










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versión impresa ISSN 0872-0169
Port J Nephrol Hypert vol.29 no.4 Lisboa dic. 2015
REVIEW ARTICLE
Treatment of hepatitis C in patients with chronic kidney disease: a challenge
O tratamento da hepatite C na doença renal crónica: um desafio
Alice Santana, Natacha Rodrigues
Department of Nephrology and Kidney Transplantation, Hospital de Santa Maria, Centro Hospitalar Lisboa Norte EPE,Lisboa, Portugal
ABSTRACT
The prevalence of hepatitis C virus infection is several times higher in the sub-population of patients with chronic end -stage renal disease on dialysis, or transplanted.
Therapy with Interferon and Ribavirin was for many years the gold standard treatment of hepatitis C. However, this therapy has many adverse effects and low effectiveness. The emergence of new drugs with direct antiviral action, has revolutionized the treatment of hepatitis C. Cure rates greater than 90% associated with easy and convenient oral administration and good safety profile, contributed to the large patient adherence to these therapies. Treatment options with Interferon-free and Interferon-Ribavirin-free regimens are now available.
In chronic renal failure or dialysis patients, therapy with Interferon and Ribavirin is even worse tolerated.
Initial studies with new drugs with direct antiviral action did not include patients with severe renal failure, and its use in these patients must be done carefully, since some drugs require dose adjusted to renal function. Preliminary results of ongoing studies are promising: Simeprevir, Ledipasvir and the combination Ritonavir-Paritaprevir-Ombitasvir-Dasabuvir seem to be safe and efficient in severe renal failure. Sofosbuvir is not indicated for patients with creatinine clearance < 30 ml/min/1.73m2 or on regular haemodialysis since no dose recommendation is defined.
In kidney transplant patients, therapy with Interferon and Ribavirin is even more disappointing. The success rate is much lower than in the general population, and the toxicity is very high. Acute rejection and graft dysfunction rates greater than 20% are described even in the most recent series. There is a consensus that for these patients the ideal therapy should not include Interferon. However, until now there is no experience with the use of new drugs with direct antiviral action in kidney transplantation. Current recommendations suggest that the choice of therapy in these patients have regard to the function of the transplanted kidney and pharmacological interaction of new drugs with immunosuppressive therapy.
Studies are needed to best define the most effective therapeutic and the optimal doses of these new drugs in the sub -population of patients with chronic renal disease.
Key -Words: Chronic kidney disease; direct antiviral action drugs; hepatitis C infection.
RESUMO
A prevalência da infeção pelo vírus da hepatite C é maior nos doentes com insuficiência renal crónica em diálise ou transplantados do que na população geral.
A terapêutica com Interferão e Ribavirina que foi durante muitos anos o «gold standard» do tratamento da hepatite C, apresenta baix a eficácia, e elevada toxicidade. O aparecimento recente de novos fármacos, com ação antiviral direta, veio revolucionar o tratamento ao proporcionar taxas de cura superiores a 90%.
A fácil e cómoda administração por via oral e a baixa incidência de efeitos secundários, contribuíram para a grande adesão dos doentes a estas terapêuticas. Regimes sem Interferão e em alguns casos sem Interferão nem Ribavirina são agora possíveis.
Nos doentes com insuficiência renal crónica em diálise a terapêutica com Interferão e Ribavirina é ainda pior tolerada do que na população geral. Os estudos iniciais com os novos fármacos com ação antiviral direta não incluíram doentes com insuficiência renal avançada. No entanto resultados preliminares de estudos em curso são promissores: o Simeprevir, o Ledipasvir e a combinação de Ritonavir-Paritaprevir-Ombitasvir-Dasabuvir parecem ser eficazes e seguros nos doentes com insuficiência renal avançada. O Sofosbuvir não está indicado nos doentes com clearence de creatinina < 30ml/min/1.73m2 ou em hemodiálise, uma vez que não está ainda definida a dose a administrar.
Nos doentes transplantados renais, a terapêutica com Interferão e Ribavirina é ainda mais dececionante.
A taxa de sucesso é muito inferior à da população geral, e a toxicidade é muito elevada. Taxas de rejeição aguda e disfunção do rim transplantado superiores a 20% são descritas com a utilização do Interferão, mesmo nas séries mais recentes. Não existe ainda experiência com a utilização dos novos fármacos com ação antiviral direta nesta subpopulação. As recomendações atuais sugerem que a escolha da terapêutica nestes doentes tenha em consideração a função do rim transplantado e a interação farmacológica dos novos fármacos com a terapêutica imunossupressora.
São necessários estudos para definir a terapêutica mais eficaz e as doses ideais dos novos fármacos na subpopulação de doentes com insuficiência renal crónica.
Palavras -Chave: Doença renal crónica; fármacos com ação antiviral direta; hepatite C.
INTRODUCTION
Infection by hepatitis C virus (HCV) is one of the most frequent causes of chronic liver disease worldwide.
The long-term impact of HCV infection is highly variable, ranging from minimal histological changes to extensive fibrosis and cirrhosis with or without hepatocellular carcinoma. In the United States, HCV infection is the leading cause of death from liver disease and the main cause for liver transplantation1,2.
It is estimated that about 2.8% of the world population has positivity for HCV antibody, which translates from around 160 to 170 million people infected. The prevalence varies depending on the part of the world, reaching more than 3.5% in less developed areas, in contrast with more developed countries where the prevalence is less than 1.5%3.
A recent review of published studies shows that the prevalence of HCV infection has increased in recent years, thus being considered a serious public health problem. Moreover, many cases are undiagnosed, delaying the institution of therapy and favouring transmission of the infection3.
The prevalence of HCV infection in patients with end stage renal disease (ESRD) is higher than in the general population, and also varies among geographical areas. In developed countries, the prevalence and incidence of HCV in patients with ESRD has been declining in the last decades. In the United States, the prevalence of anti -HCV positivity has dropped from 10.4% in 1985 to 7.8%, in 2002, but is still 5 times greater than in the general population4. Similarly, the European multicentre survey reported a decreasing prevalence of anti-HCV positivity in the majority of European countries5. A recent meta-analysis carried out by Su et al. on the incidence of HCV infection in haemodialysis patients, confirms the variability in the number of new cases of hepatitis C in several geographical areas6. The authors reviewed 22 published studies and found an incidence of 0.97 (95% CI: 0.66 -1.29) per 100 patients in developed countries and 4.44 (95% CI: 2.65 -6.23) per 100 patients in the developing world. In the dialysis units where the prevalence of HCV infection was greater, the number of new cases also tended to be higher6.
Haemodialysis patients are particularly vulnerable to HCV transmission from infected sources in their dialysis units. Knowledge about the HCV transmission process was crucial to the implementation of measures to control and prevent the infection in dialysis centres. The Kidney Disease Improving Global Outcomes (KDIGO) practice guidelines for the prevention of hepatitis C in chronic kidney disease do not recommend dedicated machines or patient isolation for anti-HCV positive patients in haemodialysis7. However, Portuguese guidelines recommend the use of dedicated machines in anti-HCV positive patients. It is also recommended by Portuguese law that the units implement a preventive strategy by concentrating patients with HCV in the same room in a defined area, with some kind of physical separation of the remaining patients8.
Screening for HCV infection must be based on the detection of anti -HCV antibodies and if antibodies are detected, HCV -RNA should be determined by a sensitive molecular method2,7,8. The adoption of surveillance measures with serial monitoring of anti-HCV antibody in patients on dialysis is also important in the early identification of seroconversion. Patients on haemodialysis should be tested for anti -HCV antibody when they start haemodialysis, when they transfer from another haemodialysis facility or when unexplained abnormal aminotransferases are present.
