










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
Print version ISSN 0872-0169
Port J Nephrol Hypert vol.30 no.3 Lisboa Sept. 2016
ORIGINAL ARTICLE
Serum levels of TNF-α, IL-6 and IL-10 in haemodialysis and renal transplant patients and in healthy subjects
Nasar Yousuf Alwahaibi1, Halima Khalfan Alissaei1, Sara Abdullah Alshihi1, Nadia Alabri2, Samya Sulaiman Albalushi2, Mohammed Albalooshi3
1 Department of Allied Health Science
2 Departament of Pathology
3 Department of Microbiology and Immunology
College of Medicine and Health Sciences
Sultan Qaboos University, Sultanate of Oman
ABSTRACT
Background: Inflammatory processes seem to play an important role in the development of atherosclerosis. Recurrent or chronic inflammatory processes are common in individuals with end‑stage renal disease. There isno consensus approach to assess the degree of severity of inflammation in individuals with kidney disease. In recent years, there has been a growing interest in the role of various cytokines in chronic kidney disease (CKD). Cytokines such as tumor necrosis factor‑alpha (TNF‑α) and interleukin 6 (IL‑6) are mediators of inflammation that may play an important role in CKD. Interleukin 10 (IL‑10) is a regulatory cytokine that seems to play a role in limiting inflammatory processes. Aim: The aim of this study was to evaluate the serum levels of TNF‑ α, IL‑6 and IL‑10 in a population of haemodialysis and renal transplant patients and in healthy subjects. Methods: This was a cross‑sectional study. In 152 participants inflammation was assessed by measuring TNF‑α, IL‑6 and IL‑10. The study included 53 haemodialysis patients, 45 renal transplant patients and 54 healthy subjects. Results: Serum levels of TNF‑α were significantly higher in haemodialysis and renal transplant patients than in healthy subjects (40.2±10.8 vs 5.2±1.7 pg/mL; p<0.05; and 16.1±5.9 vs 5.2±1.7 pg/mL; p<0.05, respectively). Serum levels of IL‑6 were significantly higher in haemodialysis patients than in healthy subjects (40.2±41.4 vs 16.4±5.4 pg/mL; p<0.05), whereas no significant difference was found between renal transplant patients and healthy subjects (20.1±8.3 vs 16.4±5.4 pg/mL; p=NS). Serum levels of IL‑10 were significantly higher in haemodialysis and renal transplant patients than in healthy subjects (23.8±4.5 vs 10.5±3.9 pg/mL; p<0.05; and 19.4±3.1 vs 10.5±3.9 pg/mL; p<0.05, respectively). Conclusion: This study showed higher levels of inflammatory markers (TNF‑α, IL‑6) and of the regulatory cytokine IL‑10 in haemodialysis patients than in healthy controls and higher levels of TNF‑α and IL‑10 in renal transplant patients than in healthy controls. In haemodialysis patients, increased levels of inflammatory markers usually predict a poor outcome.
Keywords: TNF‑α; IL‑6; IL‑10; chronic renal failure; hemodialysis; renal transplant.
INTRODUCTION
Inflammatory processes seem to play an important role in the development of atherosclerosis. Recurrent or chronic inflammatory processes are common in individuals with end‑stage renal disease (ESRD). There is no consensus approach to assess the degree of severity of inflammation in individuals with kidney disease. In recent years, there has been a growing interest in the role of various cytokines in chronic kidney disease (CKD). The aim of this study was to evaluate the serum levels of the inflammatory markers TNF‑α and IL‑6, and of the regulatory cytokine IL‑10 (which seems to play a role in limiting inflammatory processes), in a population of haemodialysis and renal transplant patients and in healthy subjects.
METHODS
This was a cross‑sectional study. In 152 participants inflammation was assessed by measuring TNF‑α and IL‑6.
