










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.32 no.4 Lisboa dez. 2018
ORIGINAL ARTICLE
Infective endocarditis in renal transplant recipients: one centers experience
Pereira L1,2, Meng C1,2, Guedes L3, Marques S1,2, Nunes A1,2, Sampaio S1,2, Tavares I1,2, Bustorff M1,2, Pestana M1,2
1 Nephrology Department, São João Hospital Center, Porto, Portugal.
2 Nephrology and Infectious Diseases Group, INEB/I3S, Porto, Portugal.
3 Medicine Department, Entre Douro e Vouga Hospital Center, Santa Maria da Feira, Portugal.
ABSTRACT
Background: Infective endocarditis (IE) is rarely described among renal transplant recipients.
Methods: We conducted a retrospective study to identify all cases of IE in our renal transplant unit between 1992 and 2012 to elucidate IEs clinical features and outcomes. Modified Duke criteria were applied to confirm diagnosis and patient evolution was evaluated.
Results: Between 1992 and 2012, our renal transplant unit performed 1065 renal transplants. Seven episodes of IE were identified in six patients. Median age at presentation was 59 years and most cases occurred in males (71.4%). Blood cultures were negative in 42.9% of patients. Gram positive coccus were the most frequent etiologic agents. There were no fungal endocarditis. Aortic valve was involved in all patients. Three patients underwent cardiac surgery. Mortality at 30 days and 2 years were 16.7%.
Conclusion: Infective endocarditis in renal transplant patients remains a rare disease. The diagnosis is challenging considering nonspecific presentation and the high proportion of negative blood cultures.
Keywords: Infective endocarditis, kidney, transplantation
INTRODUCTION
Infection is the second cause of death among renal transplant recipients with graft function preserved1. In these patients, infective endocarditis (IE) is a rarely described infection with high rates of morbidity and mortality2. It remains an underappreciated infection – Ruttmann et al showed that 33.3% of transplant recipients with IE were diagnosed only at autopsy3.
There is a paucity of published data and, therefore, the clinical features and outcome of IE in this particular group of patients need to be elucidated.
In this study, we report etiologic agents, clinical features, treatment and outcome of IE in renal transplant recipients at our center.
PATIENTS AND METHODS
We conducted a retrospective study to identify all cases of IE occurring at the Renal Transplant Unit of the São João Hospital Center from January 1992 to December 2012 using the hospital codification system.
The department registry was also used to ensure that no case was missed. Only cases that met the Duke criteria4 for definite or possible IE were included in thisstudy.
Demographic, clinical, microbiological and outcome data were obtained using clinical records. Data included age, sex, donor source, immunosuppression, time since renal transplantation, clinical presentation, valve involved, etiologic agent, history of rejection, history of valvular heart disease, treatment and outcome at 30 days, 2 years and at the end of follow‑up. Patient evolution was recorded from diagnosis until death, loss of follow‑up or end of study (December 2012).
RESULTS
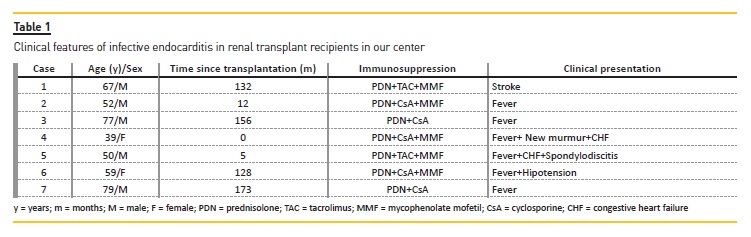
In our long‑term single‑center experience from 1992 to 2012, we found 7 cases of IE in 6 patients. In this period of time, our renal transplant unit performed 1065 renal transplants which corresponds to an IE prevalence of 0.66%. Age, sex, time since transplantation, immunosuppression and clinical presentation are listed in Table 1; involved valve, etiology, treatment and outcome are listed in Table 2.
Median age at presentation was 59 years (range: 39‑79 years) and median time since transplantation was 128 months (range: 0‑173 months). All cases occurred in deceased‑donor renal transplant recipients. There was no history of rejection or previous invasive procedure with risk of bacteremia. Three patients had valvular heart disease – aortic stenosis in 2 cases (cases 3 and 7 in Table 2) and mitral insufficiency in another (case 5 in Table 2).
Fever was the most common clinical presentation and occurred in all but one case. The aortic valve was involved in all patients. In 2 cases, the mitral valve was also affected.
Two patients had embolic events attributed to IE (stroke in one and spondylodiscitis in another). In 42.9% of cases (3 of 7) blood culture results were negative. It was not possible to identify an etiologic agent in spite of further evaluation with serological examinations for infectious by fastidious organisms, namely Coxiella burnetii, Bartonella spp, Legionella spp and Brucella spp. Further, investigators were not able to ascertain prior history of antibiotic treatment.