For patients who test negative for HCV, the current United States guidelines and KDIGO suggest retesting every 6 months, but Portuguese guidelines recommend retesting every 3 months. For the units with a prevalence of HCV carriers greater than 20% the recommended retesting is monthly7,8.
CHARACTERISTICS OF HCV INFECTION IN HAEMODIALYSIS PATIENTS
In haemodialysis patients, acute infection is usually asymptomatic and anicteric, so it can be difficult to diagnose early. The elevation of transaminases in particular alanine aminotransferse (ALT) is lower than in patients without renal failure. This is possibly due to suppression of ALT synthesis in hepatocytes, defective release into the blood stream, or accelerated clearance9. Despite the lower levels of ALT, acute infections are often accompanied by moderate increases. Anti -HCV seroconversion follows ALT elevation, one to seven months after, in 90% of cases10.
Unexplained increase in serum ALT in haemodialysis patients should raise the suspicion of acute HCV infection and the infection must be confirmed by the detection of HCV-RNA in serum by polymerase chain reaction (PCR) assay, which precedes the appearance of anti-HCV antibodies by weeks or months.
A third generation anti-HCV assay by enzyme immunoassay technique is the most commonly used screening tool, providing excellent accuracy, with a 0.26% false-negative rate. Then a PCR -based molecular diagnosis is required to confirm viraemia, quantify viral load and diagnose viral genotype. Low HCV viral loads are typically observed in haemodialysis patients and HCV-RNA level is transiently decreased during haemodialysis session and gradually returns to baseline level within 48 hours. Explanations for this may be filtration of viral particles into the dialysate, adherence of the virus to the surface of the dialysis membrane, destruction of viral particles during the dialysis procedure by the hydraulic pressure, or interference with PCR technique by heparin used during haemodialysis. It is recommended to determine HCV -RNA level before the haemodialysis session to avoid underestimation11. Moreover, intermittent HCV viraemia with low levels of serum HCV-RNA interpolated with episodes of undetectable HCV –RNA are common in haemodialysis patients. False negative results in HCV -RNA assays are reported in 33% to 67% of anti-HCV reactive haemodialysis patients.
Therefore, isolated undetectable results of HCV–RNA should not be interpreted as absence of replication.
A sequential HCV-RNA monitoring is useful for all anti-HCV patients on haemodialysis.
Spontaneous viral clearance is very uncommon in haemodialysis patients, occurring in less than 5%, so most of the patients get to a chronic stage12. In haemodialysis patients with chronic HCV hepatitis there is a weak correlation between ALT levels and liver disease, even in the presence of significant histological damage, which hampers the utility of ALT as a marker of hepatic lesion in this population. However, the prevalence of advanced liver fibrosis is lower than in the general population and the progression to cirrhosis during haemodialysis is uncommon13.
CHARACTERISTICS OF HCV INFECTION IN KIDNEY TRANSPLANT PATIENTS
The HCV -infected renal transplant recipients have worse patient and allograft survival when compared with non-infected patients14-16. In contrast to what is observed in chronic kidney disease patients under haemodialysis, HCV-positive kidney transplanted patients have higher prevalence of advanced liver disease, such as cirrhosis, fibrosing cholestatic hepatitis or liver failure15. However, the increased mortality in the post-transplant period in this population has been associated not only with the progression of liver disease but also with extra -hepatic complications of HCV infection, including renal disease and diabetes mellitus.
HCV infection may be more commonly associated with glomerular disease in renal transplants than in native kidneys. Both recurrent and de novo glomerular diseases can occur. One possible mechanism is that immunosuppressive therapy increases the title of HCV-RNA14. The higher number of HCV particles may lead to an alteration in the ratio of antibody to antigen in immune complexes, resulting in decreased clearance and increased deposition of viral complexes in the kidney. Membranoproliferative glomerulonephritis with or without mixed cryoglobulinemia, membranous nephropathy and renal thrombotic microangiopathy are the more frequent kidney lesions16.
TREATMENT
The history of HCV discovery and anti-viral–drug development is a striking example of the effect of advances in biomedical research on disease outcome.
The virus discovery had relied on direct visualization of viral particles and the subsequent molecular characterization of the viral genome. The development of new therapeutic strategies was only possible due to the ultra-structural characterization of non-structural proteins involved in viral replication.
The HCV is a positive-stranded RNA virus that replicates its genome directly into RNA without traversing a DNA intermediate, so that unlike HIV or hepatitis B virus, it lacks a latent, nuclear form that defies ready immunologic clearance. Instead, it requires continuous replication for its existence.
Knowledge of this fact was important for the design of strategies to permanently clear the virus1. In addition molecular characterization of viral genotypes led to the development of genotype-specific therapeutic regimens2. Knowledge of the proteins involved in virus replication was essential to the development of direct-acting antiviral agents (DAAs) that have revolutionized HCV treatment. These include inhibitors of NS3/4A prote ase, NS5A and both nucleoside and nonnucleoside NS5B polymerase inhibitors. A combination of potent agents from two or more classes with non-overlapping resistance profiles could provide rapid and potent suppression of viral replication and prevent the emergence of resistant variants.
This regimen could achieve high cure rates greater than 90% for all viral genotypes, and freedom from dependence on interferon.
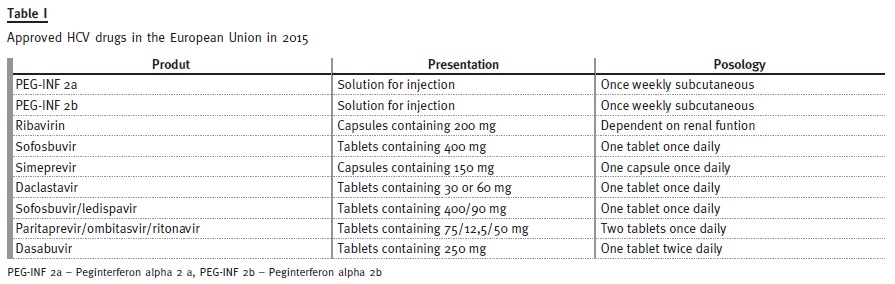
Table 1 shows the drugs approved in the European Union for the treatment of hepatitis C in 2015.
Sustained virological response (SVR) rate to determine the HCV cure is defined as undetectable HCV-RNA, 12 weeks after the end of treatment.
1 – Interferon
Interferon -alpha (INF) is a glycoprotein, produced by immune cells in response to foreign antigens, such as virus, bacteria or tumour cells. The elimination half-life of INF following subcutaneous injection is 2-4h. Due to a short half -life, sustained plasma levels are not maintained, which is believed in part to explain the suboptimal response rates, when used in the treatment of hepatitis C17. Elimination is brought about by filtration through the glomeruli and during proximal tubular reabsorption it undergoes lysosomal proteolytic degradation. The kidney is the main site of degradation of INF molecule and accumulation of INF occurs in patients with renal dysfunction17. Compared with non-uraemic patients, patients on haemodialysis demonstrate one-half the clearance, significantly longer half -lives, and markedly larger areas under the concentration curve. This may contribute to the high rate of serious adverse events reported with daily administration of INF among haemodialysis patients.
A «flu-like» syndrome with asthenia, myalgia and headache, haematologic toxicity and neuropsychiatric symptoms are the most common INF side effects18.
