










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.28 no.3 Lisboa set. 2014
ORIGINAL ARTICLE
Clinicopathological correlations in proteinuric diseases: presenting features of patients with minimal change disease, focal and segmental glomerulosclerosis and membranous nephropathy
Correlações clínico -patológicas em doenças proteinúricas: características à apresentação dos doentes com doença de lesões mínimas, glomeruloesclerose segmentar e focal e nefropatia membranosa
Marta Neves, Luis Rodrigues, Helena Sa, Jorge Pratas, Mario Campos
Department of Nephrology, Centro Hospitalar e Universitário de Coimbra. Coimbra, Portugal.
ABSTRACT
Background: Some clinical and laboratory features may provide clues to the diagnosis of specific glomerular diseases. However, the kidney biopsy remains the gold standard in the diagnosis of parenchymal disease. Aim: To compare presenting clinical and laboratory features and report outcomes of adult patients with proteinuria diagnosed with primary minimal change disease (MCD), focal and segmental glomerulosclerosis (FSGS), and membranous nephropathy (MN). Subjects and Methods: Retrospective study of 143 patients over the age of eighteen years diagnosed with primary MCD, FSGS or MN, between 1981 and 2009. The groups were compared regarding presenting features and outcomes. Results: The most common glomerulopathy was MN (49.7%), followed by MCD (25.2%) and FSGS (25.2%). Statistically significant differences (p < 0.05) were found between the three groups regarding proteinuria, serum albumin, total cholesterol and serum creatinine higher than 1.5 mg/dl at the time of kidney biopsy, as well as the motive for the biopsy. No statistical differences were found between the three histological groups regarding remission at the end of the follow-up. Statistically significant differences (p < 0.05) were determined between the three groups regarding time to partial and complete remission, proteinuria and serum albumin at the final evaluation, and infectious complications. Conclusions: Patients with MCD presented lower serum albumin and higher levels of 24 -hour proteinuria and total cholesterol than the other groups. Patients with MCD achieved remission sooner, but suffered more infectious complications than those with FSGS or MN. In turn, patients with FSGS had higher proteinuria at the final evaluation and a trend towards the need for long-term RRT.
Key-Words: Focal and segmental glomerulosclerosis; membranous nephropathy; minimal change disease; proteinuria.
RESUMO
Introdução: Algumas características clínicas e laboratoriais podem fornecer pistas para o diagnóstico de doenças glomerulares específicas. No entanto, a biópsia renal continua a ser o método padrão para o diagnóstico de doenças do parênquima renal. Objectivo: Comparar características clínicas e laboratoriais e reportar a evolução de adultos com proteinúria diagnosticados com doença de lesões mínimas (DLM), glomeruloesclerose segmentar e focal (GESF) e nefropatia membranosa (NM) primária. Material e Métodos: Estudo retrospectivo de 143 doentes com idade superior a dezoito anos diagnosticados com DLM, GESF ou NM primária entre 1981 e 2009. Os grupos foram comparados quanto às características à apresentação e evolução clínica. Resultados: A glomerulopatia mais frequente foi a NM (49.7%), seguida pela DLM (25.2%) e GESF (25.2%). Foram encontradas diferenças estatisticamente significativas (p < 0.05) entre os três grupos em relação à proteinúria, albumina sérica, colesterol total e creatinina sérica superior a 1.5 mg/dl no momento da biópsia renal, assim como o motivo para a realização da biópsia. Não foram encontradas diferenças estatísticas entre os três grupos histológicos em relação à remissão no final do seguimento. Diferenças estatisticamente significativas (p < 0.05) foram encontradas entre os três grupos em relação ao tempo até remissão parcial e completa, proteinúria e albumina sérica na avaliação final, e complicações infecciosas. Conclusões: Doentes com DLM apresentaram menores níveis de albumina sérica e níveis mais elevados de proteinúria de 24 horas e colesterol total comparado com os outros grupos. Doentes com DLM atingiram remissão mais cedo, no entanto sofreram mais complicações infecciosas do que aqueles com GESF ou NM. Por sua vez, os doentes com GESF apresentaram valores de proteinuria mais elevados na avaliação final e uma tendência para necessidade de TSFR a longo prazo.
Palavras-chave: Doença de lesões mínimas; glomeruloesclerose segmentar e focal; nefropatia membranosa; proteinúria.
