










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkNascer e Crescer
versión impresa ISSN 0872-0754versión On-line ISSN 2183-9417
Nascer e Crescer vol.27 no.3 Porto set. 2018
https://doi.org/10.25753/BirthGrowthMJ.v27.i3.12801
QUAL O SEU DIAGNÓSTICO? | WHAT IS YOUR DIAGNOSIS?
Imaging case
Caso imagiológico
Élcio Roberto DuarteI; Lucas Ribeiro dos SantosIII; Márcio Luís DuarteI,II
I Clínica Radiológica e Especialidades Médicas São Gabriel. 11701-370 São Paulo, Brasil. elcioroberto09@hotmail.com; marcioluisduarte@gmail.com
II WEBIMAGEM. 04104-020 São Paulo, Brasil. marcioluisduarte@gmail.com
III Faculdade de Ciências Médicas de Santos. 11013-330 São Paulo, Brasil. lrs1985@uol.com
ABSTRACT
Inguinal hernias are a common pathology, with an estimated incidence of 20 cases per 1,000 live births, constituting the most common form of hernias of the abdominal wall. This problem affects boys about six times more often than girls.
The canal of Nuck in the female is a protrusion, tubular fold of the peritoneum through the internal inguinal ring, following the round ligament and extending to the labia. The canal of Nuck is patent in up to 90% of newborns, with an increased prevalence in prematures and a tendency to spontaneously close over the first year of life.
We report a case of a six-year-old girl with an ovary containing canal of Nuck hernia diagnosed by ultrasonography. According to the present literature, there are less than twenty ultrasonographic published studies which report ovary containing canal of Nuck hernias.
Keywords: Color doppler; Hernia; Inguinal/diagnostic imaging; Ovarian Diseases/diagnostic imaging; Ultrasonography
RESUMO
As hérnias inguinais são uma patologia comum, com uma incidência estimada de 20 casos por 1.000 nados-vivos, sendo a forma mais comum de hérnia da parede abdominal. Este problema afecta os rapazes cerca de seis vezes mais do que as raparigas.
O canal de Nuck é uma protrusão tubular do peritoneu no sexo feminino, através do anel inguinal interno, seguindo o ligamento redondo e com extensão até ao lábio vaginal. O canal de Nuck está patente em até 90% dos recém-nascidos, sendo mais prevalentes nos recém-nascidos prematuros e apresentando uma tendência para o seu encerramento espontâneo ao longo do primeiro ano de vida.
Apresentamos um caso de uma menina de 6 anos com uma hérnia do canal de Nuck contendo o ovário, diagnosticada por ecografia. De acordo com a literatura, existem menos de duas dezenas de estudos ecográficos publicados que descrevem o encarceramento ovárico neste tipo de hérnias.
Palavras-chave: Doenças ováricas/diagnóstico por imagem; Ecografia Doppler a Cores; Hernia; Inguinal/diagnóstico por imagem
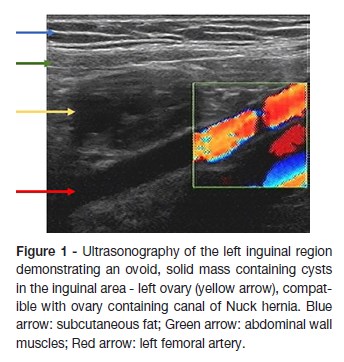
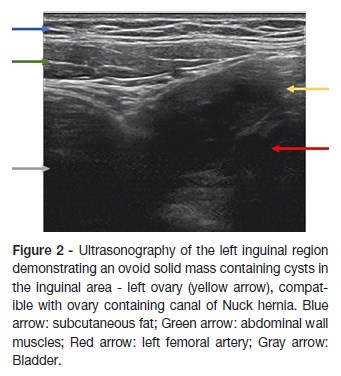
A six-year-old girl who presented at the pediatrician with a complaint of a bulge in the left inguinal region, presenting pain associated with physical activity, for the last eight months, with no improvement after use of analgesic or anti-spasmodic medication. Her physical examination showed a tender but reducible mass in her left inguinal region. Ultrasonography of the left inguinal region detected an inguinal hernia, containing the left ovary (Figures 1 and 2) reporting normal vascularization in the Doppler study. The patient was operated a week later and the follow-up was uneventful.
What is your diagnosis?