Combining a polyethylene glycol (PEG) polymer to INF successfully created a molecule with a longer half-life, improved pharmacokinetic profile, and allowed administration once weekly. PEG -INF alpha-2a, a branched -PEG attached to INF, is metabolized in the liver and kidneys and has a long elimination half-life of approximately 77h. PEG -INF alpha-2b, a linear PEG molecule attached to INF, is metabolized exclusively by the kidneys and has a half–life of approximately 40h19. The pharmacokinetic of PEG-INF alpha-2a is less affected by renal failure, and less dose modifications are necessary in the setting of renal impairment when compared to PEG -INF alpha -2b, so it is a best choice in these patients. Haemodialysis has only a small effect on INF and PEG -INF clearance.
2 – Ribavirin (RBV)
After oral intake, RBV is rapidly absorbed and distributed with a bioavailability of approximately 50%. Elimination is predominately via the kidney and very little RBV is removed by haemodialysis20.
The optimal dosing strategy of RBV must be calculated according to the renal function. The area under the curve (AUC) for RBV is increased by 2 folds in patients with creatinine clearance (CrCl) 30 -60 ml/min per 1.73m2 and by 3 folds in patients with CrCl 10 -30 ml/min per 1.73m2, when compared to those with CrCl> 90 ml/min per 1.73m2 21. The use of RBV in moderate to severe renal insufficiency is controversial.
The KDIGO clinical practice guidelines contraindicate its use when CrCl is less than 50 ml/min per 1.73m2 7. However, some authors defend its use with low doses and closer monitoring in patients with moderate to severe renal i mpairment and in haemodialysis patients.
The main adverse effect of RBV is haemolytic anaemia. RBV is actively transported into circulating red blood cells (RBC) and causes a relative triphosphate deficiency and increased susceptibility to oxidative damage, leading to accelerated RBC turnover and haemolytic anaemia. The RBV plasma concentrations predict RBV -induced anaemia, therefore in patients with chronic kidney disease, renal function and haemoglobin levels should be carefully monitored.
The use of erythropoiesis-stimulating agents may be helpful22,23.
3 – Direct acting antiviral agents (DAAS) Boceprevir and Telaprevir
These first generation protease NS3/4A inhibitors are used in triple therapy in combination with PEG-INF and RBV. This strategy has succeeded in boosting rates of SVR from about 50% to approximately 75% among patients with genotype 1 infection. However its effectiveness was limited by the side effect profile, with cytopenias, depression, rash and autoimmune disorders.
In vitro studies indicate that Boceprevir undergoes metabolism through the aldo -keto redutase-mediated pathway and, to a lesser extent, oxidative metabolism mediated by CYA3A4 in the liver. Telaprevir is metabolized in the liver involving hydrolysis, oxidation, and reduction. No dose adjustment is required for both in patients with any degree of renal impairment, and they are not removed by dialysis24.
Preliminary experience with its use has been reported in a small number of patients with renal impairment.
Dumortier et al. reports 4 cases of HCV infected haemodialysed patients, who had not responded to a prior course of PEG -IFN and RBV and who received a second-line antiviral treatment with PEG -IFN, RBV and Telaprevir. After 12 weeks of triple therapy, HCV–RNA became undetectable in 3/4 patients, and they concluded that triple therapy with a first generation protease inhibitor could be the new standard for the treatment of HCV patients with ESRD25.
Simeprevir
Simeprevir is a second generation protease inhibitor. In phase 3 studies, Simeprevir was given in combination with PEG -INF and RBV to naive patients (QUEST 1 and 2), and to patients who had relapsed or who did not respond to prior therapy with PEG-INF and RBV, (PROMISE and ASPIRE respectively).
The effectiveness of this combined therapy was compared with a placebo. The triple therapy with PEG -INF/RIB/Simeprevir achieved a SVR of about 80% in naïve and in patients who relapsed after prior IFN-RBV-based therapy, a much higher rate than double therapy with PEG-INF/RBV/placebo. The safety profile was very favourable with discontinuation of Simeprevir due to adverse reactions occurring in only 0.9% of patients26-28.
Simeprevir is primarily metabolized by the CYP3A4 in the liver, and renal elimination is negligible. A pharmacokinetic study in volunteers demonstrated that Simeprevir exposure after 7 days of 150mg/day dosing was 62% higher in patients with severe renal impairment compared with matched healthy volunteers, but safety and tolerance were considered favourable. It was concluded that no dose adjustment is required in patients with mild or moderate renal impairment, but Simeprevir has not been studied in HCV infected patients with severe renal impairment (CrCl below 30ml/min per 1.73m2) or ESRD, including patients requiring haemodialysis29.
The safety and efficacy of Simeprevir have not been studied in organ transplant patients. Co-administration with substances that moderately or strongly induce or inhibit cytochrome P450 3A (CYP3A4) is not recommended as this may lead to significantly lower or higher exposure of Simeprevir, respectively.
Increased Simeprevir concentrations may occur when it is co-administered with immunosuppressive drugs such as Cyclosporine and Tacrolimus, but no dose adjustment is recommended for immunosuppressive drugs. Closer monitoring Cyclosporine and Tacrolimus trough levels are required29.
The European Association for the Study of the Liver (EASL) recommendations on the treatment of hepatitis C suggests that Simeprevir is effective in the treatment of HCV genotype 1 and 4 in INF -regimens with RBV (INF/RBV/Simeprevir) or in INF -free regimens with Sofosbuvir. The recommended dosage is one capsule of 150 mg once daily for 12 weeks, taken with food2.
Sofosbuvir
Sofosbuvir is an HCV NS5B nucleotide analogue polymerase inhibitor. Phase 3 studies encompassed over 1700 patients with hepatitis C and included naive patients, patients who had already undergone treatment and had not responded or had relapsed, and patients with co -infection by HCV and HIV. The results were very promising with SVR greater than 90% in almost all the groups. Patients carriers of genotype 3 showed the worst response (30-32).
The pharmacokinetic properties of Sofosbuvir have been evaluated in healthy adult subjects and in subjects with chronic hepatitis C. After oral administration,
Sofosbuvir is rapidly converted in the liver to the metabolite GS-331007 that lacks anti-HCV activity in vitro, and accounts for greater than 90% of drug-related systemic exposure. Eighty per cent of the drug is eliminated by the kidney33.
The pharmacokinetic of Sofosbuvir was studied in HCV negative subjects with mild (CrCl ≥ 50 and < 80 ml/min per 1.73m2), moderate (CrCl ≥ 30 and < 50 ml/min per 1.73m2) and severe renal impairment (CrCl < 30 ml/min per 1.73m2) and subjects with ESRD requiring haemodialysis, following a single 400 mg dose of Sofosbuvir. Compared to subjects with normal renal function, the Sofosbuvir AUC was 61%, 107% and 171% higher in mild, moderate and severe renal impairment, respectively. No dose adjustment is recommended for patients with mild or moderate renal impairment, however the safety and efficacy of Sofosbuvir have not been established in patients with severe renal impairment or ESRD. No dose recommendation can be given at this time for patients with severe renal impairment or ESRD33.
Its use in renal transplant patients is facilitated since there are no described interactions with immunosuppressive drugs.
The Sofosbuvir efficacy has been established in subjects with all HCV genotypes infection, including those with hepatocellular carcinoma (awaiting liver transplantation) and those with HCV/HIV-1 co-infection. Treatment regimen and duration are dependent on both viral genotype and patient population, generally for 12 to 24 weeks. The recommended dose is one 400 mg tablet, taken orally, once daily with or without food33.
