










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versión impresa ISSN 0872-0169
Port J Nephrol Hypert vol.29 no.2 Lisboa jun. 2015
EDITORIAL
Haemodiafiltration: Present time technical, clinical, and financial issues
Bernard Canaud1,3, Laura Scatizzi2, Aileen Grassmann2, Daniele Marcelli2
1 Center of Excellence Medical, Fresenius Medical Care, Bad Homburg-Germany
2 Clinical and Epidemiological Research Management, Fresenius Medical Care, Bad Homburg-Germany
3 University of Montpellier, UFR Medicine, Montpellier-France
ABSTRACT
Online haemodiafiltration (HDF) is not a generic term that covers all convection-based renal replacement modalities – an optimal convection dose must be delivered to improve outcomes of end-stage kidney disease patients. In this brief article, we review current facts on HDF technical features, clinical/biological effects, and financial issues. In summary, HDF today offers highly efficient solute removal over the to-date widest known uraemic toxin molecular weight spectrum. Both safety and efficacy have been demonstrated in several short- and medium-term clinical studies. Recent randomized controled clinical trials and systematic reviews accredited the superiority of online HDF over standard haemodialysis (HD) when adequate convection dose is delivered. Additional clinical trials are needed to establish the optimal convection dose for different clinical settings (e.g. different patient characteristics and/or ethnicities, different substitution fluid delivery modalities) and to establish the cost-effectiveness of HDF compared to standard HD.
Key-Words: Chronic kidney disease; convective dose; end-stage kidney disease; patient outcomes; renal replacement therapy.
INTRODUCTION
In the early 1980s, the development of haemodiafiltration (HDF) was initially conceived as an attempt to cover unmet needs and shortfalls observed with the use of short conventional haemodialysis (HD) therapy. HDF was postulated to be beneficial both for the short-term, by improving efficacy (i.e. enhancing clearance of low and middle molecular weight uraemic toxins) and tolerability (i.e. increasing cardiovascular stability), and for the long-term, being putatively capable of reducing dialysis-related pathology (e.g. amyloidosis, ageing, accelerated atherosclerosis)1.
TECHNICAL AND SAFETY FEATURES
After the pioneering work of Leber et al. describing HDF using bags of substitution fluid2, it soon became clear from both a technical and economical viewpoint that on-line preparation of substitution fluid was the only viable method to implement HDF as a sustainable renal replacement therapy option in chronic kidney disease patients3,4.
Microbial safety of online HDF methods
Several clinical studies have confirmed the safety of the online HDF (ol-HDF) provided that appropriate CE marked and certified HDF machines are used and best clinical practices are applied5,6. The CONTRAST study confirmed the reliability and safety of the method in over 20,000 HDF sessions7.
In addition, using sensitive biomarkers of the acute-phase reaction (C-reactive protein, various interleukins), several prospective studies have shown reduced stimulation of these markers compare to HD8.
Flexibility of online HDF machines
The online HDF approach affords access to virtually unlimited volumes of substitution fluid as well as to various HDF options. This unique aspect facilitates not only achievement of an optimal targeted convection volume per patient (defined as the sum of the substitution volume and the volume removed for weight loss), but also allows one to select the most appropriate substitution fluid delivery modality (i.e. post-dilution, pre-dilution, mixeddilution) according to the patients individual profile9.
Accuracy and reliability of online HDF machines
Today, the technical features of HDF machines ensure delivery of an optimal convection-based treatment for all patients with incredible accuracy.
Irrespective of the convection volume targeted, fluid balance (including ultrafiltration required for weight loss) is achieved with a precision of ±100g with modern HDF machines. Ultrafiltration flow is optimized during HDF sessions by means of automated ultrafiltration control systems (e.g., AutoSub plus) ensuring a maximal tolerable filtration fraction and achievement of targeted convection volume10.