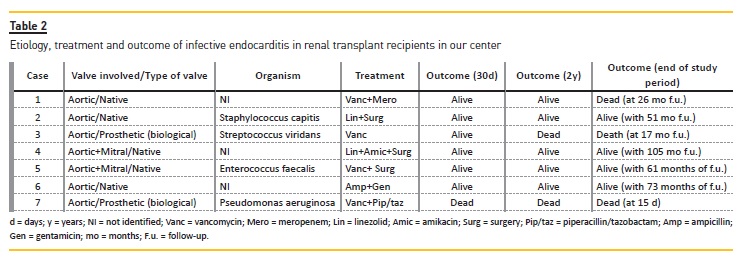
Gram positive coccus were the most frequent etiologic agents – Staphylococcus capitis, Streptococcus viridans and Enterococcus faecalis, one case each. In 1 patient, IE was due to Pseudomonas aeruginosa. In 3 cases transthoracic echocardiogram was negative and subsequent transesophageal echocardiogram revealed echocardiographic findings positive for IE – vegetations in 1 patient (case 1) and abscess in the others (cases 3 and 7). The proportion of negative transthoracic echocardiogram was 42.9% (3 negative results in 7 cases) in our series.
Treatment included antibiotics, and surgery was needed in 3 patients – one patient was submitted to aortic valve replacement; two patients to aortic and mitral valve replacement. Antibiotic treatment duration was 4‑6 weeks.
In one case (case 7), renal allograft function was lost due to sepsis and the patient died with a failed transplant. Of the remaining cases, three had reversible acute allograft dysfunction and three had no allograft dysfunction.
There was one case of recurrent IE (case 7) 17 months after the initial episode (case 3). At 30 days of follow‑up, mortality was 16.7% (1 death in 6 patients). In the long‑term, at 2 years of follow‑up, mortality was 16.7% (1 death in 6 patients). At the end of study period, with a median follow‑up time of 51 months (range: 0.5‑105 months), the cumulative mortality was 33.3% (2 deaths in 6 patients).
The patient referred to as case 1 died 26 months after IE episode due to trauma and so not directly clinically related to IE.
DISCUSSION
Infective endocarditis in renal transplant recipients may be difficult to diagnose. In these patients, clinical features of IE remain to be elucidated. The classic manifestations of IE such as new murmur and splenomegaly are usually not seen5,6. Fever may be lacking or it can be attributed to causes other than IE5,6. However, in our study, 85.7% of cases (6 of 7 cases) had fever on presentation. Also, the most recent published series of renal transplant recipients with IE demonstrated that fever occurred in 100% of patients7. Infective endocarditis should be considered in renal transplant recipients with fever without other obvious cause.
As a recent case report helps to highlight8, we have to keep in mind that vascular access for hemodialysis (including nonfunctioning arteriovenous grafts) should be considered as the possible origin of the infection.
Fluorodeoxyglucose‑positron emission tomography/computed tomography (FDG‑PET/CT) scan is useful for the identification of extra‑cardiac infection sites in patients with IE.
The most common cause of IE in renal transplant recipients remains to be clarified. In previous studies, Staphylococcus aureus2,3 and Streptococcus spp9 were the most frequent etiology. However, in Farahani´s series, the most frequent cultured organism was Enterococcus spp and it was responsible for 31% of cases7. In our series, we couldn´t identify a most frequent agent.
The causative organisms were Staphylococcus capitis, Streptococcus viridans, Enterococcus faecalis and Pseudomonas aeruginosa, one case each. To our knowledge, endocarditis due to Staphylococcus capitis has not yet been reported in renal transplant recipients.
Fungal endocarditis is considered more frequent in solid organ transplant recipients than in the general population. Former series showed a prevalence of fungal endocarditis varying between 14.8%3 and 28%2 in these immunosuppressed patients while in the general population fungal endocarditis is rare and corresponds to only 2% of cases10. However, in our series, there was no endocarditis due to fungal infection. It is unlikely that we missed a fungal endocarditis because our patients responded well to antibiotic treatment without antifungal therapy. This absence of fungal endocarditis in our series could be explained by a very small number of patients with IE in the first 30 days after transplantation.
Paterson and colleagues showed that in solid organ transplant recipients with IE, fungal infections predominated within 30 days of transplantation, while bacterial infection caused most cases after this time2. Farahani´s series also showed no cases of fungal endocarditis7.
As 2 recent studies in this field have not shown any case of fungal endocarditis, we can speculate that modern improved care of renal transplant recipients, with a tighter surveillance of patients and avoidance of excessive immunosuppression, is responsible for this lack of fungal endocarditis in two series of this decade.