The EASL recommendations on the treatment of hepatitis C, suggests that Sofosbuvir can be used in INF -containing regimens in association with RBV (INF/ RBV/Sofosbuvir) in all genotypes of the virus. Sofosbuvir is also effective in INF-free regimens with Ribavirin (RBV/Sofosbuvir) in genotypes 2 and 3, or in INF -RBV-free regimens in combination with other DAAs, such as Simeprevir or Ledipasvir, in the treatment of patients carriers of genotypes 1 and 4, or in association with Daclastavir in all genotypes of the virus2.
Ledipasvir Plus Sofosbuvir
Is a two-drug fixed -dose combination product that contains 90 mg of Ledipasvir (a NS5A inhibitor) and 400 mg of Sofosbuvir (a nucleotide analogue NS5B polymerase inhibitor) in a single tablet. This association is effective in the treatment of chronic hepatitis C genotype 1 infection34,35.
The pharmacokinetic properties of Ledipasvir/Sofosbuvir, have been evaluated in healthy adult subjects and in subjects with chronic hepatitis C.
Following oral administration, Ledipasvir median peak concentrations were observed 4 to 4.5 hours post-dose, and Sofosbuvir 0.8 to 1 hour post-dose.
Biliary excretion of unchanged Ledipasvir is the major route of elimination, with renal excretion being a minor pathway (approximately 1%)36.
No clinically relevant differences in Ledipasvir pharmacokinetic were observed between healthy subjects and subjects with severe renal impairment, however as discussed previously, Sofosbuvir is eliminated mainly by the kidney. No dosage adjustment of Ledipasvir/Sofosbuvir is required for patients with mild or moderate renal impairment but the safety and efficacy have not been established in patients with CrCl < 30 ml/min per 1.73m2 or E SRD requiring haemodialysis36.
Symptomatic bradycardia, as well as fatal cardiac arrest and cases requiring pacemaker intervention, have been reported when amiodarone is co administered with these drugs36.
Ombitasvir, Paritaprevir with Ritonavir
Ombitasvir plus Paritaprevir are two direct –acting antiviral agents, combined in the same pill, with distinct mechanisms of action and non–overlapping resistance profiles to target HCV at multiple steps in the viral life-cycle.
Ombitasvir is an inhibitor of HCV NS5A, and Paritaprevir is an inhibitor of HCV NS3/4A protease, both essentials for viral replication. Ritonavir is not active against HCV, it is a CYP3A inhibitor that increases the systemic exposure of the CYP3A substrate Paritaprevir.
The efficacy and safety of these drugs in combination with Dasabuvir with and without RBV was evaluated in six randomized phase 3 clinical trials, in over 2,300 subjects with genotype 1 chronic hepatitis C infection.
In these studies 97% of the patients achieved SVR, and only 1.3% had post -treatment relapse. The most commonly reported adverse reactions (in more than 20% of subjects) were fatigue and nausea. The proportion of subjects who permanently discontinued treatment due to adverse reactions was 0.2%37 -40.
Ombitasvir is metabolized via amide hydrolysis followed by oxidative metabolism in the liver, and biliary excretion is a major elimination pathway (approximately 90%). Paritaprevir is also metabolized in the liver predominantly by CYP3A4 and to a lesser extent CYP3A5, and biliary excretion contributes to the elimination of more than 80% of the drug. Ritonavir is predominantly metabolised by the liver CYP3A, 90% is eliminated in the faeces and 10% is excreted in the urine41.
Pharmacokinetic in subjects with mild (CrCl: 60 to 89 ml/min per 1.73m2), moderate (CrCl: 30 to 59 ml/min per 1.73m2) and s evere (CrCl: 15 to 29 ml/ min per 1.73m2) renal impairment showed that Ombitasvir exposure is not different in renal failure. Paritaprevir AUC values were 19%, 33% and 45% higher in mild, moderate and severe renal impairment, and Ritonavir plasma concentrations increased 42%, 80% and 114% in subjects with mild, moderate and severe renal impairment, respectively41.
No dose adjustment is recommended in HCV-infected patients with mild, moderate or severe renal impairment, however phase 3 studies did not include HCV-infected patients on dialysis.
Preliminary results (RUBY study) in patients with severe renal failure and on haemodialysis were recently presented at the International Liver Congress 2015 in Vienna42.
Ritonavir is a strong inhibitor of CYP3A, so co –administration with medicinal products primarily metabolized by CYP3A may result in increased plasma concentrations of these products. The CYP3A substrates evaluated in drug interaction studies, which may require dose adjustment and/or clinical monitoring, include Cyclosporine and Tacrolimus. The recommendations are to give one fifth of the total daily dose of Cyclosporine once daily or 0.5 mg Tacrolimus once every week, with monitoring of trough levels and adjustments of the dose and/or dosing frequency as needed41.
The EASL recommendations on the treatment of hepatitis C suggest that these drugs are effective in combination with RBV in the treatment of HCV genotype 4, and associated with Dasabuvir with or without RBV in the treatment of HCV genotype 1, treatment time ranging from 12 to 24 weeks2.
DasabuvirDasabuvir is a non-nucleoside inhibitor of the HCV RNA-dependent RNA polymerase encoded by the NS5B gene. Co-administration of Dasabuvir with Ombitasvir/Paritaprevir/Ritonavir combines three direct-acting antiviral agents with distinct mechanisms of action. This association is effective in the treatment of HCV genotype 137-40.
The pharmacokinetic properties of the combination of Dasabuvir with Ombitasvir/Paritaprevir/Ritonavir have been evaluated in healthy adult subjects and in subjects with chronic hepatitis C. Dasabuvir is predominantly metabolized by CYP2C8 in the liver, and approximately 94% eliminated in faeces with limited excretion in urine43.
In subjects with mild, moderate and severe renal impairment, Dasabuvir mean AUC values were 21%, 37% and 50% higher, respectively, relative to subjects with normal renal function, but these changes in Dasabuvir exposures are not considered to be clinically significant43.
Who should be treated?
The goal of therapy is to cure HCV infection to prevent hepatic cirrhosis, hepatocellular carcinoma, severe extra -hepatic manifestations and death. The end point of therapy is undetectable HCV-RNA in a sensitive assay, 12 weeks (SVR12) and 24 weeks (SRV24) after the end of treatment2.
The HCV -RNA quantification and HCV genotype must be assessed prior to treatment initiation and will determine the choice of therapy. Liver disease severity should be assessed prior to therapy. Identifying patients with cirrhosis is of particular importance, as their prognosis is altered and their treatment regimen may be adapted. Although widely performed and accepted as the gold -standard method to evaluate hepatic fibrosis, liver biopsy is an invasive technique with associated morbidity and mortality.
Transjugular liver biopsy is an alternative procedure especially used in patients with higher bleeding risk, such as chronic kidney disease patients. Fibrosis stage can also be assessed by non-invasive methods, such as hepatic fibroscan. These non -invasive methods have shown good diagnostic performance to predict the severity of liver fibrosis in chronic kidney disease patients44.
All treatment-naive and treatment–experienced patients with chronic liver disease due to HCV should be considered for therapy. The treatment should be prioritized for patients with significant fibrosis or cirrhosis.
The treatment should also be prioritized regardless of the fibrosis stage in patients with HIV or HBV co-infection and patients with significant extra–hepatic manifestations, such as HCV-related mixed cryoglobulinaemia, HCV immune complex-related nephropathy and non-Hodgkin B cell lymphoma. Patients at risk of transmitting HCV, such as drug abusers, patients with promiscuous sexual habits and haemodialysis patients should also be considered high -priority for therapy2.