Serum levels of the regulatory cytokine IL‑10 were also measured. The study included 53 haemodialysis patients (pre‑and post‑dialysis samples), 45 renal transplant patients and 54 healthy subjects. Haemodialysis patients were dialysed for three to four hours, two to three times weekly on Braun‑dialysis machine (B. Braun Medical Inc. Michigan, USA), using biocompatible polysulfone membranes. Patients who had infectious diseases were excluded from the study. Blood samples (5 ml) were collected in plain tubes. The samples were centrifuged at a speed of 3000 rpm at 40C for 10 minutes to separate the serum from the blood cells.
Then the serum was pipetted and stored at ‑800C till use. Serum levels of TNF‑α, IL‑6 and IL‑10 were measured by enzyme‑linked immunosorbent assay (ELISA). Kits were obtained from R&D Systems Europe (Abingdon, UK). The manufacturers instructions were followed.
Ethical approval was obtained from the Medical Research Committee and Ethics Committee from Sultan Qaboos University, College of Medicine and Health Sciences (MREC# 538). All participants gave their written informed consent.
Statistical analysis was performed using SPSS (version 19.0) statistical package (SPSS Inc., Chicago, IL, USA). The numerical variables are presented as mean ± standard deviation. For data that do not follow a normal distribution, Mann‑Whitney U‑test and Wilcoxon signed‑rank test (for paired difference between pre‑dialysis and post‑dialysis) were used for comparison and P< 0.05 was considered significant.
RESULTS
The haemodialysis group consisted of 53 patients, 25 females and 28 males, with a mean age of 51.0±13.6 years. The renal transplant group consisted of 45 patients, 14 females and 31 males, with a mean age of 41.1±13.0 years, and included 27 stable transplants (60%) and 18 renal biopsy‑proven rejections (40%), of which five were acute and 13 chronic rejections. The healthy control group consisted of 54 subjects, 22 females and 32 males, with a mean age of 40.7±7.0 years.
Levels of TNF‑α, IL‑6 and IL‑10 cytokines were measured and the mean concentration ± standard deviation was presented.
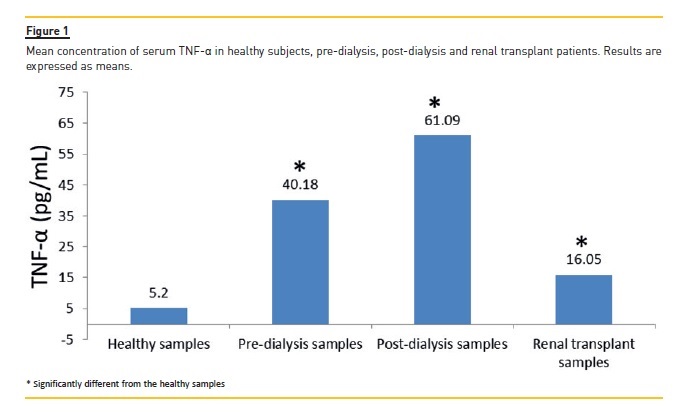
In the haemodialysis population, the mean concentration of TNF‑α was not significantly different in post‑dialysis samples when compared to pre‑dialysis samples.
TNF‑α mean concentration was significantly higher in haemodialysis and renal transplant patients when compared to the healthy subjects (40.2±10.8 vs 5.2±1.7 pg/mL; p<0.05; and 16.1±5.9 vs 5.2±1.7 pg/mL; p<0.05, respectively). (Figure 1).
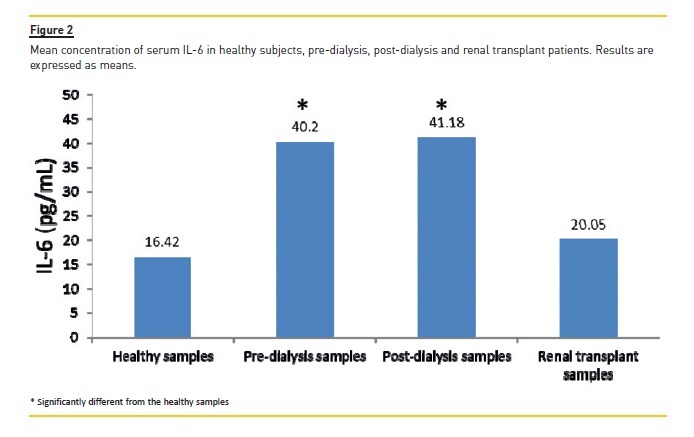
The mean concentration of serum IL‑6 was significantly higher in haemodialysis patients when compared to the healthy subjects (40.2±41.4 vs 16.4±5.4 pg/mL; p<0.05). No significant difference was seen between pre‑and post‑dialysis samples or between renal transplant patients and healthy subjects (Figure 2).