BIOLOGICAL AND CLINICAL EFFECTS
Enhanced solute removal and clinical benefits of HDF
Several controlled studies have confirmed enhanced clearance and mass removal of β2-microglobulin with HDF (30 to 40% higher than high-flux HD) accompanied by a 10 to 20% decline in circulating blood β2-microglobulin concentrations11,12. Phosphate mass removal could be enhanced by 15 to 20%13 and pre-dialysis serum phosphate levels were reduced by 6% while the percentage of patients reaching target pre-treatment serum phosphorus levels increased from 64 to 74% in the CONTRAST study14. Higher clearances of a number of other uraemic compounds have also been documented with HDF, including complement factor D (a pro-inflammatory mediator), leptin (16 kDa, involved in loss of appetite), FGF23 (30kDa, implicated in metabolic bone disorders and vascular calcification) and various cytokines, and circulating advanced glycosylation end products (AGEs) and AGE precursors15,16. ESA dose could be reduced in several clinical studies, the benefit being attributed to the combined effects of the higher solute removal of middle-sized toxins (erythropoietic inhibitor substances) and the use of higher quality water and dialysis fluid (reducing inflammation)17. This effect was not confirmed in a recent meta-analysis18. Several large cohort studies indicate that the extended use of high-flux membranes and convective therapies have a beneficial impact on the development of β2-microglobulin amyloidosis, reducing the incidence of carpal tunnel syndrome. This beneficial effect probably results from the regular use of ultrapure water and biocompatible materials, preventing inflammation, combined with convective modalities that enhance β2-microglobulin removal19.
Better dialysis session tolerance
A significant reduction in episodes of intradialytic hypotension was observed in HDF compared to conventional HD20. This has been ascribed to negative thermal balance (due to infusion of relatively cool replacement fluid), a high sodium concentration of the substitution fluid, and/or removal of vasodilating mediators21.
Patient outcome
The ultimate benefits of HDF therapy for ESKD patients are survival improvement and hospitalization reduction. Several retrospective cohort studies that suggested that HDF had beneficial effects on patient outcomes have been confirmed by recent prospective randomized controlled trials22,23. The Dialysis Outcomes and Practice Patterns Study (DOPPS) first suggested that patients being treated with highefficiency HDF (substitution volume of 15 – 25 L/session) had a 35% lower mortality than those treated with low-flux HD; however, comparison with high-flux HD and low-efficiency HDF (<15 L/session), did not yield statistically significant results24.
Two recent prospective randomized trials (CONTRAST and Turkish HDF studies) failed to show beneficial effects on mortality (all-cause or cardiovascular mortality) as primary endpoint. Interestingly, both studies showed beneficial effects in post-hoc analyses restricted to patients with high convection volumes (> 20 L/session)25,26. The fact that 50 to 66% of patients enrolled did not achieve the targeted convection volume underlines the importance of best clinical practices and some weakness of these studies27.
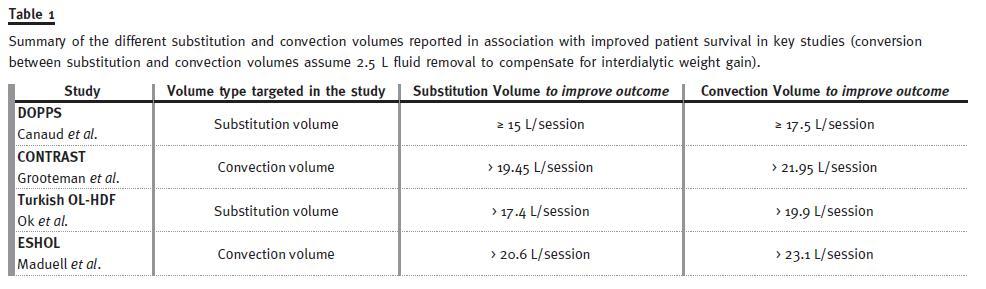
The most recent randomized controlled trial, the Catalonian ESHOL study, complying with best clinical practices and achieving targeted convection volume in 90% of patients, proved that mortality was reduced by 30% (all-cause and cardiovascular cause) in patients treated with high-volume HDF. In addition, this study found a reduction in hypotensive episodes (28%), stroke (61%) and infection (55%) for the high-volume HDF patients compared to the HD patients28. The remaining question today concerns the magnitude of the effective convection volume that should, optimally, be delivered, i.e., the sum of the substitution volume and the volume ultrafiltered to compensate for weight gain29,30. The CONTRAST study was the first RCT study that aimed to answer this question. It was designed to target delivery of 24L of convection volume per treatment, but only achieved an average of 20.7 L27,31. Post hoc analysis showed that survival was significantly higher in the tertile of patients treated with the highest convection volume, >21.95 L25. A similar study was conducted in parallel in Turkey. Here online HDF was compared with high-flux HD, a substitution volume of at least 15 L was targeted, and a median substitution volume of 17.4 L was achieved26. The result was similar to CONTRAST in that no difference in survival could be shown for the global population, but again a post hoc analysis of HDF patients treated with convection volumes of > 19.9 L (17.4 L substitution volume ±2.5 L weight loss), revealed significantly improved survival for this subgroup. The secondary result from these two large, randomized, controlled studies was confirmed by the ESHOL study, which in its primary analysis showed that all patients treated with HDF with convection volumes exceeding 23.1 L per session had significantly improved survival compared to patients treated with high-flux HD28. A summary of the different substitution and convection volumes reported in association with improved patient survival in the different studies mentioned above is presented in Table 1.