Haemodialysis patients, particularly those who are suitable candidates for renal transplantation, should be treated before kidney transplantation. HCV treatment before kidney transplantation may avoid liver-related morbidity and mortality in the post-transplant patient, and may prevent HCV -specific causes of renal graft dysfunction7,14,16. HCV eradication before transplantation improves patient survival and reduces the occurrence of chronic graft nephropathy and post-transplant diabetes mellitus.
How to treat patients with chronic renal failure
The combination of PEG -INF and RBV was previously the standard treatment for chronic HCV in the general population, but is quickly being replaced by regimens that also contain DAAs and by INF-free and RBV-free regimens. The EASL recommendations on the treatment of HCV hepatitis, provided advice about therapies approved in the European Union for the treatment of hepatitis C in 20152. The selection of the antiviral regimen depends upon the extent of underlying liver disease and on viral genotype. For example, six treatment options are available for patients infected with HCV genotype 1, the most common in the world, including 2 INF-containing regimens and 4 INF-free regimens. However, the large registration trials of agents used for the treatment of HCV infection have excluded patients with significant renal impairment.
For patients with CrCl greater tha n 30 ml/min per 1 .73m2 the regim en selection is the same as that for patients without renal impairment. For patients with CrCl less than 30 ml/min per 1.73m2 limited data are available. Much of the data on antiviral efficacy in the setting of renal impairment is with the standard interferon therapy.
INF mono -therapy is not recommended for the treatment of chronic HCV patients without renal impairment.
However, some experts consider it an important option for patients with chronic kidney disease, because of concerns about the safety and limited data of other agents. The KDIGO guidelines for the treatment of hepatitis C in chronic kidney disease, suggest for patients with stages 3, 4 and 5 not yet on dialysis, mono-therapy with PEG -INF and for stage 5 on dialysis mono-therapy with standard INF7. Overall, SVR rates were generally low (< 50%) and in several studies treatment with standard INF was stopped due to side effects in up to 54% of patients 45-49.
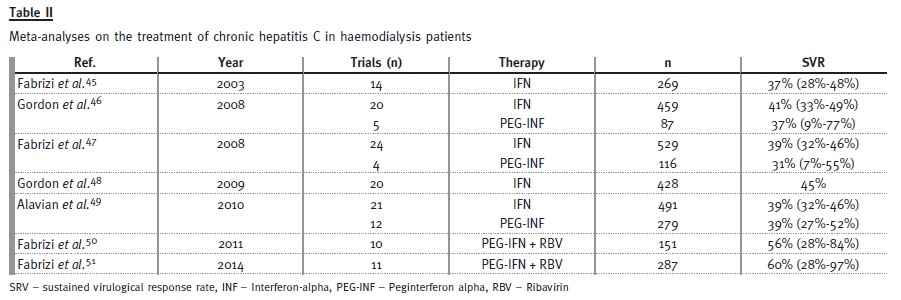
There have been several trials of hepatitis C treatment in haemodialysis patients, mostly uncontrolled and with different therapeutic regimens. These trials have been included in many meta-analyses, some of which are listed in Table 2. The SVR rates derived from meta -analyses appear not to be very different for the use of standard IFN or PEG-IFN. As with the standard INF, the antiviral efficacy of PEG -INF alone is low among patients on haemodialysis (SVR < 50%).
However, the addition of Ribavirin seems to provide a significant increase in SVR50,51. One open-label, randomized, controlled trial compared PEG-INF alfa-2, with PEG-INF alfa -2 plus low dose RBV in haemodialysis patients with HCV genotype 1. After 48 weeks of treatment, combination therapy achieved greater SVR rate than mono-therapy (64% versus 33%). Adverse event-related withdrawal rates were 7% in the combination therapy and 4% in the mono -therapy group52. However, the proportion of patients who had haemoglobin values < 8.5g/dl was significantly higher in the dual therapy group (72 versus 6%). A similar study in patients with HCV genotype 2 also showed a greater SVR rate with combination therapy (74% versus 44%), with good tolerance53.
The PEG -INF and RBV remain a treatment option for patients with severe renal impairment. It is recommended to use PEG -IFN (preferably PEG -IFN α2a) once a week, after dialysis session, in combination with low dose RBV. The RBV dose should be initiated with 200 mg once a week, followed by increments of 200 mg every two weeks until the maximum tolerated dose (stable levels of haemoglobin above 10 g/dL are often required). Recommended treatment time ranges from 24 to 48 weeks54.
For HCV positive patients undergoing haemodialysis, the optimal treatment should be an INF-RBV-free regimen. No safety dosing and efficacy data are available with the new DAAs drugs in this population, so these drugs should be used with caution.
However, isolated cases of successful treatment with INF -RBV -free regimens have now been reported.
The association with standard-dose of Simeprevir in combination with half -standard dose of Sofosbuvir may be helpful55. Preliminary results of the first study which examined the safety and efficacy of the combination Ritonavir-boosted Paritaprevir, Ombitasvir and Dasabuvir regimen in non–cirrhotic HCV genotype 1 patients with chronic kidney disease with estimated glomerular filtration rate < 30 mL/min/1.73 m2, was presented in the 50th International Liver Congress, April 2015, Vienna (RUBY trial)(46).
This open -label phase 3b study enrolled 20 patients, 65% on haemodialysis. As most patients have not yet reached post-treatment week 12, conclusions on efficacy are limited. Nevertheless, all patients completing treatment have had a good virological response so far.
The largest INF-RBV -free regimen study presented in patients with renal impairment was the C-SURFER study56. In this placebo -controlled trial, 224 patients were randomized to immediate treatment with Grazoprevir/Elbasvir (GZR/EBR) or deferred treatment. In the deferred group the patients received placebo for 12 weeks then GZR/EBR starting at follow-up week4. All patients had a CrCl < 30 ml/min per 1.73m2, and the study included patients on haemodialysis.
In the intent-to-treat analysis, an impressive 94% of study participants achieved an SVR12. The overall safety was very good with 0 discontinuations of study drug due to adverse events. Adverse events, such as headache, nausea and diarrhoea, were equally distributed between patients receiving the study drug versus placebo. The efficacy and safety of Grazoprevir (an HCV NS3/A4 protease inhibitor) combined with Elbasvir (an HVC NS5A inhibitor) were previously assessed in patients with HCV genotype 1 infection without renal failure in phase 2 studies57.
The good results of these studies support the ongoing phase 3 development of Grazoprevir plus Elbasvir.
This INF-RBV -free treatment, not yet approved in the European Union, promises great hope for therapy in patients with renal impairment.
There are still many questions regarding efficacy and needs for dose adjustments with the new DAAs in the treatment of HCV hepatitis in ESRD. Studies with larger numbers of patients are needed to find the best drug association and the necessity for dose adjustments. The EASL recommends that Simeprevir and the combination of Ritonavir -boosted Paritaprevir, Ombitasvir and Dasabuvir can be used in severe renal disease, however Sofosbuvir should not be administered to patients with CrCl < 30ml/min/1.73m2 or on haemodialysis2.
KIDNEY TRANSPLANT PATIENTS
In the past, antiviral theraphy was contraindicated for patients who have undergone renal transplantation.
The use of INF is associated with increased risk of acute rejection. In addition to viral activity, INF has pleiotropic effects including antiproliferative and immunomodulatory properties58. INF also induces cytokine gene expression, increased cell surface expression of HLA antigens, and enhanced function of natural killer cells, cytotoxic T cells, and monocytes.