INTRODUCTION
Glomerular diseases are classified as primary (or idiopathic) and secondary according to the absence or presence of a causal disease or factor, respectively. The association between proteinuria, glomerular diseases and clinical features of the nephrotic syndrome has become recognized as a formal entity over the past two centuries1. Some clinical and laboratory features may provide clues to the underlying kidney disease, and some clinicians seem tempted to use these features in an attempt to speculate about the diagnosis. However, the kidney biopsy remains the gold standard in the official diagnosis of a specific primary or secondary parenchymal disease, also playing an important role in defining treatment choice and prognosis2.
The aim of this single-centre retrospective study was to compare clinical and laboratory presentations and report on outcomes of adult patients with proteinuria ultimately diagnosed with primary minimal change disease (MCD), focal and segmental glomerulosclerosis (FSGS), and membranous nephropathy (MN).
SUBJECTS AND METHODS
We analysed all 216 patients presenting at the Nephrology Department of a tertiary university hospital serving two million citizens, who underwent a percutaneous ultrasonography-guided native kidney biopsy for the study of proteinuric conditions, between the 1st January 1981 and the 31st December 2008, and in whom primary MCD, FSGS or MN was detected. Kidney biopsies were processed for light and immunofluorescence microscopy according to standard techniques.
Exclusion criteria comprised 0f: age under 18 years, identification of an underlying secondary cause or systemic disease for the glomerular disease, follow-up of less than three months, transfer after kidney biopsy to local hospitals closer to the patients´ residence or insufficient data in hospital records.
Demographic and clinical data were registry –based and retrospectively collected. The data included parameters such as gender, age at kidney biopsy, reason for kidney biopsy, oedema, hypertension, dyslipidaemia, microscopic or macroscopic haematuria, presence of interstitial fibrosis on kidney biopsy, use of immunosuppressive and/or conservative therapy with angiotensin-converting–enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARBs), diuretic use, statin use, time to partial remission, time to complete remission, number of relapses per year of follow-up, thrombotic complications, infectious complications, evolution to chronic kidney disease (CKD) and death. Documented laboratory data were based on blood and urine samples collected for routine nephrology consultations and included: serum creatinine, serum albumin, total cholesterol, triglycerides and 24-hour urinary protein excretion. Laboratory data shown were recorded at the time of diagnosis and at final evaluation at our institution.
Hypertension was defined as a systolic blood pressure above 140mmHg or diastolic blood pressure above 90mmHg noted in at least two consecutive office or home measurements with a one -week interval and/or need for antihypertensive medication (not including ACEi or ARBs). Haematuria was defined as more than five red blood cells per high -power field.
Nephrotic syndrome was defined as proteinuria ≥ 3.5 g/24h, accompanied by hypoalbuminaemia (≤ 3.0 g/dl), dyslipidaemia (total cholesterol ≥ 240 mg/dl and/or triglycerides ≥ 200 mg/dl) and peripheral oedema. Nephrotic-range proteinuria was defined as proteinuria ≥ 3.5 g/24h (without the remaining components of the nephrotic syndrome) and sub–nephrotic proteinuria was defined as proteinuria < 3.5 g/24h.
The urinary protein quantification closest to the date of the histologic diagnosis was used as proteinuria at diagnosis. Partial remission was defined as proteinuria between 0.5 and 3.5 g/24h with, at least, a 50% decrease in proteinuria compared to the initial presentation. Complete remission was defined as proteinuria < 0.5 g/24h with normal serum albumin.
Relapse was defined as a minimum of 50% increase in proteinuria after a partial or complete remission had been achieved, with or without hypoalbuminaemia.
CKD was defined as serum creatinine ≥ 1.5 mg/dl for longer than three consecutive months. Estimated glomerular filtration rate (eGFR) was calculated by using the modification of diet in renal disease (MDRD) formula.
Patients complying with the inclusion criteria were divided into three groups, according to the histologically-proven primary glomerulopathy diagnosed (MCD, FSGS and MN), and comparisons were made regarding presenting features and clinical outcomes.
All statistical analyses were performed using the commercially available SPSS® for Windows® (version 20.0, Chicago, IL, USA). Continuous variables are presented as mean ± standard deviation (SD) and median, and categorical variables as a percentage of the number of studied cases. Univariate testing of variables between the three independent groups was performed using the one-way ANOVA or Kruskal-Wallis for continuous variables and the χ2 test for nominal variables, as appropriate. All p-values were two -tailed and values less than 0.05 were considered statistically significant.
