










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.30 no.1 Lisboa mar. 2016
ORIGINAL ARTICLE
Idiopathic nephrotic syndrome – Deflazacort, an alternative?
Síndrome nefrótico idiopático – Deflazacorte, uma alternativa?
Catarina Neves, Ana Carolina Cordinhã, Carmen Ferreira, Clara Gomes, António Jorge Correia
Paediatric Nephrology Unit, Hospital Pediátrico de Coimbra, Centro Hospitalar e Universitário de Coimbra, EPE, Coimbra, Portugal.
ABSTRACT
Background: Prednisolone has been the first-line therapy in the treatment of idiopathic nephrotic syndrome in children. Recurrences are common, and the need for repeated high doses of prednisolone alone or in combination with other immunosuppressants may induce significant side effects. Deflazacort has been used in recent years as an alternative, but there are not many studies on its effectiveness in maintenance therapy. The aim of this study was to assess the efficacy and safety of deflazacort maintenance therapy in childhood idiopathic nephrotic syndrome. Methods: Retrospective observational review of patients with steroid-dependent idiopathic nephrotic syndrome who had received previous treatment with prednisolone and were under deflazacort for at least a year. Steroid-dependent idiopathic nephrotic syndrome was defined when relapses occurred during the reduction of corticosteroid therapy or up to two weeks after its withdrawal. We compared the number of relapses, steroid dose at relapse, the period of time without recurrence and side effects in the twelve months of therapy before and after the introduction of deflazacort. Results: We included 20 patients, 75% were male. At diagnosis of idiopathic nephrotic syndrome, the median age was 3.4 years. All children had begun treatment with prednisolone, which was replaced by deflazacort on average 2.7 years after diagnosis. After the first year of therapy with deflazacort, we found a significant reduction in the number of relapses (mean 0.5 vs. 2.0; p < 0.001) and the side effects of corticosteroids (p = 0.037). There were no significant differences in other variables. Conclusions: In this sample, deflazacort was associated with a small number of side effects and relapses, as compared to prednisolone, proving to be a safe and effective therapy in the maintenance treatment of idiopathic nephrotic syndrome in children.
Key-Words: Children; deflazacort; efficacy; idiopathic nephrotic syndrome; safety.
RESUMO
Introdução: A prednisolona tem sido a terapia de primeira linha para o tratamento do síndrome nefrótico idiopático da infância. As recidivas são comuns e a necessidade de repetidas doses elevadas de prednisolona ou em combinação com outros imunossupressores podem induzir efeitos secundários significativos. O deflazacorte foi utilizado nos últimos anos como uma alternativa, mas não existem muitos estudos sobre a sua eficácia na terapia de manutenção. O objetivo deste estudo foi verificar a eficácia e a segurança da terapia de manutenção com deflazacorte no síndrome nefrótico idiopático da criança. Métodos: Estudo observacional retrospetivo de pacientes com síndrome nefrótico idiopático corticodependente que tinham recebido tratamento prévio com prednisolona e estavam sob deflazacorte por pelo menos um ano. O síndrome nefrótico idiopático corticodependente foi definido quando ocorreram recidivas durante a redução da terapêutica com corticosteróides ou até duas semanas após a sua retirada. Comparou-se o número de recaídas, a dose de esteróides na recidiva, o período de tempo sem recidivas e efeitos secundários nos doze meses de tratamento, antes e após a introdução de deflazacorte. Resultados: Foram incluídos 20 pacientes, 75% do sexo masculino. No momento do diagnóstico do síndrome nefrótico idiopático a idade média era de 3.4 anos. Todas as crianças tinham começado o tratamento com prednisolona, que é substituído para o deflazacorte em mediana 2.7 anos após o diagnóstico. Após o primeiro ano de terapia com deflazacorte, encontrámos uma redução significativa do número de recaídas (média de 0.5 vs. 2.0; p < 0.001) e dos efeitos secundários dos corticóides (p = 0.037). Não existiram diferenças significativas em outras variáveis. Conclusões: Nesta amostra, o deflazacorte foi associado com um menor número de efeitos secundários e recaídas em comparação com a prednisolona, provando ser uma terapia segura e eficaz no tratamento de manutenção do síndrome nefrótico idiopático em crianças.
Palavras-Chave: Crianças; deflazacorte; eficácia; segurança; síndrome nefrótico idiopático.
INTRODUCTION
The idiopathic nephrotic syndrome (INS) in children has an incidence that varies in the literature from 2 to 16 /100,000 children1-4. Corticosteroids have been the first-line therapy, since the mid-twentieth century, as 90-95% of patients respond to this therapy and mortality decreased from 35% to 3% after its introduction1,4,5.
