











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Choosing the best therapeutic option for elderly patients with stage 5 chronic kidney disease (CKD) is challenging. In addition to the patient’s wishes, the age, comorbidities, cognitive status, and dependence on daily activities may influence decision-making. Both dialysis and conservative medical treatment may be appropriate, but it is not always clear which one will be most suitable for the patient and will contribute to a better quality of life and symptom relief.
Several scales help to quantify the symptoms and the quality of life experienced by the patient. Integrated Palliative care Outcome Scalerenal (IPOS-renal) is a short survey, validated for renal patients, which quantifies the most common symptoms patients experience. It shows good content and constructs validity, reliability, and responsiveness to change.1 The 5-level EuroQol-5 Dimension (EQ-5D-5L) is a descriptive system that comprises five dimensions of quality of life indicated by the patient: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. In a systematic review of 12 cohort studies, the median survival was 13 months lower for patients undergoing conservative care comparing to dialysis patients.2 However, the survival advantage of dialysis disappears in patients over 75 years of age, who have a high comorbidity burden and/or poor functional status.3,4
We report the case of an 81-year-old woman who initially chose conservative kidney management (CKM) but later accepted to start hemodialysis due to difficult control of fluid overload. During the period on dialysis, she had several complications, the most serious related to lower limb amputation, as a result of severe chronic ischemia.
CASE REPORT
An 81-year-old Caucasian female, who lived independently at home with her husband, had stage 5 CKD, secondary to diabetic kidney disease. Her main comorbidities were long-standing insulintreated diabetes mellitus with associated diabetic retinopathy, peripheral arterial disease, dyslipidemia, arterial hypertension, and osteoarthrosis with difficult pain control (Charlson comorbidity index: 9). She was properly informed about the therapeutic options for stage 5 CKD and consciously opted for conservative care. CKM was initiated in January 2020 (serum creatinine: 5 mg/dL; glomerular filtration rate estimated by the Chronic Kidney Disease Epidemiology
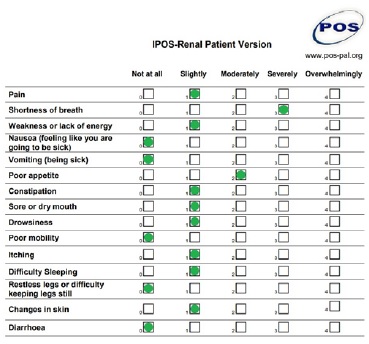
Collaboration equation: 10 mL/min/1.73 m2), and, during the follow-up period, the most disturbing symptoms she experienced were anorexia and fatigue, evaluated by the IPOS-renal scale (Fig. 1), and her Karnofsky Scale score was 80%. The Karnofsky Performance Scale Index classifies the patient’s functional impairment and assesses prognosis. A lower score indicates lower survival probability for most serious illnesses.5
In August 2021, she was admitted to the hospital twice due to acute pulmonary edema, however volume control was not achieved despite increasing diuretic doses. In this context, alternatives were presented: she could be transferred to an hospice to manage symptoms without dialysis, using opioids or even palliative sedation, or a dialysis trial could be done. Although her initial choice for CKM was based on her desire to privilege quality over quantity of life, the family circumstances, namely her husband’s dependence on her, weighed on the decision to have more time to live. Peritoneal dialysis (PD) or assisted PD had already been proposed in the past, but the patient neither wanted to do her treatments daily nor increase the burden on her family. She kept this decision, but accepted to try hemodialysis (HD) and hypervolemia became controlled. After a 3-month dialysis trial, congestive symptoms improved and she agreed to continue on HD. She was transferred to an outpatient dialysis clinic where she currently undergoes treatment through a central venous catheter . Despite improvement in fluid overload, dyspnea, and uremic symptoms, the patient experiences some intradialytic complications, namely hypotension, nausea, and dizziness. She complains of post-dialysis fatigue, requiring bed rest for the rest of the day. Additionally, she developed severe left lower limb ischemia, needing opioids for pain control, which culminated in amputation above-the-knee eight months after starting HD. After the amputation, opioid requirement decreased and she completed two and a half months of rehabilitation.
