










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.28 no.3 Lisboa set. 2014
CASE REPORT
Fenofibrate-induced rhabdomyolysis in an adolescent with chronic renal failure and hypothyroidism
Rabdomiólise induzida por fenofibrato em adolescente com insuficiência renal crónica e hipotiroidismo
Filipa Carlota Marques1, Carolina Viveiro2, Isabel Castro3
1 Pediatria, Hospital São Francisco Xavier – Centro Hospitalar de Lisboa Ocidental. Lisboa, Portugal.
2 Pediatria, Hospital de Santo André – Centro Hospitalar de Leiria-Pombal. Leiria, Portugal.
3 Departamento da Área de Pediatria Médica; Unidade de Nefrologia CHLC, EPE – Hospital de Dona Estefânia. Lisboa, Portugal.
ABSTRACT
Background: Rhabdomyolysis is a condition defined by necrosis of muscle cell and release of its contents into the systemic circulation. The fibric acid derivative fenofibrate is indicated in the treatment of hyperlipidaemia in adults. Fenofibrate monotherapy-induced rhabdomyolysis is rare. The presence of chronic renal failure and hypothyroidism are among the primary factors for rhabdomyolysis.
Case: Our case study is about an adolescent with chronic renal failure, severe hypertriglyceridemia and hypothyroidism who developed rhabdomyolysis and irreversible deterioration of kidney function after monotherapy with fenofibrate. The patient required renal replacement therapy using haemodialysis and kidney transplant.
Conclusion: This case study is of the highest importance to warn against the adverse events associated with fenofibrate therapy and to alert to the need of a rigorous control of its use when risk factors are present.
Key-words: Chronic renal failure; fenofibrate; hypothyroidism; rhabdomyolysis
RESUMO
Introdução: A rabdomiólise é uma patologia definida pela necrose da célula muscular com posterior extravasão do seu conteúdo para a circulação sistémica. O fenofibrato é um derivado do ácido fíbrico indicado no tratamento da dislipidémia do adulto. A rabdomiólise provocada pelo fenofibrato em monoterapia é rara. A insuficiência renal crónica e o hipotiroidismo são factores precipitantes de rabdomiólise provocada pelo fenofibrato.
Caso clínico: Descrevemos o caso de uma adolescente com insuficiência renal crónica e hipotiroidismo que teve rabdomiólise após terapêutica com fenofibrato em monoterapia e agravamento irreversível da função renal com necessidade de hemodiálise e posterior transplante renal.
Conclusão: Este caso alerta para os efeitos adversos associados à utilização de fenofibrato e para a necessidade do seu controlo rigoroso sobretudo na presença de factores de risco.
Palavras-chave: Fenofibrato; hipotiroidismo; insuficiência renal crónica; rabdomiólise.
BACKGROUND
Rhabdomyolysis is a syndrome characterized by clinical and biochemical abnormalities resulting from necrosis of the muscle cells with release of its contents into the systemic circulation1. It presents a broad clinical spectrum from asymptomatic elevation of muscle enzymes to potentially life -threatening clinical situations, including electrolyte disturbances and acute renal failure (ARF)2. There are multiple potential inherited and acquired causes for rhabdomyolysis: strenuous exercise, trauma, ischaemia, infection, hereditary muscle enzyme deficiencies, hydroelectrolytic abnormalities, seizures, hypothyroidism, drugs and toxics3,4.
However, drug -induced rhabdomyolysis is rare5.
Fenofibrate is a fibric acid derivative indicated for use in the treatment of hypertriglyceridemia and mixed dyslipidemia used in adults, in mono-therapy or in combination with statins. The most common side-effects of fibrates include gastrointestinal and musculoskeletal symptoms, skin reactions, gallstones, fatigue, headaches and anxiety. Rhabdomyolysis is a rare, still very serious and potentially fatal side-effect2. Major risk factors for induced-fenofibrate rhabdomyolysis include comorbidities, such as renal or liver disease, hypothyroidism, diabetes mellitus, female gender, using higher doses of fenofibrate5 and advanced age (over 65 years).
Our case study presents a clinical history of an adolescent with chronic renal failure (CRF), severe hypertriglyceridemia and hypothyroidism who developed rhabdomyolysis after monotherapy with fenofibrate, resulting in an irreversible degeneration of renal function and subsequently the need for haemodialysis and posterior renal transplant.
CASE STUDY PRESENTATION
A 14-year-old female adolescent with a history of end -stage CRF of unknown aetiology, was referred to our Nephrology unit for evaluation for possible creation of an arteriovenous fistula for haemodialysis in the context of the renal function decline.