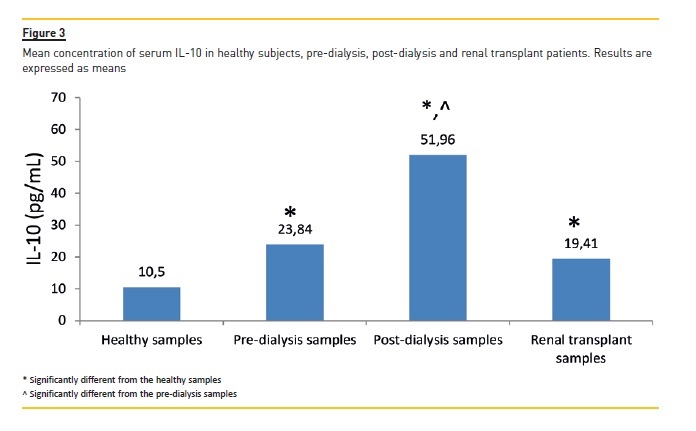
For IL‑10 level, there was a significant difference in the mean concentration of IL‑10 between pre and post‑dialysis samples (p< 0.05). Also the mean concentration of IL‑10 was significantly higher in hemodialysis and renal transplant patients when compared to healthy subjects (23.8±4.5 vs 10.5±3.9 pg/mL; p<0.05; and 19.4±3.1 vs 10.5±3.9 pg/mL; p<0.05, respectively) (Figure 3).
DISCUSSION
The findings of this study show significant elevated levels of TNF‑α, IL‑6 and IL‑10 in haemodialysis patients as compared with healthy subjects.
IL‑10 is an anti‑inflammatory cytokine which is very important in patients with ESRD. Elevated levels of IL‑10 were reported by several studies1,2. It is believed that higher levels of IL‑10 are needed in ESRD patients, in comparison with healthy subjects, to limit their strong inflammatory activation. Chronic inflammation is a common feature of ESRD which carries a heightened risk of atherosclerosis and other co‑morbid conditions3‑5.
IL‑10 is a regulatory cytokine that limits inflammatory processes by down‑regulating the production of monocyte‑derived cytokines5. The elevation of IL‑10 observed in dialysis patients seems to be a counter‑regulatory mechanism to control chronic inflammation associated with uraemia and the dialysis technique5,6.
In this study IL‑10 levels were significantly higher in dialysis and transplant patients than in healthy subjects, and levels tended to increase during the dialysis sessions.
The findings of elevated concentrations of TNF‑α in haemodialysis and renal transplant patients are in line with some earlier studies7‑9.
However, this has not been consistent finding as Powell et al in a study published recently found that the concentration of serum TNF‑α in dialysis and chronic renal failure patients were not higher than in healthy subjects10. Also, the increase in serum TNF‑α, observed during the haemodialysis session, was also shown by Bukan et al who also measured the concentration of serum TNF‑α before and after dialysis and reported similar findings11.
If confirmed by subsequent studies, the elevated levels of TNF‑α in haemodialysis and renal transplant patients could be due to uraemia as impaired renal function may be one of the major factors associated with increased serum levels of TNF‑α12.
Insulin resistance, volume overload and obesity have been also proposed as important causes of elevated TNF‑α levels in haemodialysis and renal transplant patients13.
It has been suggested that T‑helper and T‑regulatory cells are important in haemodialysis patients. T‑helper cells are the major cells for expressing different cytokines. There are two types of T‑helper cells, Th1 and Th2. Th1 cells produce many pro‑inflammatory cytokines, including TNF‑α, whereas Th2 cells produce also several pro‑inflammatory cytokines, including IL‑6.