RESULTS
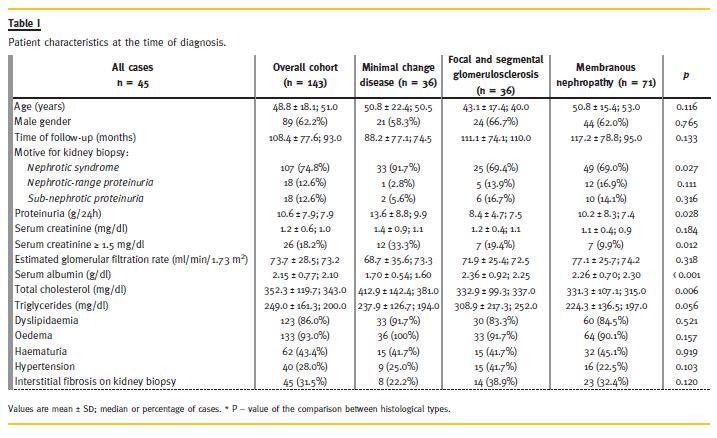
One hundred and forty -three patients met the inclusion criteria and, by the 30th September 2012, the mean follow -up period was 9.0 ± 6.5 years (minimum 4 months and maximum 30.5 years). The most common glomerulopathy was MN (n = 71; 49.7%), followed equally by MCD (n = 36; 25.2%) and FSGS (n = 36; 25.2%). Almost two -thirds of the patients were male, with a mean age of 48.8 years, ranging from 18 to 84 years of age. Table 1 summarises the characteristics at the time of diagnosis of the studied patients. At univariate analysis statistically significant differences (p < 0.05) were found between the three groups regarding proteinuria, serum albumin, total cholesterol and serum creatinine higher than 1.5mg/dl at the time of kidney biopsy, as well as the reason for the biopsy. Creatinine ≥ 1.5 mg/dl was seen in 26 patients (18.2%) at diagnosis: 33.3% of those with MCD; 19.4% of those with FSGS; and 9.9% of those with MN. Analysis of residuals and post hoc analysis determined that, statistically, patients with MCD presented more frequently with the nephrotic syndrome as the reason for kidney biopsy (91.7% vs. 69.4% with FSGS and 69.0% with MN), patients with MCD had significantly higher levels of 24 -hour proteinuria than those with MN or FSGS (13.6 ± 8.8 vs. 10.2 ± 8.3 and 8.4 ± 4.7 g, respectively), patients with MCD had significantly higher levels of total cholesterol than those with FSGS or MN (412.5 ± 142.4 vs. 332.9 ± 99.3 and 331.3 ± 107.1 mg/dl, respectively), and significantly lower levels of serum albumin on admission or before kidney biopsy were found in patients with MCD, compared to those with MN or FSGS (1.70 ± 0.54 vs. 2.26 ± 0.70 and 2.36 ± 0.92 g/dl, respectively).
Treatment choice was determined by the patient´s Nephrologist and influenced according to severity of disease and existing department protocols. Most patients with MCD received first -line immunosuppressive therapy with corticosteroids (n = 34; 94.4%) and conservative therapy with ACEi or ARBs (n = 28; 77.8%). Relapses occurred 0.3 ± 0.4 times per patient per year (minimum 0 and maximum 2.2) and second - or third -line immunosuppressive therapy was required in 15 patients (41.7%). Cyclophosphamide was the therapy of choice in 53.3% (n = 8) of the 15 patients requiring alternate therapies. Diuretics were used in 33 patients with MCD (91.7%) and statins in 19 patients (52.8%). More than half of the patients with FSGS received first -line immunosuppressive therapy with corticosteroids (n = 23; 63.9%) and most received conservative therapy with ACEi or ARBs (n = 35; 97.2%). Relapses occurred 0.2 ± 0.3 times per patient per year (minimum 0 and maximum 1.1) and second - or third -line immunosuppressive therapy was required in 17 patients (47.2%).
Cyclosporin A was the therapy of choice in 52.9% (n = 9) of the 17 patients requiring alternate therapies.
