rejection diagnosis12.
It introduced for the first time a category of borderline changes. It also set a minimum threshold for a confident diagnosis of acute/active cell-mediated rejection. It also recognized the importance of the location of the inflammatory cell infiltrate in the biopsy12,15. It should be noted, as will become evident later on, that the above criteria and thresholds, are required for the diagnosis of tubulointerstitial or type I rejection. The rationale for creating the borderline changes category is that the morphological appearances of the rejection process develop gradually, so it is not surprising that in centres where biopsies are done early after graft dysfunction, pathologists often feel difficulty in definitively diagnosing rejection, owing to the inflammatory and tubulitis scores not reaching the threshold of rejection diagnosis22,23.
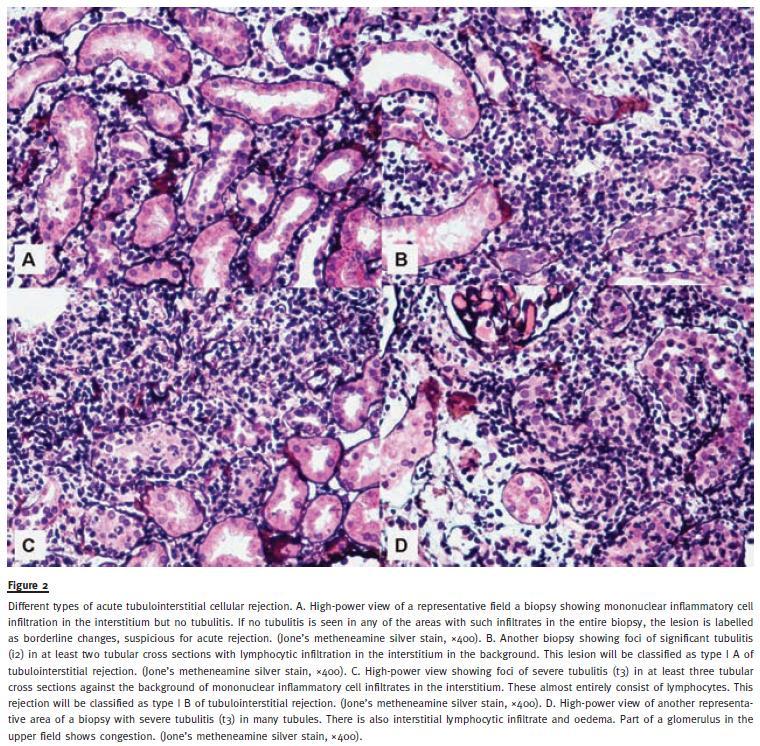
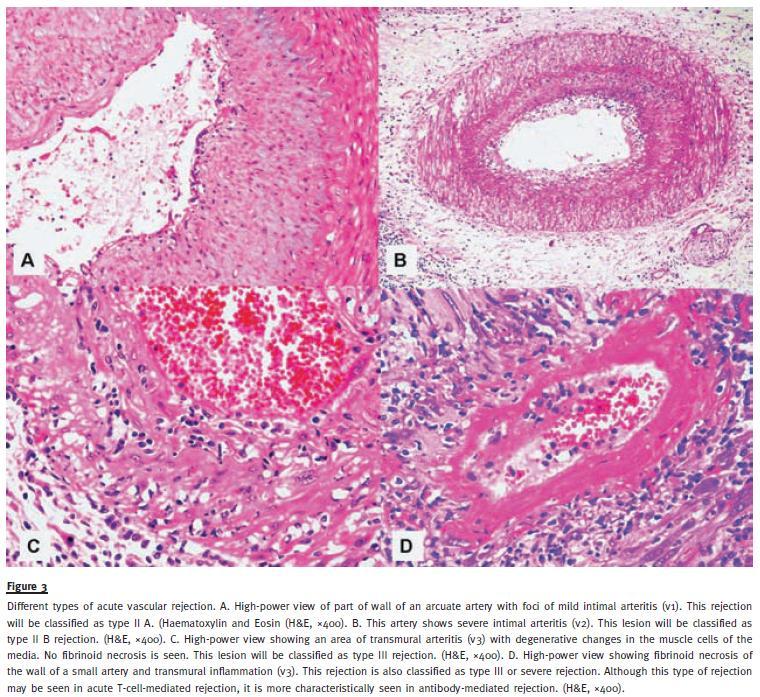
There is no borderline category for vascular or type II rejection and presence of even one lymphocyte in the intima is sufficient to diagnose a case as vascular rejection. However, the lymphocytic infiltration in the interstitium and tubulitis, especially of mild degree, are not specific for rejection and can be seen in other conditions. In order to avoid a high false positive rate of rejection diagnosis, the Banff schema set the minimum threshold of rejection diagnosis at i2 and t2, as illustrated in Fig. 2. On the other hand, higher degrees of both interstitial inflammation and tubulitis are relatively specific for rejection diagnosis24-26.Regarding the classification of rejection, the first Banff classification categorized acute/active rejection into three grades of increasing severity12. However,both the tubulointerstitial and vascular rejections were lumped together in this schema. The grades were: grade I or mild, grade II or moderate and grade III or severe (shown in Table I). Little consideration was given to the underlying pathogenetic basis of rejection in this categorization2,12. The first major reshuffle in this category took place in Banff 97 meeting, when investigators using the Banff 93 classification and CCTT classification met together and adapted the Banff 97 classification with significant contributions from the CCTT classification, which emphasized the pathogenetic basis for the classification of cellular rejection15,16. Banff 97 classification categorized acute/active rejection into types and subtypes instead of grades (Table II). The major changes in Banff 97 included the separation of type I or tubulointerstitial rejection from vascular or type II rejection15. Type III rejection was categorized separately as in Banff 93 classification (Fig. 3). This change represented the flexibility of the Banff group to accommodate the views of investigators using CCTT classification and also assimilate the experience from newer studies showing that vasculitis per se has implications for the response to therapy and/or graft survival15,16.