Several meta-analyses and/or systematic reviews addressing benefits of HDF compared to standard HD have reported conflicting results18,32. Unfortunately, these meta-analyses aggregated several different convection-based methods under the umbrella of convective therapies (i.e. haemofiltration, acetate-free biofiltration, low volume haemodiafiltration).
Failure to account for the effective convection volume achieved presents a major shortcoming in their findings. The EUDIAL group, an official ERA-EDTA working group, clearly identified improved outcomes in patients receiving adequately dosed haemodiafiltration33.
The remaining and burning question for the nephrology community is now to identify the threshold and/or optimal convection dose for improving outcomes of ESKD patients.
Online haemodiafiltration can no longer be considered an experimental treatment, but has matured to a renal replacement therapy that is used daily to sustain life in more than 70,000 ESKD patients in Europe34.
FINANCIAL ISSUES
Cost of HDF treatment relies on the cost of the three main components: 1. The online HDF machine and technical features; 2. Disposable tubing sets and ultrafilters for substitution fluid sterility; 3. Microbiological monitoring of water and substitution/dialysis fluid quality. If one accepts that HDF is an optional technical feature of most available HD machines in Europe, and ultrapure water and dialysis fluid are anyway required for high-flux HD (backtransport of dialysis fluid), then the extra cost of HDF is only bound to the cost of the disposable tubing set (blood and substitution lines) and is not significantly different from high-flux HD35. A recent comparison of the costs of different HDF machines in a non-profit French organization revealed that the extra cost per treatment is between +0.17 and +0.23 Euros, but varies between -1.29 and +4.58 Euros, according to the type of HDF machines. This difference was mainly due to the disposable tubing set including (or not) a final sterilizing ultrafilter in the substitution line36.
Reimbursement policy differs from country to country and sometimes even within countries, from region to region. In the majority of European countries, HDF is reimbursed at the same tariff as high-flux HD, meaning that no extra reimbursement is provided for this method. Cost-saving effects of HDF have not yet been extensively analysed; nevertheless, one can postulate some savings due to an improvement in the inflammation profile, less ESA consumption, and a reduction in the use of phosphate binders. A recent sub-analysis of the CONTRAST study focusing on cost-utility of HDF (QALY) did not show favourable results compared to regular HD, but also suffered the shortcoming of not taking the role of convection volume into consideration37.
CONCLUSION
Online HDF offers efficient solute removal over a wide spectrum of uraemic toxin molecular weights.
Both safety and efficacy have been proven in several short-and medium-term clinical studies. Recent randomized controled clinical trials tend to support the superiority of online HDF compare to standard HD when a high convection dose (or convection volume) is delivered.
Further clinical trials are needed to establish the optimal convection dose in different clinical settings (e.g. patient characteristics and/or ethnicities, substitution modalities) and to establish the cost-effectiveness of HDF compared to standard HD.