Diuretics were used in 27 patients with FSGS (75.0%) and statins in 20 patients (55.6%). Before 2001, the first-line choice for immunosuppressive therapy in MN at our department was corticosteroids (in 27 of 42 patients diagnosed during this period; 64.3%), and since then the first -line approach for immunosuppressive therapy included regimens containing cyclosporin A (with or without low -dose corticosteroid therapy) in 18 of the 29 patients diagnosed during this period (62.1%). Relapses occurred 0.2 ± 0.2 times per patient per year (minimum 0 and maximum 0.9) and a second course of immunosuppressive therapy was required in 23 patients (32.4%).
Cyclophosphamide was the therapy of choice in 30.4% (n = 7) of the 23 patients requiring alternate therapies, while 15 of the 23 patients (65.2%) repeated treatment with a second course of cyclosporine A -based therapy. Conservative therapy with ACEi or ARBs was employed in 61 patients (85.9%), diuretics were used in 58 patients (81.7%) and statins in 42 patients (59.2%) with MN.
After the first year of follow -up, 72.2% (n = 26) of patients with MCD had achieved complete remission and 13.9% (n = 5) were in partial remission, while five patients (13.9%) had not yet achieved remission. Of those patients with MCD not in remission after the first year, four progressed to CKD, probably reflecting a misdiagnosed FSGS due to sampling error or a subsequent progression to this histological pattern over time. At one year, 30.6% (n = 11) of patients with FSGS had achieved complete remission and 38.9% (n = 14) were in partial remission, while 11 patients (30.6%) had not yet achieved remission. Regarding MN, 33.8% (n = 24) of patients had achieved complete remission and 45.1% (n = 32) were in partial remission, while 15 patients (21.1%) had not achieved remission after one year of follow-up.
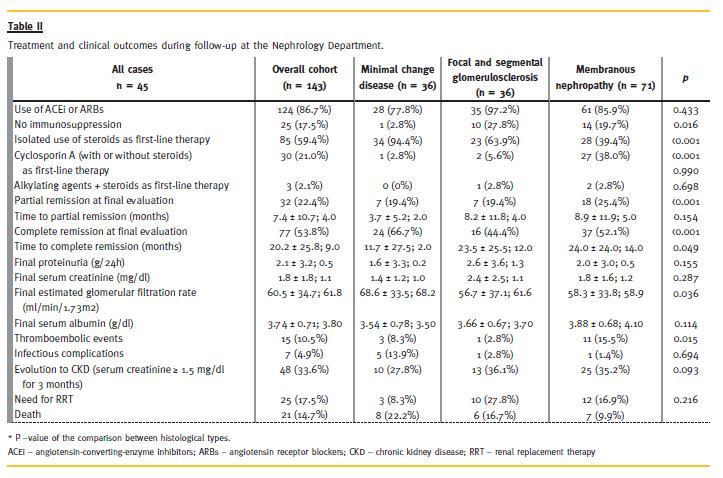
At the final evaluation (after 108.4 ± 77.6 months in the overall population), 109 patients (76.2%) were in remission: 32 (22.4%) in partial remission and 77 (53.8%) in complete remission. No statistical differences were found between the three histological groups regarding remission at the end of follow–up (partial remission in 19.4% of patients with MCD, 19.4% of patients with FSGS and 25.4% of patients with MN, p = 0.698; complete remission in 66.7% of patients with MCD, 44.4% of patients with FSGS and 52.1% of patients with MN, p = 0.154). Mean proteinuria at final evaluation was statistically different between the three groups (1.6 ± 3.3 in MCD vs. 2.6 ± 3.6 in FSGS vs. 2.0 ± 3.0 g/24h in MN, p = 0.049).
Clinical outcomes throughout follow -up are presented in Table 2. Univariate analysis determined statistically significant differences (p < 0.05) between the three groups regarding time to partial and complete remission, serum albumin and 24 -hour proteinuria at final evaluation, and infectious complications.