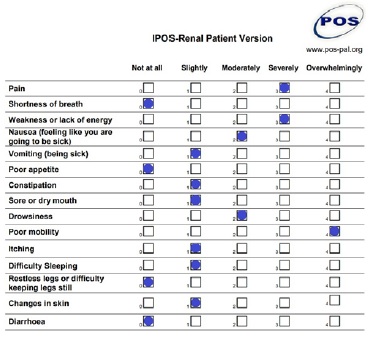
Nevertheless, she became more physically dependent due to poor mobility and currently moves on a wheelchair and needs help for daily living activities.She used to live in 2nd floor apartment without an elevator and needed assistance to get home, so she moved into her daughter´s house. Meanwhile, she got widowed. Although sad, she remains lucid and resilient with an euthymic mood. She is peaceful with the decision of starting dialysis, since it allowed her to have more time to take care of her husband, and to date has not shown the desire to discontinue HD. Currently, 11 months after starting dialysis, her Karnofsky Score is 50%, her Edmonton Frail Scale is 13/17, which represents severe frailty, and the most disturbing symptoms she complains about are weakness, poor mobility, and pain (Fig. 2).
DISCUSSION
Nowadays, patients older than 75 years are the fastest-growing group starting dialysis worldwide.6,7Dialysis may improve quality of life, restore health, and extend life in some patients with CKD, however several studies have reported that, among frail older adults with several comorbidities, the functional status and the level of independence may decrease after dialysis initiation.6,8,9
More than 30% of the elderly over 80 years of age who lived independently at the time of starting dialysis require assistance from the community or from a private caregiver within the first 6 months.8 CKM can be an alternative to dialysis for some patients, especially for those who do not wish to receive maintenance dialysis or would not benefit from it, given their severe comorbidities and clinical conditions. The concept was introduced in some Kidney Units in the United Kingdom in 200310 and is currently a treatment option established in most nephrology departments around the world.7 Conservative care aims to individualize support according to the needs and wishes of each patient, always with a focus on the quality of life and comfort, and is provided by a multidisciplinary team.6,7
Establishing the most suitable therapy for patients with stage 5 CKD, especially the older ones, is challenging. Prognosis estimation is critical in supporting treatment decisions in patients with advanced kidney disease.7,11 Regarding our patient, the estimated 6-month survival on HD was 82.3%, based on the Cohen model, which represents a better survival in dialysis than in CKM. Despite better control of fluid overload, during her time on dialysis, she had several complications. The most significant was severe lower limb ischemia which ended up on amputation and, consequently, on increased dependency in daily living activities. Thus, the predicted better survival did not translate into better quality of life, which in this case was greatly reduced after HD initiation.
Patients on dialysis generally survive longer than those treated conservatively. However, several studies already demonstrated a similar survival in elderly patients with a high burden of comorbidities, regardless of the therapeutic strategy.10,12,13 Patients on CKM tend to be older, but not necessarily with more comorbidities, and usually spend significantly less time in hospital or health care settings, compared to those on dialysis.14 These considerations (time spent in a medical setting; travels to and from dialysis and life expectancy) are important to shared decision-making.10,12,14
Life expectancy and disease trajectory are very heterogeneous among patients of similar ages in the same stage of kidney disease, precluding an accurate prognosis.12,15 Appropriate counseling regarding different treatment options (dialysis vs CKM), based on adequate information and reliable estimation of life expectancy at a given time, is paramount to prevent unrealistic expectations, frustration, and anxiety in patients and their families.7,11,16
Patients want realistic and truthful physicians, who understand their psychosocial needs, provide time for questioning and individualize their prognosis.7 However, the time spent to know the patient as a whole, including family and social circumstances, is limited and many nephrologists are still unaware of the true genesis of CKM, which may hamper suitable and individualized counseling.
Regardless of the treatment strategy chosen, permanent re-evaluation and communication are needed to guarantee that approaches previously defined continue to accomplish the patient’s priorities and needs.12 Many treatment decisions are adapted over time, based on the individual’s experience of disease and its treatment, as well as changing circumstances.12,17
Sometimes, it is uncertain if a given symptom or condition will be better managed conservatively or with dialysis or what kind of experience each patient will have in these different therapeutic strategies. Besides, as demonstrated in this case, the benefits and harms associated with dialysis often change over time, especially after life events or serious complications that may compromise cognitive and functional status.12 The better control of congestive heart failure and improvement of dyspnea was counterbalanced by the worsening of ischemia and consequent amputation, which made her more physically dependent.
In summary, our case reflects the complexity of managing an older stage 5 CKD patient, both on dialysis or CKM, mirroring most of our everyday patients. It would be challenging to control hypervolemia in CKM and would result in an earlier death. However, the complications that occurred during dialysis compromised the patient’s functional status, exacerbating her dependence in daily activities.
Estimating prognosis is always challenging, mainly in the elderly, and treatment decisions may sometimes frustrate physicians and patients. Time is essential to understand the benefits and burdens of different treatment strategies for each patient and the priority should always be optimizing care for older adults with advanced CKD.