The KDIGO guidelines for the treatment of hepatitis C in chronic kidney disease, suggest that HCV-infected kidney transplant recipients must be considered for treatment only when the benefits of treatment outweigh the risk of rejection due to INF -based therapy, such as fibrosing cholestatic hepatitis or life-threatening vasculitis7.
Outcomes of INF -based therapy after kidney transplantation are disappointing. In a meta-analysis published by Fabrizi et al. in 2006, treatment with INF with or without RBV was associated with SVR and treatment -related withdrawal rates of 18% and 35%, respectively59. A more recent meta –analysis published by Wei et al. in 2014, reported that the overall SVR rate, dropout rate, and graft rejection rate was 26.6%, 21.1% and 4%, respectively60. The overall SVR rate in PEG -INF based and standard INF-based therapy was 40.6% and 20.9%, respectively.
So PEG-INF-based therapy may be a more effective approach for treating HCV infection in renal transplant patients. The early studies reported that graft dysfunction occurred in 15%-100% of HCV-positive kidney transplant patients treated with INF, with up to 20% resultant permanent allograft failure.
Baid et al. noted that the risk for acute rejection is higher during the first year after transplantation, thus it is recommended to wait at least one year to initiate INF-regimen therapy63. However, more recent studies have shown lower graft rejection rates, between 0% and 5%. The use of less immunogenic PEG-INF is a possible explanation for this observation.
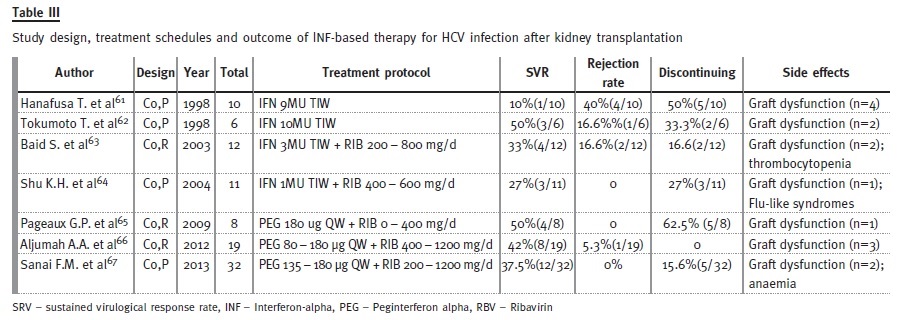
After all, SRV are still relatively low (38% -50%), and dropout rates remain high. Unlike in non-transplant setting, there are no large, controlled clinical trials to test the efficacy of anti-HCV therapy in kidney transplant patients. Most of the published reports describe small cohort studies or case reports (Table 3), and minimal data exist on the use of INF-free regimens in this population61-67.
Although there is no safety and efficacy data regarding the use of DAAs in the kidney transplant setting, some recent cases reported in the literature suggest that kidney transplant recipients may benefit from the use of new antiviral drugs, with high SVR and an excellent safety profile68-70. If kidney function allows, an INF -free regimen is preferred, with careful monitoring of drug -drug interactions between DAAs and immunosuppression therapy such as Cyclosporine and Tacrolimus.
CONCLUSION
The ultra -structural characterization of non-structural proteins involved in viral replication was the key to the development of new therapeutic strategies to cure HCV hepatitis. The success of the new therapeutics is deeply associated with the combination of pharmaceuticals that inhibit a lot of those proteins, acting in conjunction to inhibit the virus replication. With SVR greater than 90%, and a favourable safety profile, it may be possible to imagine the global eradication of HCV infection.
However, major challenges remain: infection is often diagnosed at a late stage, the high cost of DAAs may lead to selective use and reinfection remains possible.
The large studies that have shown the efficacy and safety of the new DAA drugs did not include patients with advanced chronic renal failure or renal transplant patients. While for some DAAs, such as, for example, Sofosbuvir, a dosage adjustment to renal function is necessary, for others like Ombitasvir/Paritaprevir/Ritonavir there are interactions with immunosuppressive drugs that require dose adjustments and close monitoring of trough levels.
The use of DAAs in these patients is not well studied and its administration is recommended with caution.
However, preliminary results of ongoing studies bring hope for future therapeutic regimens without INF or RBV. Some drugs not yet approved in the European Union, such as the association of Grazoprevir with Elbasvir, included in the phase 3 studies patients with advanced renal failure and on haemodialysis, may also be a therapeutic alternative in the future.
Current guidelines for the treatment of HCV positive patients with chronic renal failure, recommend that patients accepted for kidney transplant be treated before entering the waiting list. The HCV positive patients with no indication for transplantation are excluded from the therapeutic indications.
For patients already transplanted the guidelines recommend treatment of only the patients who experience serious complications attributed to HCV, such as fibrosing cholestatic hepatitis or vasculitis. With availability of the new DAA drugs for the treatment of hepatitis C showing higher effectiveness and having lower toxicity than previous therapies, it has become questionable if we should treat all HCV positive patients on dialysis and with a kidney transplant.
We hope that it may be possible in the future to eradicate HCV infection in our patients, however much work remains to be done to come up with the best therapeutic regimen and approach to achieve this goal.
References
1. Chung RT, Baumert TF. Curing chronic hepatisis C -the arc of a medical Ttriumph. N Engl J Med 2014; 370(17):1576 -1578. [ Links ]
2. European Association for the Study of the Liver. Recommendations on the treatment of hepatitis C. 2015 http://www.easl.eu/medias/cpg/HEPC-2015/Summary.pdf [ Links ]
3. Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age -specific antibody to HCV seroprevalence. Hepatology 2013;57(4):1333–1342. [ Links ]
4. Finelli L, Miller JT, Tokars JI, Alter MJ, Arduino MJ. National surveillance of dialysis-assotiated diseases in the United States, 2002. Semin Dial 2005;18(1):52 -61. [ Links ]
5. Jadoul M, Poignet JL, Geddes C, et al. with the PHCV Collaborative Group. The changing epidemiology of hepatitis C virus infection in haemodialysis: European multicentre study. Nephrol Dial Transplant 2004;19(4):904-909. [ Links ]
6. Su Y, Norris JL, Zang C, Peng Z, Wang N. Incidence of hepatitis C virus infection in patients on hemodialysis: a systematic review and meta -analysis. Hemodial Int 2013;17(4):532–541. [ Links ]
7. Kidney Disease Improving Global Outcomes (KDIGO). KDIGO clinical practice guidelines for the prevention, diagnosis, evaluation, and treatment of hepatitis C in chronic kidney disease. Kidney Int 2008; 73 (Suppl 109):S1 -S2. [ Links ]
8. http://www.ordemdosmedicos.pt Manual de Boas Práticas de Diálise Crónica. Aprovado pelo Conselho Executivo da Ordem dos Médicos a 2 de Setembro de 2011, D7-9. [ Links ]
9. Fabrizi F, Lunghi G, Andrulli S, et al. Influence of hepatitis C virus viraemia upon serum aminotransferase activity in chronic dialysis patients. Nephrol Dial Transplant 1997;12(7):1394 -1398. [ Links ]