However, corticosteroids are associated with numerous side effects, such as, cushingoid appearance, growth retardation, glucose intolerance, hypertension, osteoporosis and suppression of adrenal gland1,3,6,7. The INS relapses are frequent in childhood and the need for high and repeated doses of corticosteroids alone or in combination with cyclophosphamide, cyclosporine, mycophenolate mofetil or levamisole, can induce significant side effects1,3,5. A new corticosteroid derivative of prednisolone was introduced in 1969, deflazacort8.
This has been used in recent years as an alternative for maintenance therapy in paediatric INS and has shown superior or the same efficacy than prednisolone, with fewer side effects1,2,8,9. However, there has not been widespread use.
The aim of this study was to assess the efficacy and safety of deflazacort maintenance therapy in childhood INS.
METHODS
Analytical retrospective observational study of medical records of patients with steroid-dependent INS that had been treated with deflazacort. We excluded patients in whom it was necessary to use other immunosuppressive therapy. All patients included had undergone previous treatment with prednisolone that had been replaced by deflazacort for at least one year. The induction therapy in the first episode consisted of prednisolone 60mg/m2/day for 6 weeks followed by 40mg/m2 on alternate days for 6 weeks, with subsequent slow decrease of corticosteroid therapy. The relapse was defined with the appearance of proteinuria equal to or higher than three crosses in the quick urine test for three or more consecutive days. In relapse, prednisolone therapy consisted of 60mg/m2/day or deflazacort equipotent dose of up to three consecutive days without proteinuria, followed by 40mg/m2 on alternate days for 4 weeks, with subsequent slow decrease of corticosteroid therapy. Steroid-dependent INS was defined as the occurrence of a relapse during the reduction of corticosteroid therapy or up to two weeks after their suspension3. We considered as equipotent dose 1.2 mg of deflazacort to 1mg of prednisolone1,6,8,10.
The following variables were evaluated: the number of relapses, the dose of corticosteroids at the time of relapse, the time to remission, the time without relapse, weight and height standard deviation scores (SDS) and side effects of therapy (Cushings syndrome, hirsutism, intracranial hypertension, glucose intolerance and hypertension) during the first year of treatment with deflazacort and the year before under therapy with prednisolone, comparing the results. Statistical analysis was performed using Excel 2007 and SPSS 17 software.
RESULTS
We included 20 patients, 15 (75%) of them were male. At the time of diagnosis of INS the median age was 3.4 years (1.1 to 13.1 years), weight SDS was 0.80 (minimum -0.85, maximum 1.93), height SDS was -0.12 (minimum -1.23, maximum 0.92) and body mass index (BMI) SDS was 0.9 (minimum -0.81, maximum 2.29). On this date, 10% of patients had hypertension (HT) or microhaematuria. All patients underwent induction therapy after diagnosis and the recurrences with prednisolone. The deflazacort was added in median 2.7 years (minimum 0.5, maximum 9.1 years) after the diagnosis of INS. At the time of introduction of deflazacort, all patients met criteria for steroiddependent INS, none had haematuria and one had HT, being treated with enalapril.
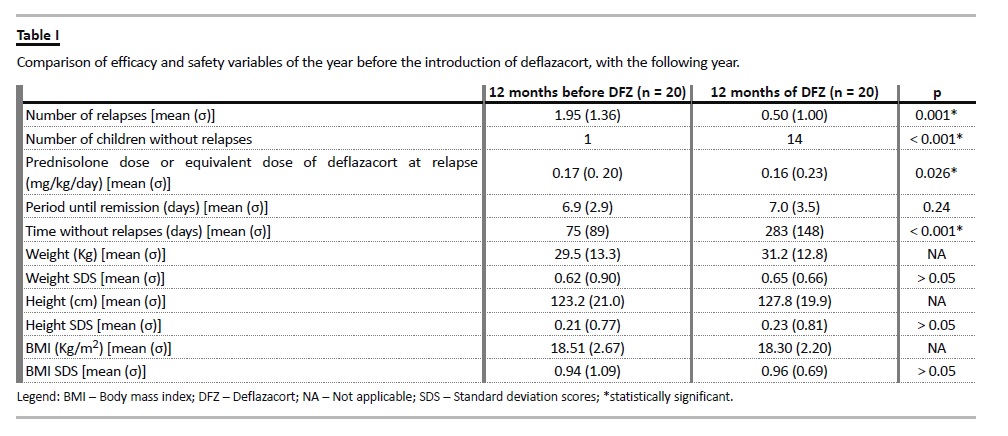
During the first year of therapy with deflazacort there was a significant reduction in the number of relapses (average of 0.5/year versus 2.0/year; p <0.001); increase in the number of children without relapses (14 versus 1 on the year before the introduction of deflazacort, p < 0.001) and in the relapse-free period (average of 283 days versus 75 days in the year prior to the introduction of deflazacort, p < 0.001). The prednisolone dose or equivalent dose of deflazacort at relapse was 0.17mg/kg/day vs. 0.16mg/kg/day, respectively (p = 0.026). There were no statistically significant differences with respect to the height, weight and BMI SDS of the patients between the two periods (Table I).