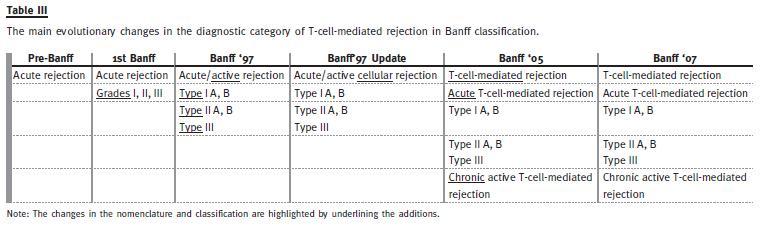
Banff 97-update, published in 2003, maintained the category of borderline changes, as all the subsequent updates of the classification21. With significant changes in the category of ABMR in this classification, however, the category of acute/active rejection was renamed as acute/active cellular rejection, to emphasize its distinction from ABMR. The typing and subtyping, however, remained the same as in Banff 97 classification21. No changes occurred in the nomenclature or classification of this category in Banff 2003 meeting27. The name of the category was again changed to T-cell-mediated rejection (TCMR) in Banff 2005 update28. This time, it was further divided into acute TCMR, which now included all the subtypes of acute/active cellular rejection of Banff 97-update, and the chronic active TCMR. The later was defined by the presence of chronic allograft arteriopathy28.
Banff 2007 classification added a new lesion score, termed ti (total interstitial inflammation score) to the schema. The scoring of the lesion was made optional in routine practice as the true significance of this is not known at present, but the pathologists were encouraged to note down this score in their reports. The lesion will be assessed in future meetings as the data accumulate on this variable. No change was made in lesion scoring of i-scoring29. A tabulated summary of the changes in the nomenclature and classification of cellular rejection is shown in Table III. Banff 09 and Banff 2011 meetings did not make any alterations in the criteria of diagnosis or classification of cellular rejection30,31.
It is apparent from the above discussion and the illustrations that the mainstay for the diagnosis and classification of cellular rejection has been the morphology with little help from ancillary techniques of immunohistochemistry (IHC) or electron microscopy (EM). More recently, attention has been focused towards the identification of molecular markers of acute cellular rejection with promising results in single centre studies29-31.
Multicentre trials and standardization of the methodology represent future challenges for the Banff group. The molecular data may be combined with the morphological data in the Banff classification in near future to increase the accuracy of diagnosis and classification of rejection29-31.
In conclusion, the development of the Banff classification of the renal allograft pathology has allowed the standardization of approaches to rejection diagnosis and classification and reduced interobserver and interinstitutional variation. The mainstay of the diagnosis and classification of cellular rejection is still the morphology. Molecular profiles may help fine tune the diagnosis and classification criteria in near future.