On the other hand, T‑regulatory cells produce anti‑inflammatory cytokines, including IL‑10.
T‑regulatory cells down‑regulate both Th1 and Th2 responses. Thus it has been suggested that the control of Th1 (TNF‑α) and Th2 (IL‑6) by T‑regulatory cell (IL‑10) is important in monitoring inflammation in haemodialysis patients14.
In this study, serum levels of IL‑6 were significantly higher in haemodialysis patients than in healthy subjects, whereas no significant difference was found between renal transplant patients and healthy subjects.
The latter could be due to improvement of health status and renal function as most patients with a kidney transplant did not show kidney transplant rejection. During the dialysis sessions no change in IL‑6 levels was observed. A number of studies have shown that haemodialysis and renal transplant patients usually havehigh IL‑6 serum levels15‑18.
The causes of elevated IL‑6 concentration in haemodialysis and renal transplant patients could be due to uremia, genetic factors such as single nucleotide polymorphisms, persistent infections such as Chlamydia pneumoniae, oxidative stress, volume overload, obesity and old age13. Other dialysis‑related factors may include the use of bioincompatible membranes, nonsterile dialysate and backfiltration19.
Several studies reported an increase in serum IL‑6 concentrations during haemodialysis sessions16‑18.
Additionally, it has been reported that high serum levels of IL‑6 in haemodialysis or renal transplant patients is a strong predictor of poor outcome or disease severity16,20,21.
Several limitations of our study are worth noting. First, dialysis session length ranged from 180 to 240 minutes and this variable session length may have influenced cytokine levels in the haemodialysis population.
Second, the renal transplant group included in this study was a heterogeneous population, including both stable patients and patients with acute and chronic allograft rejection. It is, therefore, not possible to assess the relative impact of each of these conditions on the serum levels of cytokines. The rejection process, being an inflammatory process, may in fact increase several pro‑inflammatory cytokines. Third, serum levels of C‑reactive protein (CRP) were not measured. CRP is reported to be a marker for cardiovascular disease and inflammation22. Fourth, due to the small sample size, and the possibility of sampling error, the results of this study should be interpreted with caution.
References
1. Girndt M, Köhler H, Schiedhelm‑Weick E, Schlaak JF, Meyer zum Büschenfelde KH, Fleischer B. Production of interleukin‑6, tumor necrosis factor alpha and interleukin‑10 in vitro correlates with the clinical immune defect in chronic hemodialysis patients. Kidney Int 1995; 47:559‑565. [ Links ]
2. Morita Y, Yamamura M, Kashihara N, Makino H. Increased production of interleukin‑10 and inflammatory cytokines in blood monocytes of hemodialysis patients. Res Commun Mol Pathol Pharmacol 1997; 98:19‑33. [ Links ]
3. Tarakçioglu M, Erbagci A, Usalan C, Deveci R, Kocabas R. Acute effect of hemodialysis on serum levels of proinflammatory cytokines. Mediators Inflamm 2003; 12:15‑19. [ Links ]
4. Rysz J, Banach M, Ciałkowska‑Rysz A, Stolarek R, Drozdz J, Okonski P. Blood serum levels of IL‑2, IL‑6, IL‑8, TNF‑α and IL‑1β in patients on maintenance hemodialysis. Cell Mol Immunol 2006; 3:151‑154. [ Links ]
5. Girndt M, Kaul H, Sester U, et al. Anti‑inflammatory interleukin‑10 genotype protects dialysis patients from cardiovascular events. Kidney Int 2002; 62:949‑955. [ Links ]