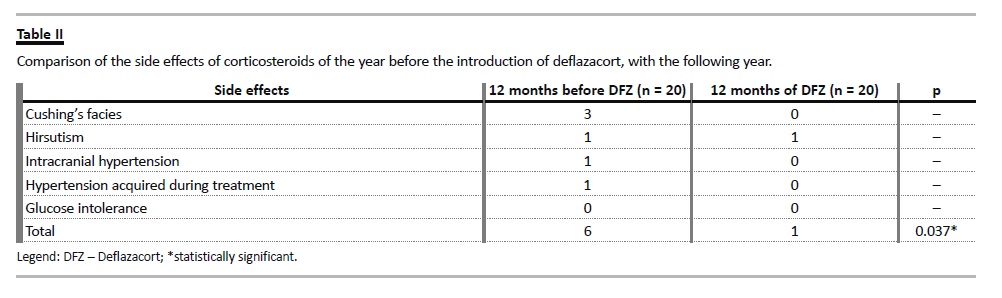
Regarding side effects of steroids, they were, in total, statistically less frequent during the year of therapy with deflazacort than with prednisolone (p = 0.037) (Table II).
There were no statistically significant differences in the remaining variables.
DISCUSSION
This is the first study conducted in Portugal and one of the few in the literature in children with steroid-dependent INS.
In our study, deflazacort showed to be an effective drug for maintenance therapy in steroiddependent INS, having a high number of children that remained without relapses for one year, as well as a small average number of relapses and a large interval between relapses. Broyer et al.6, in the first prospective study on this topic performed in children, also found that the average recurrences in the group treated with prednisolone was significantly higher than those in the group treated with deflazacort (2.8+/-1.8 versus 0.9+/-1.4) and the number of patients without recurrence was significantly higher in the group treated with deflazacort (60% versus 10%). Nayak et al.8 indicated that an equipotent dose of deflazacort relative to prednisolone inhibits reactivity of T cells for a longer period, and relative to methylprednisolone it has a more potent immunosuppressive activity with a low ratio of CD4+/CD8+ lymphocytes, which may explain its greater efficiency and the longest period without recurrence.
We did not found a statistically significant difference with respect to the period from the start of treatment until a patient reaches the remission (6.9+/-2.9 days with prednisolone versus 7+/-3.5 days with deflazacort), as described in previous studies1,6.
For example, in Broyer et al.6 the mean time for attaining remission when the treatment was started at the time of a new relapse was the same in two groups (8 days) with range in the deflazacort group of 3–24 days and 4–69 days in the prednisolone group.
For side effects of corticosteroid therapy, a much discussed and controversial subject, we found a smaller number in the year of treatment with deflazacort, with fewer symptoms of Cushing, hirsutism, acquired hypertension or intracranial hypertension.
There had been no cases of glucose intolerance during the two years of study. This may be due to the fact that the active metabolite of deflazacort (D-21 OH) has a short half-life and a shorter duration of effect, compared to prednisolone or methylprednisolone8.
The fewer side effects is also supported by previous studies6-9, in particular Broyer et al.6 that, despite not having found statistically significant difference, described that symptoms of Cushing and osteopenia were less marked with deflazacort. Nayak et al.8 described a smaller decline in bone mineralization with deflazacort, with less likelihood of corticosteroid induced osteoporosis, because deflazacort causes less depression of osteoblasts and intestinal calcium absorption. Also Olgaard et al.10 showed a smaller loss of bone mass in patients treated with deflazacort (forearm: 2.0%/year versus 5.3%/year; lumbar spine 6.8%/year versus 12.5% /year). Joshi et al.9 relates that osteoprotegerin (OPG) and receptor activator of NF-KB ligand (RANKL) are osteoblast-derived proteins, responsible for inhibition and stimulation of bone resorption respectively, and that the adult population studies have shown a favourable ratio of serum RANKL / OPG with deflazacort, which means less bone mass loss. Several other studies show contradictory conclusions regarding these and other side effects of these drugs1,4,6,8,10. Also we have to take into account that because the patients in our study had fewer relapses in the period of deflazacort, the total dose of corticosteroid administered was smaller, which may also justify fewer side effects.