DIAGNOSIS
Ovary-containing Hernia of the Canal of Nuck
DIscussion
Inguinal hernias are a common pathology, occurring up to 20 cases per 1.000 live births, especially during the first year of life, representing the most common form of hernias of the abdominal wall. These hernias affects boys about six times more often than girls.1-3
The canal of Nuck in the female is a protrusion, tubular fold of the peritoneum through the internal inguinal ring, following the round ligament and extending to the labia.4 The canal of Nuck is patent in up to 90% of newborns, with a tendency to spontaneously close over the first year of life. The congenital origin of this problem justifies its increased incidence in preterm children.5
All viscera and internal organs herniation can occur through the inguinal canal, but the ovary, specifically, is found in up to 30% of the cases, with its incidence decreasing along with age.1,4,6,7 Constipation, lung disorders, and conditions that raise intra-abdominal pressure, increase the risk of inguinal herniation.8 There are less than 20 ultrasonography (US) descriptions of ovary-containing hernias of the Nuck canal, according to Yang et al.9
The US is an excellent method for the evaluation of superficial regions such as the groin, being very sensitive in superficial structures and must be the first diagnostic method for pediatric patients with abdominal pain and irritability.3,8,9 US has also the possibility of using color Doppler, and may also detect the deficiency of vascularization of the herniated structure, or in the case of the ovary, a torsion - early diagnosis is essential to evaluate gonadal tissue and to preserve fertility.8,9 US should be indicated in female patients with an inguinal hernia containing a palpable movable mass.10
The treatment for this condition is surgical, consisting on ligation of the sac proximally, with its subsequent invagination into the peritoneal cavity through the internal ring, while confirming the reposition of the ovary into the peritoneal cavity.11 Ultrasonography with color Doppler is of great value in establishing the urgency of this procedure. This exam can be particularly useful in defining the blood supply of the ovary, thus evaluating if it is ischemic or not.8,9 This finding can be important in the management of the patient regarding the best surgical approach and the adequate timing of the procedure.
REFERENCES
1. Kapur P, Caty MG, Glick PL. Pediatric hernias and hydroceles. Pediatr Clin North Am. 1998. 45:773-89 [ Links ]
2. Manoharan S, Samarakkody U, Kulkarni M, Blakelock R, Brown S. Evidence-based change of practice in the management of unilateral inguinal hernia. J Pediatr Surg. 2005; 40:1163-6 [ Links ]
3. George EK, Oudesluys-Murphy AM, Madern GC, Cleyndert P, Blomjous JG. Inguinal hernias containing the uterus, fallopian tube, and ovary in premature female infants. J Pediatr. 2000 May;136:696-8. [ Links ]
4. Goldstein IR, Potts WJ. Inguinal hernia in female infants and children. Ann Surg. 1958; 148:819–22. [ Links ]
5. Ando H, Kaneko K, Ito F, Seo T, Ito T. Anatomy of the round ligament in female infants and children with an inguinal hernia. Br J Surg. 1997; 84:404-5. [ Links ]
6. Fowler CL. Sliding indirect hernia containing both ovaries. J Pediatr Surg. 2005; 40:e13–4. [ Links ]
7. George EK, Oudesluys-Murphy AM, Madern GC, Cleyndert P, Blomjous JG. Inguinal hernias containing the uterus, fallopian tube, and ovary in premature female infants. J Pediatr. 2000; 136:696-8. [ Links ]
8. Aydin R, Polat AV, Ozaydin I, Aydin G. Gray-scale and color Doppler ultrasound imaging findings of an ovarian inguinal hernia and torsion of the herniated ovary: a case report. Pediatr Emerg Care. 2013; 29:364-5. [ Links ]
9. Yang DM, Kim HC, Kim SW, Lim SJ, Park SJ, Lim JW. Ultrasonographic diagnosis of ovary-containing hernias of the canal of Nuck. Ultrasonography. 2014; 33:178-83. [ Links ]
10. Huang CS, Luo CC, Chao HC, Chu SM, Yu YJ, Yen JB. The presentation of asymptomatic palpable movable mass in female inguinal hernia. Eur J Pediatr. 2003; 162:493-5. [ Links ]
CORRESPONDENCE TO
Márcio Luís Duarte
Clínica Radiológica e Especialidades Médicas São Gabriel
Rua Mihailo Lukich, 94
Boqueirão, Praia Grande
11701-370 São Paulo
Email: marcioluisduarte@gmail.com
Received for publication: 11.08.2017
Accepted in revised form: 12.02.2018