Analysis of residuals and post hoc analysis determined that patients with MCD took significantly less time to achieve documented partial remission than those with FSGS or MN (3.7 ± 5.2 vs. 8.2 ± 11.8 and 8.9 ± 11.9 months, respectively), with the same being determined for the time to documented complete remission (11.7 ± 27.5 vs. 23.5 ± 25.5 and 24.0 ± 24.0 months, respectively). Final serum albumin was significantly higher in patients diagnosed with MN compared to those with MCD and FSGS (3.88 ± 0.68 vs. 3.54 ± 0.78 and 3.66 ± 0.67 mg/dl, respectively) and proteinuria was significantly higher in those with FSGS at final evaluation as compared to those with MN and MCD (2.6 ± 3.6 vs. 2.0 ± 3.0 and 1.6 ± 3.3 g/24h, respectively). Patients with MCD also suffered more infectious complications than those patients with FSGS or MN (13.9% vs. 2.8% and 1.4%, respectively; p = 0.015), while, although not statistically significant, patients with MN experienced a significantly higher number of venous thromboembolic episodes compared to patients with MCD or FSGS (15.5% vs. 8.3% and 2.8%, respectively). A higher proportion of patients diagnosed with FSGS tended to require RRT, while a lower proportion of patients with MCD required dialysis or transplantation (27.8% vs. 8.3%, respectively; p = 0.093). Twelve patients diagnosed with MN (16.9%) required RRT sometime during follow-up.
DISCUSSION
The dawn of the percutaneous kidney biopsy in the 1950s allowed for an enhanced knowledge about glomerular disease and, consequently, a more directed therapeutic attitude1.
In our population, the most common primary glomerulopathy diagnosed was MN, which is among the most common causes of nephrotic syndrome in non-diabetic adults. At one time, it was the most common kidney biopsy diagnosis in adults (especially those over the age of 40 years) presenting with nephritic syndrome, but in the United States of America its relative frequency has declined, in part due to an increase in the relative frequency of FSGS3. Similarly to published studies concerning large series of kidney biopsies, this study also showed a male predominance for the studied glomerular diseases4,5,6. No significant differences were found between patients diagnosed with MCD, FSGS and MN regarding age or gender.
Nephrotic syndrome was statistically more common as the clinical indication for kidney biopsy in those patients ultimately diagnosed with MCD.
Minimal change disease is the most common cause of nephrotic syndrome in children, also posing as an important cause of primary nephrotic syndrome in adults of all ages7. Whereas hypertension, haematuria and kidney dysfunction are unusual in children, these features can be found in adults diagnosed with MCD, with modestly elevated creatinine in an average of 30 -40% of patients at presentation8-11.
In our study, hypertension was present in 25.0%, haematuria was seen in 41.7% and creatinine ≥ 1.5 mg/dl was seen in twelve patients (33.3%) at diagnosis.
In a retrospective review of 95 patients with adult-onset MCD, acute kidney dysfunction occurred in 24 of those patients and mean serum creatinine of the studied population was 1.4 mg/dl7. This reduction in GFR may be mediated, at least in part, by reduced glomerular permeability due to the foot process fusion that is representative of MCD9,11, although other factors, such transient ischaemic tubular injury, interstitial oedema and nephrotoxins, can also play a role. In our study, patients with MCD also showed significantly lower levels of serum albumin and higher levels of 24-hour proteinuria and total cholesterol at admission than those with either FSGS or MN.
Conservative therapy was used in more patients with FSGS and MN than with MCD (97.2% and 85.9% vs. 77.8%). Statistically, in more patients with FSGS and MN was there no employment of immunosuppressive therapies, as compared with those suffering from MCD (27.8% and 19.7% vs. 2.8%; p = 0.016).
Patients with MCD took significantly less time to achieve documented partial and complete remission than those with FSGS or MN. Patients younger than 16 years with MCD are known to remit rapidly – 50% respond within two weeks of initiation of therapy and almost all children remit within eight weeks.
Kidney biopsy is, therefore, rendered unnecessary in most children, unless indicated otherwise by the clinical course12. Adults tend to have a slower response to therapy and more than 25% of responders require three to four months or even longer to achieve complete remission8,13-16.
Remission was observed in 63.9% of patients with FSGS, similar to other observations in published studies17-19. In our study, a higher proportion of patients diagnosed with FSGS required RRT, while a lower proportion of patients with MCD required dialysis or transplantation (27.8% vs. 8.3%, respectively), however, this did not achieve statistical significance.
Of the 10 patients with FSGS needing RRT, nine had nephrotic-range proteinuria at the final evaluation and, of these, four had never achieved remission despite appropriate treatment. According to data from the United States Renal Data System, collected over 21 years, FSGS is the most common primary glomerular disease identified in patients with end -stage renal disease (ESRD) in the United States3.