Her family history combines a mother with hypothyroidism, hypertension and controlled hypertriglyceridemia and a father with Crohns disease.
The patient is an only child, premature at gestational age of 32 weeks. Her mother was primigravida with a high-risk pregnancy due to hypertension and intrauterine growth restriction diagnosed during the 2nd trimester. For this reason, an emergency caesarean section for pre -eclampsia and fetal distress was performed. Apgar scores after 1 and 5 minutes were 4 and 8, requiring endotracheal intubation in the delivery room and positive –pressure ventilation. Afterwards she was admitted to the Neonatology Unit for eighty days, with the following diagnostic: jaundice, thrombocytopenia, hyaline membrane disease, atrial septal defect (ASD), and persistency of the arterial ductus requiring surgical ligation, heart and renal transitional failure. The ASD is currently small without haemodynamic significance.
At the age of 15 months, she was hospitalized due to acute pyelonephritis with Escherichia coli bacteraemia.
The patient was apparently well until the age of 5, when she was diagnosed with hypothyroidism (the perinatal screening was negative), hypercholesterolemia and hypertriglyceridemia associated with excessive weight. After an endocrinologist appointment, she initiated therapy with levothyroxine combined with proper diet.
Around the age of 7, she was diagnosed with CRF of unknown aetiology presenting a glomerular filtration rate (GFR) of 50 mL/1.73m2/min. Follow-up was made as an outpatient in the clinic of the local hospital until the age of 12, when she presented a GFR of 37.7 mL/1.73m2/min, requiring follow-up by the Nephrology Unit. Her clinical studies at the age of 12 did not show any renal malformations or reflexive pathology. The renal echography revealed little, hyperecogenic kidneys, without corticomedular differentiations.
DMSA renal scan revealed bilateral hypofunction and a right polar inferior renal scar. The renal biopsy performed in the left kidney was inconclusive (2 -3 glomerulus without any alterations, tubular atrophy and interstitial sclerosis, negative immunofluorescence). By the age of 13, after diet therapy had failed to lower triglycerides (564 mg/dL), she started therapy with fenofibrate 100 mg/day (half the contents of the 200 mg capsule), recommended by an endocrinologist.
When the patient was admitted by the Emergency Room, her treatment plan included sodium bicarbonate, calcium carbonate, calcitriol, folic acid, iron hydroxide, B complex, enalapril, levothyroxine and, for the last 9 months, fenofibrate approximately 100 mg/day.
About a month and a half before admission, the patient had been complaining of muscle weakness, myalgia and dark urine. Ten days prior to admission she presented symptoms compatible with a probable viral gastroenteritis with subsequent mild dehydration and worsening of the renal failure. In consequence she was transferred to the Nephrology Unit where initial examination revealed an ill-appearing girl. Cardiopulmonary evaluation was normal. Abdominal examination showed painful palpation of muscle masses, without organomegaly. Vital signs: blood pressure 126/82 mmHg (95th percentile for height and sex)6; pulse 66 bpm, respiratory rate 20/min. Anthropometric data: weight 43 kg, height 146 cm, body mass index 20.2 Kg/m2, body surface area 1.3 m2.
INVESTIGATION
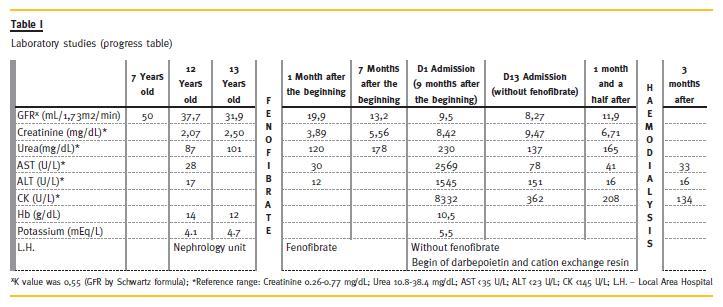
Four months prior to therapy with fenofibrate creatinine was 2.50 mg/dL (GFR of 31.9 mL/1.73 m2/min). It was found that after initiation of fenofibrate CRF progressed from stage 3 to stage 5 (Table 1).