References
1. Blagg CR. Long-term Complications in Hemodialysis. Saudi J Kidney Dis Transpl. 2001;12(4):487-493. [ Links ]
2. Leber HW, Wizemann V, Goubeaud G, Rawer P, Schutterle G. Hemodiafiltration: a new alternative to hemofiltration and conventional hemodialysis. Artif Organs. 1978;2(2):150-153. [ Links ]
3. Henderson LW, Beans E. Successful production of sterile pyrogen-free electrolyte solution by ultrafiltration. Kidney Int. 1978;14(5):522-525. [ Links ]
4. Canaud B, NGuyen QV, Lagarde C, Stec F, Polaschegg HD, Mion C. Clinical evaluation of a multipurpose dialysis system adequate for hemodialysis or for postdilution hemofiltration/hemodiafiltration with on-line preparation of substitution fluid from dialysate. Contrib Nephrol. 1985;46:184-186. [ Links ]
5. Di Felice A, Cappelli G, Facchini F, et al. Ultrafiltration and endotoxin removal from dialysis fluids. Kidney Int Suppl. 1993;41:S201-204. [ Links ]
6. Vaslaki L, Karatson A, Voros P, et al. Can sterile and pyrogen-free on-line substitution fluid be routinely delivered? A multicentric study on the microbiological safety of online haemodiafiltration. Nephrol Dial Transplant. 2000;15 Suppl 1:74-78. [ Links ]
7. Penne EL, Visser L, van den Dorpel MA, et al. Microbiological quality and quality control of purified water and ultrapure dialysis fluids for online hemodiafiltration in routine clinical practice. Kidney Int. 2009;76(6):665-672. [ Links ]
8. Susantitaphong P, Riella C, Jaber BL. Effect of ultrapure dialysate on markers of inflammation, oxidative stress, nutrition and anemia parameters: a meta-analysis. Nephrol Dial Transplant. 2013;28(2):438-446. [ Links ]
9. Canaud B, Chenine L, Henriet D, Leray H. Online hemodiafiltration: a multipurpose therapy for improving quality of renal replacement therapy. Contrib Nephrol. 2008;161:191-198. [ Links ]
10. Marcelli D, Scholz C, Ponce P, et al. High-volume postdilution hemodiafiltration is a feasible option in routine clinical practice. Artif Organs. 2015;39(2):142-149. [ Links ]
11. Ward RA, Schmidt B, Hullin J, Hillebrand GF, Samtleben W. A comparison of on-line hemodiafiltration and high-flux hemodialysis: a prospective clinical study. J Am Soc Nephrol. 2000;11(12):2344-2350. [ Links ]
12. Pedrini LA, Gmerek A, Wagner J. Efficiency of post-dilution hemodiafiltration with a high-flux alpha-polysulfone dialyzer. Int J Artif Organs. 2011;34(5):397-404. [ Links ]
13. Lornoy W, De Meester J, Becaus I, Billiouw JM, Van Malderen PA, Van Pottelberge M. Impact of convective flow on phosphorus removal in maintenance hemodialysis patients. J Ren Nutr. 2006;16(1):47-53. [ Links ]
14. Penne EL, van der Weerd NC, van den Dorpel MA, et al. Short-term effects of online hemodiafiltration on phosphate control: a result from the randomized controlled Convective Transport Study (CONTRAST). Am J Kidney Dis. 2010;55(1):77-87. [ Links ]
15. Lin CL, Huang CC, Yu CC, Yang HY, Chuang FR, Yang CW. Reduction of advanced glycation end product levels by on-line hemodiafiltration in long-term hemodialysis patients. Am J Kidney Dis. 2003;42(3):524-531. [ Links ]
16. Stein G, Franke S, Mahiout A, et al. Influence of dialysis modalities on serum AGE levels in end-stage renal disease patients. Nephrol Dial Transplant. 2001;16(5):999-1008. [ Links ]
17. Panichi V, Scatena A, Rosati A, et al. High-volume online haemodiafiltration improves erythropoiesis-stimulating agent (ESA) resistance in comparison with low-flux bicarbonate dialysis: results of the REDERT study. Nephrol Dial Transplant. 2015;30(4):682-689. [ Links ]
18. Susantitaphong P, Siribamrungwong M, Jaber BL. Convective therapies versus low-flux hemodialysis for chronic kidney failure: a meta-analysis of randomized controlled trials. Nephrol Dial Transplant. 2013;28(11):2859-2874. [ Links ]
19. Schiffl H. Impact of advanced dialysis technology on the prevalence of dialysis-related amyloidosis in long-term maintenance dialysis patients. Hemodialysis international International Symposium on Home Hemodialysis. 2014;18(1):136-141. [ Links ]
20. Locatelli F, Altieri P, Andrulli S, et al. Hemofiltration and hemodiafiltration reduce intradialytic hypotension in ESRD. J Am Soc Nephrol. 2010;21(10):1798-1807. [ Links ]