10. Furusyo N, Hayashi J, Kakuda K, et al. Acute hepatitis C among Japanese hemodialysis patients: a prospective 9-year study. Am J Gastroenterol 2001;96(5):1592–1600. [ Links ]
11. Liu CH, Kao JH. Treatment of hepatitis C virus infection in patients with end–stage renal disease. J Gastroenterol Hepatol 2011;26(2):228 -239. [ Links ]
12. Lemos LB, Perez RM, Matos CA, Silva IS, Silva AE, Ferraz ML. Clinical and laboratory characteristics of acute hepatitis C in patients with end-stage renal disease on hemodialysis. J Clin Gastroenterol 2008;42(2):208–211. [ Links ]
13. Okuda K, Yokosuka O. Natural history of chronic hepatitis C in patients on hemodialysis: case control study with 4 -23 years of follow-up. World J Gastroenterol 2004;10(15):2209–2212. [ Links ]
14. Singh N, Neidlinger N, Djamali A, et al. The impact of hepatitis C virus donor and recipient status on long-term kidney transplant outcomes: University of Wisconsin experience. Clin Transplant 2012;26(5):684–693. [ Links ]
15. de Oliveira Uehara SN, Emori CT, da Silva Fucuta Pereira P, et al. Histological evolution of hepatitis C virus infection after renal transplantation. Clin Transplant 2012;26(6):842–848. [ Links ]
16. Morales JM, Marcén R, Andres A, et al. Renal transplantation in patients with hepatitis C virus antibody. A long national experience. NDT Plus 2010; 3(Suppl 2):ii41–ii46. [ Links ]
17. Wills RJ. Clinical pharmacokinetics of interferons. Clin Pharmacokinet 1990;19(5):390–399. [ Links ]
18. Uchihara M, Izumi N, Sakai Y, et al. Interferon therapy for chronic hepatitis C in hemodialysis patients: increased serum levels of interferon. Nephron 1998;80(1):51–56. [ Links ]
19. Zeuzem S, Welsch C, Herrmann E. Pharmacokinetics of peginterferons. Semin Liver Dis 2003;23(Suppl 1):23–28. [ Links ]
20. Wade JR, Snoeck E, Duff F, Lamb M, Jorga K. Pharmacokinetics of ribavirin in patients with hepatitis C virus. Br J Clin Pharmacol 2006;62(6):710–714. [ Links ]
21. Berenguer M. Treatment of chronic hepatitis C in hemodialysis patients. Hepatology 2008;48(5):1690–1699. [ Links ]
22. Russmann S, Grattagliano I, Portincasa P, Palmieri VO, Palasciano G. Ribavirin-induced anemia: mechanisms, risk factors and related targets for future research. Curr Med Chem 2006;13(27):3351–3357. [ Links ]
23. De Franceschi L, Fattovich G, Turrini F, et al. Hemolytic anemia induced by ribavirin therapy in patients with chronic hepatitis C virus infection: role of membrane oxidative damage. Hepatology 2000;31(4):997–1004. [ Links ]
24. Treitel M, Marbury T, Preston RA, et al. Single -dose pharmacokinetics of boceprevir in subjects with impaired hepatic or renal function. Clin Pharmacokinet 2012;51(9):619-628.
25. Dumortier J, Guillaud O, Gagnieu MC, et al. Anti -viral triple therapy with telaprevir in haemodialysed HCV patients: is it feasible? J Clin Virol 2013;56(2):146 -149. [ Links ]
26. Jabobson IM, Dore GJ, Foster GR et al. Simeprevir with pegylated interferon alfa 2a plus ribavirin in treatment -naive patients with chronic hepatitis C virus genotype 1 infection (QUEST -1): a phase 3, randomised, double -blind, placebo -controlled trial. Lancet 2014;384(9941):403 -413. [ Links ]
27. Manns M, Marcellin P, Poordad F, et al. Simeprevir with pegylated interferon alfa 2a or 2b plus ribavirin in treatment -naive patients with chronic hepatitis C virus genotype 1 infection (QUEST -2): a randomised, double -blind, placebo –controlled phase 3 trial. Lancet 2014;384(9941):414 -426. [ Links ]
28. Forns X, Lawitz E2, Zeuzem S, et al. Simeprevir with peginterferon and ribavirin leads to high rates of SVR in patients with HCV genotype 1 who relapsed after previous therapy: a phase 3 trial. Gastroenterology 2014;146(7):1669 -1679. [ Links ]
29. Olysio (simeprevir) product information. Available online at http://ec.europa.eu/health/documents/communityregister/2014/20140514128513/anx_128513_pt.pdf [ Links ]
30. Lawitz E, Mangia A, Wyles D, et al. Sofosbuvir for previously untreated chronic hepatitis C infection. N Engl J Med 2013;368(20):1878 -1887. [ Links ]
31. Jacobson IM, Gordon SC, Kowdley KV, et al. with the POSITRON Study and the FUSION Study. Sofosbuvir for hepatitis C genotype 2 or 3 in patients without treatment options. N Engl J Med 2013;368(20):1867-1877. [ Links ]
32. Zeuzem S, Dusheiko GM, Salupere R, et al. with the VALENCE Investigators. Sofosbuvir and ribavirin in HCV genotypes 2 and 3. N Engl J Med 2014;370(21):1993 -2001. [ Links ]
33. Solvadi (sofosbuvir) product information. Available online at http://www.ema.europa.eu/docs/pt_PT/document_library/EPAR_Product_Information/human/002798/WC500160597. [ Links ]
34. Afdhal N, Zeuzem S, Kwo P, et al. with the ION-1 Investigators. Ledipasvir and sofosbuvir for untreated HCV genotype 1 infection. N Engl J Med 2014;370(20):1889-1898. [ Links ]
35. Afdhal N, Reddy KR, Nelson DR, et al. with the ION -2 Investigators. Ledipasvir and sofosbuvir for previously treated HCV genotype 1 infection. N Engl J Med 2014;370(16):1483 -1493. [ Links ]
36. Harvoni (sofosbuvir, ledispavir) product information, Available online at http://ec.europa.eu/health/documents/communityregister/2014/20141117130011/anx_130011_pt.pdf [ Links ]
37. Feld JJ, Kowdley KV, Coakley E, et al. Treatment of HCV with ABT -450/r –ombitasvir and dasabuvir with ribavirin. N Engl J Med 2014;370(17):1594 -1603. [ Links ]
38. Zeuzem S, Jacobson IM, Baykal T, et al. Retreatment of HCV with ABT-450/r-ombitasvir and dasabuvir with ribavirin. N Engl J Med 2014;370(17):1604 -1614. [ Links ]
39. Andreone P, Colombo MG, Enejosa JV, et al. ABT-450, ritonavir, ombitasvir, and dasabuvir achieves 97% and 100% sustained virologic response with or without ribavirin in treatment -experienced patients with HCV genotype 1b infection. Gastroenterology 2014;147(2):359 -365. [ Links ]
40. Ferenci P, Bernstein D, Lalezari J, et al. with the PEARL -III Study; PEARL -IV Study. ABT-450/r-ombitasvir and dasabuvir with or without ribavirin for HCV. N Engl J Med 2014;370(21):1983 -1992. [ Links ]
41. Viekirax (ombitasvir, paritaprevir, ritonavir) product information. Available online at http://ec.europa.eu/health/documents/community-register/2015/20150115130406/anx_130406_en.pdf [ Links ]
42. Pockros P, et al. Safety of ombitasvir/paritaprevir/ritonavir plus dasabuvir for treating HCV GT1 infection in patients with severe renal impairment or end -stage renal disease: The RUBY -I Study. 50th International Liver Congress (ILC), April 22 -26, Vienna, Austria; abstract L01. [ Links ]