Of the three patients with MCD requiring RRT, all had nephrotic-range proteinuria at final evaluation and, of these, one had never achieved partial or complete remission while another took 18 months to achieve the first documented partial remission, probably reflecting a misdiagnosed FSGS due to a sampling error or a subsequent progression to this histological pattern over time, since traditionally true MCD is not a cause of ESRD.
Complications of the nephrotic syndrome are a chief source of morbidity in patients diagnosed with primary glomerulonephritis20. Traditionally, MN has been implicated as a risk factor for venous thromboembolic complications (although thromboembolic events have been described in all patients with nephrotic syndrome, and the administration of steroids – the cornerstone of therapy for many of these conditions – may also increase the risk for thromboembolism). In our cohort, patients with MN experienced a higher number of venous thromboembolic episodes compared to patients with MCD or FSGS (15.5% vs. 8.3% and 2.8%, respectively; p = 0.114). In a study derived from the Toronto Glomerulonephritis Registry by Barbour et al.20, even after adjustment for proteinuria, albumin levels and history of cancer, the underlying histological diagnosis remained an independent risk factor for thromboembolic events (adjusted hazard ratio of 10.8 for MN, p = 0.002, and adjusted hazard ratio of 5.9 for FSGS, p = 0.02). Patients with MCD suffered statistically more infectious complications (three episodes of bacterial pneumonia, one episode of upper respiratory tract infection and one episode of bacterial meningitis, all in adults between the age of 36 and 82 years) than those patients with FSGS or MN. The predisposition to infection may be related to an accumulation of extracellular fluid (possibly due to more severe hypoalbuminaemia) and a number of immunologic factors, in addition to the use of immunosuppressive medications as recommended treatment7.
Several limitations of the study deserve comment. The results accrued from this study are restricted by the retrospective nature of the design and its location at a single medical centre. Another potential limitation arises from the decision to use serum creatinine to define CKD, however, altered renal tubular handling of creatinine in patients with nephrotic syndrome renders any creatinine -based estimated glomerular filtration rate formula potentially less valid21. Nonetheless, the authors chose to employ these formulas for complimentary information in the study. The authors chose not to analyse response to or effectiveness of therapy due to the non-uniform use of immunosuppressive agents (even within the same disease) and consequent difficulty in drawing conclusions concerning these outcomes.
In conclusion, significant differences were found between the three groups regarding 24 -hour proteinuria, serum creatinine ≥ 1.5 mg/dl, serum albumin and total cholesterol at the time of kidney biopsy: a larger proportion of patients with MCD presented with a serum creatinine ≥ 1.5 mg/dl and patients with MCD also presented lower serum albumin and higher levels of total cholesterol and proteinuria. Significant differences were also found between the three groups pertaining to motive for kidney biopsy, time leading to partial and complete remission and number of infectious complications: patients with MCD achieved partial and complete remission sooner, although they suffered more infectious complications. Although not statistically significant, in our studied population, patients with MN tended to suffer more venous thromboembolic events and more patients with FSGS tended to develop the need for long-term RRT. Regular clinical and laboratory evaluation of these patients is required since the response to therapy is not predictable, particularly in an older cohort.
Our findings reproduce the information obtained from the published literature. Despite encountering significant clinicopathological correlations between the three histological groups, clinical and laboratory data and their apparent associations with a parenchymal disorder do not distinguish the concerned entities and these features will never substitute the undeniable role of the kidney biopsy in providing a definitive histological diagnosis of glomerular disease.
References
1. Cattran DC. Historical aspects of proteinuria. Adv Chronic Kidney Dis 2011; 18(4): 224-232. [ Links ]
2. Morel -Maroger L. The value of renal biopsy. Am J Kidney Dis 1982; 1(4): 244-248. [ Links ]
3. Kitiyakara C, Eggers P, Kopp JB. Twenty-one-year trend in ESRD due to focal segmental glomerulosclerosis in the United States. Am J Kidney Dis 2004; 44(5): 815 -825. [ Links ]
4. Rivera F, López -Gómez JM, Pérez -García R; Spanish Registry of Glomerulonephritis. Frequency of renal pathology in Spain 1994 -1999. Nephrol Dial Transplant 2002; 17(9):1594 -1602.