Laboratory tests: haemoglobin 10.5 g/dL, urea 230 mg/dL creatinine 8.42 mg/dL, sodium 135 mEq/L, potassium 5.5 mEq/L, calcium 9.8 mg/dL, phosphorus 6.9 mg/dL, AST 2569 U/L, ALT 1545 U/L, CK 8332 U/L, protein 6.8 g/dL, albumin 3.8 g/dL, total cholesterol 148 mg/dL, triglycerides 203 mg/dL, LDL 96 mg/dL, HDL 34 mg/dL, free T4 0.57 ng/dL (rr 0.68-1.05), TSH 4.56 uUI/mL (rr < 3). Venous blood gas pH 7.37, bicarbonate 18 mmol/L, pCO2 32.2 mmHg. GFR 9.5 mL/1.73 m2/min, 3+ proteinuria and haematuria in urine dipstick that featured dark. Immunologic study (ANA and immunoglobulins) and infectious serology (A, B and C hepatitis, HIV, CMV, EBV negatives).
TREATMENT
On the first day of hospitalization, fenofibrate was suspended, CRF conservative therapy was optimized with begin of darbepoetin and cation exchange resin and the dose of levothyroxine was increased.
OUTCOME AND FOLLOW -UP
On the third day of hospitalization, the myalgia and fatigue was significantly reduced. There was a creatinine elevation to 9.47 mg/dL after 13 days of hospitalization (GFR minimum 8.27 mL/1.73m2/ min), which stabilized at 6.71 mg/dL (GFR 11.9 mL/1.73m2/min). We observed also a progressive normalization of muscle enzymes parameters about a month and a half after fenofibrate suspension.
After two months hospitalization, she started on haemodialysis. One year later, she underwent renal transplantation.
DISCUSSION
Rhabdomyolysis is characterized by cell extravasation of CK, LDH, aldolase, AST and potassium after myocyte necrosis. Typical clinical manifestations are muscle weakness, myalgia and dark urine due to myoglobinuria. The diagnosis is established by the elevated serum enzymes of the skeletal-muscle tissue and defined by the elevated serum CK ten times over the limit or normal1.
In the case described the clinical muscle weakness, myalgia, pain on palpation of muscle mass and dark coloured urine are compatible with rhabdomyolysis.
The elevation of serum CK fifty times above the upper limit defines the diagnosis.
In our case, in the absence of other precipitating factors of rhabdomyolysis, fenofibrate therapy appears to be the main cause of this occurrence. Clinical and laboratory improvement after its discontinuation are arguments in favour of this aetiology.
Although prior viral gastroenteritis could have contributed to the exacerbation of this incident, by potentially causing hydroeletrolitics changes, but it does not seem to be the main factor for this, as the clinical picture is prior to this acute illness.
Fenofibrate has a half-life of twenty hours and is mainly excreted by the kidneys. It is necessary to adjust the dose according to renal function, because its levels increase in renal failure. With a GFR < 15 mL/min fenofibrate is not recommended and with GFR 15 -59 mL/min, the recommended dose in adults is 67 mg/day7. In this case the GFR at beginning of treatment was 31.9 mL/1.73m2/min, consequently, the dose prescribed was higher than recommended, increasing the risk of rhabdomyolysis8. This was worsened by the fact that after seven months of therapy (two months before admission) GFR was 13.2 mL/1.73m2/min, which contraindicated the use of fenofibrate.
Acute renal failure is the most frequent complication of rhabdomyolysis, occurring in 10 -40% of patients9. There have been described cases of ARF by fenofibrate -induced rhabdomyolysis4,5,9,10. In the described case, the creatinine baseline value was 2.07 mg/dL and after a year of 2.50 mg/dL. With seven and nine months of treatment with fenofibrate, creatinine increased to 5.56 mg/dL and 8.42 mg/dL, respectively. After suspension of fenofibrate, the minimum value of creatinine was 6.71 mg/dL (Table 1). Treatment with fenofibrate appears to have been responsible for the deterioration of the renal function, which forced the initiation of renal replacement therapy (haemodialysis and renal transplantation).
In the presented case, the severity of fenofibrate muscle toxicity may be the result of the combination of several rhabdomyolysis enhancers factors: hypothyroidism, female gender and CRF, aided by drug doses higher than recommended to the GFR and not interrupted with the worsening of the CRF5.
In CRF, the elevation of triglycerides is common in teenagers, despite persistent severe hypertriglyceridemia (> 500 mg/dL) being rare. As to the safety and efficacy of fibrates in reducing triglyceride from paediatric age to adolescence, it has not been proven, and its use in this age group in patients with CRF is not recommended11-14. The recommendations for treatment of hypertriglyceridemia in chronic kidney disease (Clinical Practice Guidelines for Managing Dyslipidemias in Chronic Kidney Disease) summed up to the change in lifestyle and proper diet.