References
1. Hariharan S, Johnson CP, Bresnahan BA, Taranto SE, McIntosh MJ, Stablein D. Improved graft survival after renal transplantation in the United States; 1988-1996. N Eng J Med 2000;342(9):605-612. [ Links ]
2. Mubarak M, Kazi JI. Evolution of the diagnostic criteria of antibody-mediated rejection of renal allografts: Banff classification updates. Port J Nephrol Hypert (in press). [ Links ]
3. John R, Herzenberg AM. Our approach to a renal transplant biopsy. J Clin Pathol 2010; 63(1):26-37. [ Links ]
4. Gaber LW. Role of renal allograft biopsy in multicentre clinical trials in transplantation. Am J Kidney Dis 1998;31(6 Suppl 1):S19–25. [ Links ]
5. Al-Awwa IA, Hariharan S, First MR. Importance of allograft biopsy in renal transplant recipients. Am J Kidney Dis 1998;31(6 Suppl 1):S15–18. [ Links ]
6. Parfrey PS, Kuo YL, Hanley JA, et al, The diagnostic and prognostic value of renal allograft biopsy. Transplantation 1984;38(6):586–590. [ Links ]
7. Pascual M, Vallhonrat H, Cosimi AB, et al. The clinical usefulness of the renal allograft biopsy in the cyclosporine era: a prospective study. Transplantation 1999; 67(5):737-741. [ Links ]
8. Matas AJ, Sibley R, Mauer M, Sutherland DE, Simmons RL, Najarian JS. The value of needle renal allograft biopsy. I. A retrospective study of biopsies performed during putative rejection episodes. Ann Surg 1983;197:226–237. [ Links ]
9. Matas AJ, Tellis VA, Sablay L, Quinn T, Soberman R, Veith FJ. The value of needle renal allograft biopsy. III. A prospective study. Surgery 1985;98(2):922–6. [ Links ] [ Links ]
11. Seron D, Anaya F, Marcen R, et al. Guidelines for indicating, obtaining, processing and evaluating kidney biopsies. Nefrologia 2008;28(4):385-396. [ Links ]
12. Solez K, Axelsen RA, Benediktsson H, et al. International standardization of criteria for the histologic diagnosis of renal allograft rejection: the Banff working classification of kidney transplant pathology. Kidney Int 1993;44(2):411-422. [ Links ]
13. Weening JJ. The art of classifying renal allograft pathology. Nat Clin Pract Nephrol 2008;4(8):420-421. [ Links ]
14. Solez K, Racusen LC. The Banff classification revisited. Kidney Int 2013;83(2):201-206. [ Links ]
15. Racusen LC, Solez K, Colvin RB, et al. The Banff 97 working classification of renal allograft pathology. Kidney Int 1999;55(2):713-723. [ Links ]
16. Colvin RB, Cohen AH, Saiontz C, et al. Evaluation of pathologic criteria for acute renal allograft rejection: reproducibility, sensitivity, and clinical correlation. J Am Soc Nephrol 1997;8(12):1930-1941. [ Links ]
17. Feucht HE, Felber E, Gokel MJ, et al. Vascular deposition of complement-split products in kidney allografts with cell-mediated rejection. Clin Exp Immunol 1991;86(3):464-470. [ Links ]
18. Collins AB, Schneeberger EE, Pascual MA, et al. Complement activation in acute humoral renal allograft rejection: diagnostic significance of C4d deposits in peritubular capillaries. J Am Soc Nephrol 1999;10(10):2208-2214. [ Links ]
19. Mauiyyedi S, Pelle PD, Saidman S, et al.Chronic humoral rejection: identification of antibody-mediated chronic renal allograft rejection by C4d deposits in peritubular capillaries. J Am Soc Nephrol 2001;12(3):574-582. [ Links ]
20. Mauiyyedi S, Crespo M, Collins AB, et al. Acute humoral rejection in kidney transplantation: II. Morphology, immunopathology, and pathologic classification. J Am Soc Nephrol 2002;13(3):779-787. [ Links ]
21. Racusen LC, Colvin RB, Solez K, et al. Antibody-mediated rejection criteria –an addition to the Banff 97 classification of renal allograft rejection. Am J Transplant 2003;3(6):708-714. [ Links ]
22. Kazi JI, Furness PN, Nicholson M. Diagnosis of early acute renal allograft rejection by evaluation of multiple histological features using a Bayesian Belief Network. J Clin Pathol 1998;51(2):108-113. [ Links ]
23. Furness PN, Kirkpatrick U, Taub N, Davies DR, Solez K. A UK-wide trial of the Banff classification of renal transplant pathology in routine diagnostic practice. Nephrol Dial Transplant 1997;12(5):995-1000. [ Links ]
24. Furness PN, Kazi J, Levesley J, Taub N, Nicholson M. A neural network approach to the diagnosis of early acute allograft rejection. Transplant Proc 1999;31(8):3151. [ Links ]
25. Furness PN, Levesley J, Luo Z, et al. A neural network approach to the biopsy diagnosis of early acute renal transplant rejection. Histopathology 1999;35(5):461-467. [ Links ]
26. Kazi J, Mubarak M. Biopsy findings in renal allograft dysfunction in a live related renal transplant program. J Transplant Tech Res 2012; 2:108. [ Links ]
27. Racusen LC, Halloran PF, Solez K. Banff 2003 meeting report: new diagnostic insights and standards. Am J Transplant 2004;4(10):1562-1566. [ Links ]
28. Solez K, Colvin RB, Racusen LC, et al. Banff 05 Meeting Report: differential diagnosis of chronic allograft injury and elimination of chronic allograft nephropathy (CAN). Am J Transplant 2007;7(3):518-526. [ Links ]
29. Solez K, Colvin RB, Racusen LC, et al. Banff 07 classification of renal allograft pathology: updates and future directions. Am J Transplant, 2008;8(4):753-760. [ Links ]
30. Sis B, Mengel M, Haas M, et al. Banff 09 Meeting Report: antibody mediated graft deterioration and implementation of Banff working groups. Am J Transplant 2010;10(3):464-471. [ Links ]
31. Mengel M, Sis B, Haas M, et al. Banff 2011 Meeting Report: new concepts in antibodymediated rejection. Am J Transplant 2012;12(3):563-570. [ Links ]
Prof. Dr. Muhammed Mubarak
Histopathology Department,
Sindh Institute of Urology and Transplantation,
Karachi-74200, Pakistan,
Email address: drmubaraksiut@yahoo.com
Conflict of interest statement: None declared.
Received for publication: 06/08/2013 Accepted: 17/10/2013


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}