5. Gesualdo L, Di Palma AM, Morrone LF, Strippoli GF, Schena FP; Italian Immunopathology Group, Italian Society of Nephrology. The Italian experience of the national registry of renal biopsies. Kidney Int 2004; 66(3):890-894. [ Links ]
6. Briganti EM, Dowling J, Finlay M, et al The incidence of biopsy -proven glomerulonephritis in Australia. Nephrol Dial Transplant 2001; 16(7): 1364 -1367. [ Links ]
7. Waldman M, Crew RJ, Valeri A, et al. Adult minimal -change disease: clinical characteristics, treatment, and outcomes. Clin J Am Soc Nephrol 2007; 2(3): 445 -453. [ Links ]
8. Nolasco F, Cameron JS, Heywood EF, Hicks J, Ogg C, Williams DG. Adult-onset minimal change nephrotic syndrome: a long-term follow-up. Kidney Int 1986; 29(6): 1215 -1223. [ Links ]
9. Drumond MC, Kristal B, Myers BD, Deen WM. Structural basis for reduced glomerular filtration capacity in nephrotic humans. J Clin Invest 1994; 94(3): 1187-1195. [ Links ]
10. Smith JD, Hayslett JP. Reversible renal failure in the nephrotic syndrome. Am J Kidney Dis 1992; 19(3): 201 -213. [ Links ]
11. Bohman SO, Jaremko G, Bohlin AB, Berg U. Foot process fusion and glomerular filtration rate in minimal change nephrotic syndrome. Kidney Int 1984; 25(4): 696 -700. [ Links ]
12. The primary nephrotic syndrome in children. Identification of patients with minimal change nephrotic syndrome from initial response to prednisone. A report of the International Study of Kidney Disease in Children. J Pediatr 1981; 98(4): 561 -564. [ Links ]
13. Nakayama M, Katafuchi R, Yanase T, Ikeda K, Tanaka H, Fujimi S. Steroid responsiveness and frequency of relapse in adult -onset minimal change nephrotic syndrome. Am J Kidney Dis 2002; 39(3): 503 -512. [ Links ]
14. Mak SK, Short CD, Mallick NP. Long -term outcome of adult-onset minimal-change nephropathy. Nephrol Dial Transplant 1996; 11(11): 2192 -2201. [ Links ]
15. Korbet SM, Schwartz MM, Lewis EJ. Minimal -change glomerulopathy of adulthood. Am J Nephrol 1988; 8(4): 291-297. [ Links ]
16. Fujimoto S, Yamamoto Y, Hisanaga S, Morita S, Eto T, Tanaka K. Minimal change nephrotic syndrome in adults: response to corticosteroid therapy and frequency of relapse. Am J Kidney Dis 1991; 17(6): 687-692. [ Links ]
17. Cattran DC. Are all patients with idiopathic focal segmental glomerulosclerosis (FSGS) created equal? Nephrol Dial Transplant 1998; 13(5): 1107-1109. [ Links ]
18. Tune BM, Kirpekar R, Sibley RK, Reznik VM, Griswold WR, Mendoza SA. Intravenous methylprednisolone and oral alkylating agent therapy of prednisone -resistant pediatric focal segmental glomerulosclerosis: a long -term follow-up. Clin Nephrol 1995; 43(2):84 -88. [ Links ]
19. Banfi G, Moriggi M, Sabadini E, Fellin G, Amico G, Ponticelli C. The impact of prolonged immunosuppression on the outcome of idiopathic focal -segmental glomerulosclerosis with nephrotic syndrome in adults. A collaborative retrospective study. Clin Nephrol 1991; 36(2): 53-59. [ Links ]
20. Barbour SJ, Greenwald A, Djurdjev O, et al. Disease-specific risk of venous thromboembolic events is increased in idiopathic glomerulonephritis. Kidney Int 2012; 81(2):190 -195. [ Links ]
21. Hofstra JM, Willems JL, Wetzels JF. Estimated glomerular filtration rate in the nephrotic syndrome. Nephrol Dial Transplant 2011; 26(2): 550-556. [ Links ]
Drª Marta Neves
Department of Nephrology, Centro Hospitalar e Universitário de Coimbra
Praceta Professor Mota Pinto
3000-075 Coimbra, Portugal
E-mail: martaraq_neves@hotmail.com
Conflict of interest statement: None declared.
Received for publication: 25/11/2013
Accepted in revised form: 11/08/2014


{kind=link}
{kind=link}