Another important point relates to the stat-weight growth of children who undergo prolonged treatment with corticosteroids. In our study we found no statistically significant differences in weight, height or BMI SDS when comparing the two drugs. The average SDS height was slightly bigger in the deflazacort treatment period (0.23+/-0.81 versus 0.21+/-0.77), which may mean that over a longer follow-up, we could draw more statistically relevant conclusions. Likewise, Joshi et al.9 indicate that the deflazacort has been associated with a minor reduction in growth rate and greater height after one or two years of therapy. Broyer et al.6, as in our study, did not show statistical differences between the two drugs, but found that there was a more pronounced weight gain in the group treated with prednisolone (3.9+/-4.1Kg versus 1.7+/-2.8Kg). Rather, Olgaard et al.10 found a statistically significant difference, with a more significant weight increase observed in the prednisolone group at 6 and 12 months of treatment and a decrease in the deflazacort group.
Regarding the suppression of adrenal gland, Joshi et al.9 suggests that deflazacort needs a higher dose than prednisolone to cause the suppression, since it has effect only within the pituitary but prednisolone has an effect on both pituitary and adrenal glands. However, Nayak et al.8 states that deflazacort, because its binding to plasma proteins and blood cells, reaches a low concentration in the hypothalamic-pituitary circulation during the first years of treatment.
This studys main limitations are being a retrospective study of clinical data collected from records of patients, with a small sample of patients and a treatment period of only one year with deflazacort. Furthermore, it is known that the natural course of INS includes a decrease in the number of relapses, so that, the best performance of deflazacort relative to prednisolone can be partly explained by this expected favourable course. However, in our study, the difference between the two treatments was only one year and we studied patients with steroid-dependent INS with multiple relapses until the introduction of deflazacort, with a drastic reduction of these with this drug.
As advantages, the authors aim to highlight that this is a study of the same group of patients for both drugs, which eliminates several sample stage bias. It is a groundbreaking study, which intends to draw attention to the benefits of this drug in order to be a starting point for conducting more comprehensive studies.
CONCLUSION
In this sample and in a short period of treatment, deflazacort was associated with a small number of relapses and side effects compared to prednisolone.
There was no significant impact on the stat-weight growth. In this sample, the deflazacort proved to be a safe and effective therapy in child INS maintenance treatment and it should be considered an alternative before including other immunosuppressants.
References
1. Jat KR, Khairwa A. Deflazacort in comparison to other steroids for nephrotic syndrome. Indian J Nephrol 2012;22(4):239-245. [ Links ]
2. Hodson EM, Craig JC, Willis NS. Evidence-based management of steroid-sensitive nephrotic syndrome. Pediatr Nephrol 2005;20(11):1523-1530. [ Links ]
3. Gipson DS, Massengill SF, Yao L, et al. Management of childhood onset nephrotic syndrome. Pediatrics 2009;124(2):747-757. [ Links ]
4. Filler G. Treatment of nephrotic syndrome in children and controlled trials. Nephrol Dial Transplant 2003;18 [Suppl 6]: vi75-vi78. [ Links ]
5. Hodson EM, Knight JF, Willis NS, Craig JC. Corticosteroid therapy in nephrotic syndrome: a meta-analysis of randomised controlled trials. Arch Dis Child 2000;83(1):45-51. [ Links ]
6. Broyer M, Terzi F, Lehnert A, Gagnadoux MF, Guest G, Niaudet P. A controlled study of deflazacort in the treatment of idiopathic nephrotic syndrome. Pediatr Nephrol 1997;11(4):418-422. [ Links ]
7. Tandon VR, Singh P, Mahajan A. Comparative adverse drug profile of deflazacort vs. conventional corticosteroids in spontaneous reporting system of pharmacovigilance. JK Science 2014;16(1):16-20. [ Links ]
8. Nayak S, Acharjya B. Deflazacort versus other glucocorticoids: a comparison. Indian J Dermatol 2008;53(4):167-170. [ Links ]
9. Joshi N, Rajeshwari K. Deflazacort. J Postgrad Med 2009;55(4):296-300. [ Links ]
10. Olgaard K, Storm T, Wowern N, et al. Glucocorticoid-induced osteoporosis in the lumbar spine, forearm, and mandible of nephrotic patients: a double-blind study on the high-dose, long-term effects of prednisone versus deflazacort. Calcif Tissue Int 1992;50(6):490-497. [ Links ]
Drª Catarina Isabel Madeira Rodrigues Neves
Paediatric Nephrology Unit, Hospital Pediátrico de Coimbra, Centro Hospitalar e universitário de Coimbra, EPE,
Avenida Afonso Romão-Alto da Baleia, 3000-602 Coimbra, Portugal.
E-mail: catarinarneves@hotmail.com
Disclosure of Potential Conflicts of Interest: None declared.
Received for publication: 03/08/2015
Accepted in revised form: 07/11/2015


{kind=link}
{kind=link}