However, the use of fibrates in paediatrics is upheld as a treatment of familial dyslipidemias, and the paediatric use is licensed in some countries11,13,14.
This medication should be used wisely and under the supervision of a paediatric specialist. The risk of myopathy and rhabdomyolysis increases significantly when fibrates associate with statins or in patients with renal failure14.
In this case study, the use of fenofibrate appears to be associated with an irreversible deterioration of the renal function, with complete reversibility of rhabdomyolysis.
TAKE HOME MESSAGES
This case is of extreme importance to warn against the adverse events associated with fenofibrate therapy and to alert to the need of a rigorous control of its use when risk factors are present.
Rhabdomyolysis is a serious side-effect of therapy with fibrates. The use of fibrates implies detailed and clear therapeutic advantages versus potential accessories effects. Strict clinical and laboratory monitoring should be maintained, particularly in adolescents with CRF and hypothyroidism. Patients should be informed of possible iatrogenic potentially irreversible effects of fibrates.
References
1. Wu J, Song Y, Li H, Chen J. Rhabdomyolysis associated with fibrate therapy: review of 76 published cases and a new case report. Eur J Clin Pharmacol 2009; 65(12):1169 -1174 [ Links ]
2. Huerta -Alardin AL, Varon J, Marik PE. Bench -to -bedside review: Rhabdomyolysis – an overview for clinicians. Crit Care 2005; 9(2):158 -169 [ Links ]
3. Warren JD, Blumbergs PC, Thompson PD. Rhabdomyolysis: a review. Muscle Nerve 2002; 25(3):332 -347 [ Links ]
4. Melli G, Chaudhry V, Cornblath DR. Rhabdomyolysis: an evaluation of 475 hospitalized patients. Medicine (Baltimore) 2005; 84(6):377 -385 [ Links ]
5. Danis R, Akbulut S, Ozmen S, Arikan S. Rhabdomyolysis -induced acute renal failure following fenofibrate therapy: a case report and literature review. Case Rep Med 2010; doi: 10.1155/2010/537818. Epub 2010 Jul 25 [ Links ]
6. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004; 114(2 Suppl 4th Report):555–576 [ Links ]
7. Davidson MH, Armani A, McKenney JM, Jacobson TA. Safety considerations with fibrate therapy. Am J Cardiol 2007; 99(6A):3C -18C [ Links ]
8. Clouâtre Y, Leblanc M, Ouimet D, Pichette V. Fenofibrate -induced rhabdomyolysis in two dialysis patients with hypothyroidism. Nephrol Dial Transplant 1999; 14(4): 1047-1048 [ Links ]
9. Vanholder R, Sever MS, Erek E, Lameire N. Rhabdomyolysis. J Am Soc Nephrol 2000; 11(8):1553–1561 [ Links ]
10. Tahmaz M, Kumbasar B, Ergen K, Ure U, Karatemiz G, Kazancioglu R. Acute renal failure secondary to fenofibrate monotherapy -induced rhabdomyolysis. Ren Fail 2007; 29(7): 927 -930 [ Links ]
11. Chicaud P, Demange J, Drouin P, Debry G. Action of fenofibrate in hypercholesterolemic children: 18 -month follow-up. Presse Med 1984; 13(7):417 -419 [ Links ]
12. Kidney Disease Outcomes Quality Initiative (K/DOQI) Group. K/DOQI clinical practice guidelines for managing dyslipidemias in chronic kidney disease. Am J Kidney Dis 2003; 41(4 Suppl 3):s1 -91 [ Links ]
13. Haney EM, Huffman LH, Bougatsos C, Freeman M, Steiner RD, Nelson HD. Screening and treatment for lipid disorders in children and adolescents: systematic evidence review for the US Preventive Services Task Force. Pediatrics 2007; 120(1):189-214 [ Links ]
14. Daniels SR, Greer FR and the Committee on Nutrition. Lipid screening and cardiovascular health in childhood. Pediatrics 2008; 122 (1):198-208 [ Links ]
Dr.ª Filipa Carlota Marques
Departamento da Área de Pediatria Médica; Unidade de Nefrologia CHLC, EPE – Hospital de Dona Estefânia.
Rua Jacinta Marto, 1169 -045 Lisboa, Portugal
E-mail: filipacmarques@sapo.pt
Conflict of interest statement: None declared
Received for publication: 06/02/2014
Accepted in revised form: 21/07/2014


{kind=link}