Also, in our series, transplant recipients had no history of rejection and the consequent higher degree of immunosuppression.
In the general population, blood‑culture negative infective endocarditis (BCNIE) occurs in 2.5‑31% of all cases of IE and is due most commonly to prior antibiotic administration11. Another cause of BCNIE is infection by fastidious organisms with limited proliferation under conventional culture conditions or requiring specialized tools for identification. These organisms may be more common in patients with renal failure and immunocompromised states12. In our study, BCNIE was responsible for 42.9% of cases, which might reflect the higher proportion of these organisms in transplant patients, although the retrospective nature of our study did not allow us to exclude prior antibiotic treatment. In renal transplant recipients, BCNIE had been reported in 19‑33% of cases7,9.
In line with Farahani´s findings, the aortic was the most frequent involved valve7. In our series, all patients aortic valves were affected. However the exact degree to which the aortic valve is involved in renal transplant recipients with IE remains to be clarified. Our higher frequency of aortic involvement cannot be explained by preexisting aortic valve disease as only 2 patients had a history of aortic disease. Also, valvular disease has not been conclusively linked as an independent predictor of endocarditis in transplant patients. In a study involving 27 solid organ transplant recipients with IE, only 3 patients had underlying structural valve disease as the predisposing factor3. In line with Paterson and Ruttmann2,3 we think that a history of valve disease may be a less relevant factor in the immunocompromised transplant patients compared with the general population.
Interestingly, there was no case of mural endocarditis, which probably reflects the absence of fungal endocarditis in our series. In the Paterson series of 46 solid organ transplant recipients with IE, of the 8 cases caused by Aspergillus, only one had valve involvement; the remaining fungal infections affected the mural endocardium rather than the valvular endocardium2.
Infective endocarditis is known to be more frequent in men than women12‑14.
The male:female ratio is ≥ 2:1 in all epidemiological studies12. Similarly, in our study, there were 5 cases of IE in male renal transplant recipients but only 2 cases in their female counterparts.
It suggests that the higher risk of IE in males is also present in the transplanted population. It remains to clarify this lower susceptibility of women to develop valve infection, although hormone differences have been suggested13.
The treatment of IE in renal transplant recipients includes administration of appropriate antibiotics and cardiac valve surgery in selected cases15. A high index of suspicion is essential for early diagnosis and adequate antibiotic treatment. There are no specific recommendations for the treatment of IE in this particular group of patients. Until we have studies specifically designed to evaluate the treatment of IE in renal transplant recipients, we suggest following the recommendations for the general population, keeping in mind the specificities of this group of patients.
The antibiotics dose should be adjusted for the level of renal function and it is necessary to be aware of interactions with immunosuppressive drugs and to avoid nephrotoxic agents. It is also important to monitor blood levels of both antibiotics and immunosuppressive drugs that might help to achieve adequate antibiotic therapeutic levels and at same time avoid the risks of excessive or inadequate immunosuppression. Limited data are available regarding the mortality of renal transplant recipients with IE in recent years.
The mortality of IE in renal transplant recipients has been reported to be 16‑41% in hospital7,9 and 42.2% at 2 years9. In our study, mortality at 30 days and at 2 years was 16.7%. This lower mortality in our study could be due to an aggressive diagnostic and therapeutic approach to patients with fever or other symptoms or signs compatible with IE (including blood cultures, transthoracic echocardiogram and transesophageal echocardiogram in selected cases, immediate large‑spectrum antibiotherapy) along with awareness that IE is a rarely described but feared complication in renal transplantation. It is worth noting that in solid organ transplant recipients, 33.3% to 58% of patients were diagnosed only at autopsy2,3. Also in our series the only death reported at 30 days and 2 years refers to the oldest patient (a 79‑year‑old man), with prosthetic aortic valve. In the general population, older age and prosthetic valve IE are known predictors of poor outcomes in IE12. The mortality and its risk factors of IE in renal transplant recipients can only be elucidated by prospective studies specifically designed to answer this question.
Solid organ transplant recipients have a 171‑fold risk of IE compared to the general population and the differences in organ‑specific incidence are not statistically significant3. There are many suggested risk factors3,5,9,16: immunosuppression, frequent hospitalization, invasive procedures, uremia, time in renal replacement therapy before transplantation, hospitalization due to valvular heart disease, donor age, patient age and diabetes. In our series, all cases of IE occurred in patients that were on calcineurin inhibitor as immunosuppressor – 5 on cyclosporine and 2 on tacrolimus. We believe that this seeming association with cyclosporine is only a reflection of our units immunosuppression protocol during a given period. As our study helps to highlight, there are many questions to answer. Risk factors, clinical features, mortality and predictors of outcome remain to be clarified. Keeping that in mind and given the scarcity of published cases of IE in renal transplant recipients as well as the retrospective nature of all studies, the authors suggest an international, multicenter prospective study, perhaps endorsed by an international recognized society in the field of transplantation, to elucidate the characteristics of IE in renal transplant patients. At the very least, it could augment awareness of this potentially fatal disease in this particular group of patients.