6. Girndt M, Ulrich C, Kaul H, Sester U, Sester M, Kohler H. Uremia‑associated Immune defect: the IL‑10‑CRP axis. Kidney Int 2003; 63:S76‑S79. [ Links ]
7. Sonkar GK, Usha, Singh R G. Evaluation of serum tumor necrosis factor α and its correlation with histology in chronic kidney disease, stable renal transplant and rejection cases. Saudi J Kidney Dis Transpl 2009; 20:1000‑1004. [ Links ]
8. Ficek R, Kokot F, Chudek J, Adamczak M, Ficek J, Andrzej W. Plasma concentration of tumor necrosis factor alpha may predict the outcome of patients with acute renal failure. Kidney Blood Press Res 2006; 29:203‑209. [ Links ]
9. Cottone S, Palermo A, Vaccaro F, et al. Inflammation and endothelial activation are linked to renal function in long term kidney transplantation. Transplant Int 2007; 20:82‑87. [ Links ]
10. Powell AC, Bland LA, Oettinger CW, et al. Lack of plasma interleukin‑1 beta or tumor necrosis factor‑alpha elevation during unfavorable hemodialysis conditions. J Am Soc Nephrol 1991; 2:1007‑1013. [ Links ]
11. Bukan N, Sancak B, Pasaoglu H, Elbeg S, Unal A, Erten Y. Serum homocysteine, lipoprotein (a), tumor necrosis factor‑alpha, total cholesterol and triglyceride levels in haemodialysis patients. Turkiye Klinikleri J Med Sci 2004; 24:435‑439. [ Links ]
12. Nakanishi I, Moutabarrik A, Okada N, et al. Interleukin‑8 in chronic renal failure and dialysis patients. Nephrol Dial Transplant 1994; 9:1435‑1442. [ Links ]
13. Stevinkel P, Ketteles M, Johnson R, et al. IL‑10, IL‑6, and TNF‑alpha: central factors in the altered cytokine network of uremia: The good, the bad, and the ugly. Kidney Int 2005; 67:1216‑1233. [ Links ]
14. Caligiuri G, Rudling M, Ollivier V, et al. Interleukin‑10 deficiency increases atherosclerosis, thrombosis, and low‑density lipoproteins in apolipoprotein E knockout mice. Mol Med 2003; 9:10‑17. [ Links ] [ Links ]
16. Pecoits‑Filho R, Lindholm B, Axelsson J, Stenvinkel P. Update on interleukin‑6 and its role in chronic renal failure. Nephrol Dial Transplant 2003; 18:1042‑1045. [ Links ]
17. Amirzargar A, Lessanpezeshki M, Fathi A, et al. Th1/Th2 Cytokine analysis in Iranian renal transplant recipients. Transplant Proc 2005; 37:2985‑2987. [ Links ]
18. Malaponte G, Bevelacqua V, Fatuzzo P, et al. IL‑1beta, TNF‑alpha and IL‑6 release from monocytes in haemodialysis patients in relation to dialytic age. Nephrol Dial transplant. 2002;17:1964‑70. [ Links ]
19. Stenvinkel, P, Alvestrand, P. Inflammation in end‑stage renal disease: Sources, consequences and therapy. Semin Dial 2002; 15:330‑338. [ Links ]
20. Kimmel PL, Phillips TM, Simmens SJ, et al. Immunologic function and survival in hemodialysis patients. Kidney Int 1998; 54:236‑244. [ Links ]
21. Simmons EM, Himmelfarb J, Sezer MT, et al. Plasma cytokine levels predict mortality in patients with acute renal failure. Kidney Int 2004; 65:1357‑1365. [ Links ]
22. Genest J. C‑reactive protein: Risk factor, biomarker and/or therapeutic target? Can J Cardiol 2010; 26 (Suppl) A:A41‑44. [ Links ]
Dr. Nasar Alwahaibi
Department of Allied Health Sciences
College of Medicine and Health Sciences
Sultan Qaboos University
P.O. Box 35 Postal Code 123 Muscat – Oman
Tel: Office: 00968 24141188
Fax: 00968 24413419
E‑mail: nasar@squ.edu.om
Disclosure of Conflicts of Interest: None declared
ACKNOWLEDGEMENTS
This study was supported by a research grant from Sultan Qaboos University, College of Medicine and Health Sciences, Oman. The authors would like to thank all participants and nurses of Dialysis Unite at Sultan Qaboos University Hospital for their help.
Received for publication: Oct 22, 2015
Accepted in revised form: Mar 30, 2016


{kind=link}
{kind=link}
{kind=link}