43. Exviera (dasabuvir) product information. Available online at http://ec.europa.eu/health/documents/communityregister/2015/20150115130446/anx_130446_en.pdf
44. Liu CH, Liang CC, Huang KW, et al. Transient elastography to assess hepatic fibrosis in hemodialysis chronic hepatitis C patients. Clin J Am Soc Nephrol 2011;6(5):1057–1065. [ Links ]
45. Fabrizi F, Dulai G, Dixit V, Bunnapradist S, Martin P. Meta -analysis: interferon for the treatment of chronic hepatitis C in dialysis patients. Aliment Pharmacol Ther 2003;18(11 -12):1071–1081. [ Links ]
46. Gordon CE, Uhlig K, Lau J, Schmid CH, Levey AS, Wong JB. Interferon treatment in hemodialysis patients with chronic hepatitis C virus infection: a systematic review of the literature and meta -analysis of treatment efficacy and harms. Am J Kidney Dis 2008;51(2):263–277. [ Links ]
47. Fabrizi F, Ganeshan SV, Lunghi G, Messa P, Martin P. Antiviral therapy of hepatitis C in chronic kidney diseases: meta -analysis of controlled clinical trials. J Viral Hepat 2008;15(8):600–606. [ Links ]
48. Gordon CE, Uhlig K, Lau J, Schmid CH, Levey AS, Wong JB. Interferon for hepatitis C virus in hemodialysis–an individual patient meta-analysis of factors associated with sustained virological response. Clin J Am Soc Nephrol 2009;4(9):1449–1458. [ Links ]
49. Alavian SM, Tabatabaei SV. Meta -analysis of factors associated with sustained viral response in patients on hemodialysis treated with standard or pegylated interferon for hepatitis C infection. Iran J Kidney Dis 2010;4(3):181–194. [ Links ]
50. Fabrizi F, Dixit V, Martin P, Messa P. Combined antiviral therapy of hepatitis C virus in dialysis patients: meta -analysis of clinical trials. J Viral Hepat 2011;18(7):e263–269. [ Links ]
51. Fabrizi F, Dixit V, Messa P, Martin P. Antiviral therapy (pegylated interferon and ribavirin) of hepatitis C in dialysis patients: meta -analysis of clinical studies. J Viral Hepat 2014;21(10): 681–689. [ Links ]
52. Liu CH, Huang CF, Liu CJ, et al. Pegylated interferon-α2a with or without low –dose ribavirin for treatment -naive patients with hepatitis C virus genotype 1 receiving hemodialysis: a randomized trial. Ann Intern Med 2013;159(11):729–738. [ Links ]
53. Liu CH, Liu CJ, Huang CF, et al. Peginterferon alfa -2a with or without low -dose ribavirin for treatment -naive patients with hepatitis C virus genotype 2 receiving haemodialysis: a randomised trial. Gut 2015; 64(2):303 -311. [ Links ]
54. Carvalho -Filho RJ, Feldner AC, Silva AE, Ferraz ML. Management of hepatitis C in patients with chronic kidney disease. World J Gastroenterol 2015;21(2):408 -422. [ Links ]
55. Perumpail RB, Wong RJ, Há LD, et al. Sofosbuvir and simeprevir combination therapy in the setting of liver transplantation and hemodialysis. Transpl Infect Dis 2015;17(2):275 -278. [ Links ]
56. Roth D et al. C -SURFER: Grazoprevir plus elbasvir in treatment-naïve and treatment experienced patients with hepatitis C virus genotype 1 infection and chronic kidney disease. 50th International Liver Congress (ILC), April 22 -26, 2015, Vienna, Austria; abstract LP02. [ Links ]
57. Lawitz E, Gane E, Pearlman B, et al. Efficacy and safety of 12 weeks versus 18 weeks of treatment with grazoprevir (MK -5172) and elbasvir (MK -8742) with or without ribavirin for hepatitis C virus genotype 1 infection in previously untreated patients with cirrhosis and patients with previous null response with or without cirrhosis (C -WORTHY): a randomized, open-label phase 2 trial. Lancet 2015;385(9973):1075-1086. [ Links ]
58. Black M, Peters M. Alpha-interferon treatment of chronic hepatitis C: need for accurate diagnosis in selecting patients. Ann Intern Med 1992;116(1):86 -88. [ Links ]
59. Fabrizi F, Lunghi G, Dixit V, Martin P. Meta-analysis: anti-viral therapy of hepatitis C virus-related liver disease in renal transplant patients. Aliment Pharmacol Ther 2006;24(10):1413–1422. [ Links ]
60. Wei F, Liu J, Liu F, Hu H, Ren H, Hu P. Interferon -based anti -viral therapy for hepatitis C virus infection after renal transplantation: an updated meta -analysis. PLoS One 2014;9(4):e90611. [ Links ]
61. Hanafusa T, Ichikawa Y, Yazawa K, et al. Hepatitis C virus infection in kidney transplantation and a pilot study of the effects of interferon-alpha therapy. Transplant Proc 1998;30(1): 122–124. [ Links ]
62. Tokumoto T, Tanabe K, Ishikawa N, et al. Effect of interferon -alfa treatment in renal transplant recipients with chronic hepatitis C. Transplant Proc 1998;30(7): 3270–3272. [ Links ]
63. Baid S, Tolkoff -Rubin N, Saidman S, et al. Acute humoral rejection in hepatitis C-infected renal transplant recipients receiving antiviral therapy. Am J Transplant 2003;3(1):74–78. [ Links ]
64. Shu KH, Lan JL, Wu MJ, et al. Ultra -low dose alpha -interferon plus ribavirin for the treatment of active hepatitis C in renal transplant recipients. Transplantation 2004;77(12):1894 -1896. [ Links ]
65. Pageaux GP, Hilleret MN, Garrigues V, et al. Pegylated interferon -alpha -based treatment for chronic hepatitis C in renal transplant recipients: an open pilot study. Transpl Int 2009;22(5):562–567. [ Links ]
66. Aljumah AA, Saeed MA, Al Flaiw AI, et al. Efficacy and safety of treatment of hepatitis C virus infection in renal transplant recipients. World J Gastroenterol 2012;18(1):55–63. [ Links ]
67. Sanai FM, Mousa D, Al -Mdani A, et al. Safety and efficacy of peginterferon -(alpha)2a plus ribavirin treatment in renal transplant recipients with chronic hepatitis C. J Hepatol 2013;58(6):1096 -1103. [ Links ]
68. Delabaudière C, Lavayssière L, Dörr G, et al. Successful treatment of fibrosing cholestatic hepatitis with pegylated interferon, ribavirin and sofosbuvir after a combinated kidney -liver transplantation. Transpl Int 2015;28(2):255 -258. [ Links ]
69. Bonacci M, Londoño MC, Esforzado N, Forns X, Sotoca JM, Campistol JM. Antiviral treatment with sofosbuvir and simeprevir in a kidney transplant recipient with HCV-decompensated cirrhosis: viral eradication and removal from the liver transplant waiting list. Transpl Int 2015;28(11):1345 -1349 [ Links ]
70. Kwo PY, Badshah MB. New hepatitis C virus therapies: drug classes and metabolism, drug interactions relevant in the transplant settings, drug options in decompensated cirrhosis, and drug options in end -stage renal disease. Curr Opin Organ Transplant 2015;20(3):235 -241. [ Links ]
Drª Alice Santana
Department of Nephrology and Kidney Transplantation
Hospital de Santa Maria, Centro Hospitalar Lisboa Norte
Av. Prof Egas Moniz, 1649-035 Lisboa, Portugal.
E-mail: alicesantana1@sapo.pt
Conflict of interest statement: None declared
Received for publication: 26/09/2015
Accepted: 12/10/2015


{kind=link}
{kind=link}
{kind=link}