The limitations of this study should be noted. The number of renal transplant patients with IE was small. It is a retrospective study that shows the clinical results of IE in just one transplant center.
In conclusion, IE in renal transplant patients is a serious, potentially fatal disease. Its clinical features remain to be elucidated. It should be suspected in renal transplant recipients with fever without other obvious cause. The prognosis is poor and greater awareness of this condition is necessary.
References
1. Kahwaji J, Bunnapradist S, Hsu JW, Idroos ML, Dudek R. Cause of death with graft function among renal transplant recipients in an integrated healthcare system. Transplantation 2011; 91(2): 225‑230. [ Links ]
2. Paterson DL, Dominguez EA, Chang F, Snydman DR, Singh N. Infective endocarditis in solid organ transplant recipients. Clin Infect Dis 1998; 26: 689‑694. [ Links ]
3. Ruttmann E, Bonatti H, Legit C, et al. Severe endocarditis in transplant recipients – an epidemiologic study. Transpl Int 2005; 18: 690‑696. [ Links ]
4. Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 2000; 30(4): 633‑638. [ Links ]
5. Bishara J, Robenshtok E, Weinberger M, Yeshurun M, Sagie A, Pitlik S. Infective endocarditis in renal transplant recipients. Transpl Infect Dis 1999; 1: 138‑143. [ Links ]
6. D´Cunha PT, Davenport DS, Fisher KA. Successful treatment of Staphylococcus aureus bacterial endocarditis in a renal transplant recipient. Transpl Infect Dis 2003; 5: 144‑146. [ Links ]
7. Farahani MM, Rostami Z, Einollahi B, et al. Infective endocarditis after renal transplantation. Nephro Urol Mon 2014; 6(1): e12326. [ Links ]
8. Agmon NI, Goldberg E, Cohen E, Krause I. Infective endocarditis in the setting of renal transplantation: case report and review of literature. Transpl Infec Dis 2017; 19 (6): e12786. [ Links ]
9. Shroff G, Skeans M, Herzog CA. Outcomes of renal transplant and waiting list patients with bacterial endocarditis in the United States. Nephrol Dial Transplant 2008; 23: 2381‑2385. [ Links ]
10. Murdoch DR, Corey R, Hoen B, et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century. Arch Intern Med 2009; 169(5): 463‑473. [ Links ]
11. Katsouli A, Massad MG. Current issues in the diagnosis and management of blood culture‑negative infective and non‑infective endocarditis. Ann Thorac Surg 2013; 95: 1467‑1474. [ Links ]
12. Habib G, Hoen B, Tornos P, et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the task force on the prevention, diagnosis, and treatment of infective endocarditis of the european society of cardiology (ESC). Endorsed by the European society of clinical microbiology and infectious diseases (ESCMID) and the international society of chemotherapy (ISC) for infection and cancer. Eur Heart J 2009; 30(19): 2369‑2413. [ Links ]
13. Castillo JC, Anguita MP, Delgado M, et al. Clinical characteristics and prognosis of infective endocarditis in women. Rev Esp Cardiol 2008; 61(1): 36‑40. [ Links ]
14. Van der Meer JT, Thompson J, Valkenburg HA, Michel MF. Epidemiology of bacterial endocarditis in The Netherlands. I. Patient characteristics. Arch Intern Med 1992; 152(9): 1863‑1868. [ Links ]
15. Ireland JHE, McCarthy JT. Infective endocarditis in patients with kidney failure: chronic dialysis and kidney transplant. Curr Infect Dis Rep 2003; 5: 293‑299. [ Links ]
16. Abbott KC, Duran M, Hypolite I, Ko CW, Jones CA, Agodoa LY. Hospitalizations for bacterial endocarditis after renal transplantation in the United States. J Nephrol 2001; 14(5): 353‑360. [ Links ]
Correspondence to:
Luciano Artur Lopes Pereira;
Nephrology Department, São João Hospital Center, Alameda Prof.Hernani Monteiro, 4200‑319 Porto.
E‑mail: lucianoarturpereira@hotmail.com
Disclosure of potential conflicts of interest: none declared.
Received for publication: Jul 22, 2018
Accepted in revised form: Oct 31, 2018


{kind=link}
{kind=link}