21. van der Sande FM, Kooman JP, Konings CJ, Leunissen KM. Thermal effects and blood pressure response during postdilution hemodiafiltration and hemodialysis: the effect of amount of replacement fluid and dialysate temperature. J Am Soc Nephrol. 2001;12(9):1916-1920. [ Links ]
22. Panichi V, Rizza GM, Paoletti S, et al. with the RESCAVID Study Group. Chronic inflammation and mortality in haemodialysis: effect of different renal replacement therapies. Results from the RISCAVID study. Nephrol Dial Transplant. 2008;23(7):2337-2343. [ Links ]
23. Vilar E, Fry AC, Wellsted D, Tattersall JE, Greenwood RN, Farrington K. Long-term outcomes in online hemodiafiltration and high-flux hemodialysis: a comparative analysis. Clin J Am Soc Nephrol. 2009;4(12):1944-1953. [ Links ]
24. Canaud B, Bragg-Gresham JL, Marshall MR, et al. Mortality risk for patients receiving hemodiafiltration versus hemodialysis: European results from the DOPPS. Kidney Int. 2006;69(11):2087-2093. [ Links ]
25. Grooteman MP, van den Dorpel MA, Bots ML, et al. with the CONTRAST Investigators. Effect of online hemodiafiltration on all-cause mortality and cardiovascular outcomes. J Am Soc Nephrol. 2012;23(6):1087-1096. [ Links ]
26. Ok E, Asci G, Toz H, et al. with the Turkish Online Haemodifailtration Study. Mortality and cardiovascular events in online haemodiafiltration (OL-HDF) compared with high-flux dialysis: results from the Turkish OL-HDF Study. Nephrol Dial Transplant. 2013;28(1):192-202. [ Links ]
27. Penne EL, van der Weerd NC, Bots ML, et al. with the CONTRAST Investigators. Patientand treatment-related determinants of convective volume in post-dilution haemodiafiltration in clinical practice. Nephrol Dial Transplant. 2009;24(11):3493-3499. [ Links ]
28. Maduell F, Moreso F, Pons M, et al. with the ESHOL Study Group. High-efficiency postdilution online hemodiafiltration reduces all-cause mortality in hemodialysis patients. J Am Soc Nephrol. 2013;24(3):487-497. [ Links ]
29. Tattersall JE, Ward RA; EUDIAL group. Online haemodiafiltration: definition, dose quantification and safety revisited. Nephrol Dial Transplant. 2013;28(3):542-550. [ Links ]
30. Bowry SK, Canaud B. Achieving high convective volumes in on-line hemodiafiltration. Blood Purif. 2013;35 Suppl 1:23-28. [ Links ]
31. Penne EL, Blankestijn PJ, Bots ML, et al. with the CONTRAST Study Group. Effect of increased convective clearance by on-line hemodiafiltration on all cause and cardiovascular mortality in chronic hemodialysis patients – the Dutch CONvective TRAnsport STudy (CONTRAST): rationale and design of a randomised controlled trial [ISRCTN38365125]. Curr Control Trials Cardiovasc Med. 2005;6(1):8. [ Links ]
32. Nistor I, Palmer SC, Craig JC, et al. Convective versus diffusive dialysis therapies for chronic kidney failure: an updated systematic review of randomized controlled trials. Am J Kidney Dis. 2014;63(6):954-967. [ Links ]
33. Mostovaya IM, Blankestijn PJ, Bots ML, et al. with EUDIAL1 – an official ERA-EDTA Working Group. Clinical evidence on hemodiafiltration: a systematic review and a meta-analysis. Seminars in dialysis. 2014;27(2):119-127. [ Links ]
34. Sichart JM, Moeller S. Utilization of hemodiafiltration as treatment modality in renal replacement therapy for end-stage renal disease patients–a global perspective. Contrib Nephrol. 2011;175:163-169. [ Links ]
35. Oates T, Cross J, Davenport A. Cost comparison of online haemodiafiltration with high-flux haemodialysis. Journal of nephrology. 2012;25(2):192-197. [ Links ]
36. Lebourg L, Amato S, Toledano D, Petitclerc T, Creput C. [Online hemodiafiltration: is it really more expensive?]. Nephrol Ther. 2013;9(4):209-214. [ Links ]
37. Mazairac AH, Blankestijn PJ, Grooteman MP, et al. with the CONTRAST Investigators. The cost-utility of haemodiafiltration versus haemodialysis in the Convective Transport Study. Nephrol Dial Transplant. 2013;28(7):1865-1873. [ Links ]
Prof Bernard Canaud
CMO – Center of Excellence Medical
Fresenius Medical Care Deutschland GmbH
Else Kröner Strasse, 1
61352 Bad Homburg, Germany
Phone +49 6172 609 405
E-mail: bernard.canaud@fmc-ag.com
Conflict of interest statement: No external funding was received. All authors are employees of Fresenius Medical Care and may hold stock in the company.
Received for publication: 08/04/2015
Accepted: 11/04/2015


{kind=link}