










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.28 no.3 Porto set. 2019
https://doi.org/10.25753/BirthGrowthMJ.v28.i3.14575
CASE REPORTS | CASOS CLÍNICOS
Persistent clavicle swelling in the infant
Tumefação persistente da clavícula no lactente
Juliana MacielI, Miguel FriasII, Mariana CapelaIII, Mafalda SantosII
I - Department of Pediatrics, Centro Hospitalar de Leiria. 2410-197 Leiria, Portugal. julianamaciel@live.com
II - Department of Orthopedics, Centro Hospitalar Vila Nova de Gaia/ Espinho. 4400-129, Vila Nova de Gaia, Portugal. miguelcmfrias@gmail.com; mafalda.orto@gmail.com
III - Department of Pediatrics, Centro Hospitalar Vila Nova de Gaia/ Espinho. 4400-129, Vila Nova de Gaia, Portugal. marianacarvalhocapela@gmail.com
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Introduction: Congenital pseudarthrosis of the clavicle is a rare entity of unknown etiology. It is more common in girls and on the right side. Diagnosis is challenging and often performed after the neonatal period, triggered by persistence of a clavicular prominence initially attributed to traumatic birth fracture.
Case Report: Herein is presented the case of a healthy ten-month-old girl with a right clavicle prominence since neonatal period initially attributed to traumatic birth fracture. Radiographic examination of the clavicle revealed congenital pseudarthrosis of the right clavicle.
Comments: One of the most common causes of clavicle swelling in the neonatal period is clavicle fracture due to birth trauma. Clavicular prominence persistence beyond four to six months should raise suspicion of this clinical entity.
Keywords: clavicle; infant; congenital malformation; pseudarthrosis
RESUMO
Introdução: A pseudartrose congénita da clavícula é uma entidade rara e de etiologia desconhecida. Afeta sobretudo crianças do sexo feminino e surge mais frequentemente no lado direito. O diagnóstico é desafiante e frequentemente efetuado após o período neonatal, suscitado por persistência da tumefação clavicular inicialmente atribuída a fratura por traumatismo no parto.
Caso Clínico: É descrito o caso de um lactente do sexo feminino de dez meses de idade, previamente saudável, observado em consulta por persistência de tumefação da clavícula direita identificada no período neonatal e atribuída a fratura da clavícula por traumatismo no parto. Realizou radiografia da clavícula, que foi compatível com pseudartrose congénita da clavícula direita.
Discussão: Uma das principais causas de tumefação clavicular no período neonatal é fratura da clavícula por traumatismo no parto, com consequente formação de calo ósseo. A presença de uma tumefação clavicular indolor e sua persistência após quatro a seis meses deve motivar suspeição da causa mais rara de pseudartrose.
Palavras-chave: clavícula; lactente; malformação congénita; pseudartrose
Introduction
Congenital pseudarthrosis of the clavicle (CPC) is a rare congenital defect first described by Fitzwilliams in 1910.1 Since then, approximately two hundred cases have been reported in the literature, but its exact incidence and prevalence remain unknown.2-5 It is more common in girls and on the right side of the body.2-4,6,10
The condition’s etiology remains unknown, but pathogenesis is related to ossification abnormalities during embryogenesis.2,3,5,7,9,10 Some authors suggest that pressure exerted by pulsation of the subclavian artery over the clavicle, normally located at a higher level on the right side, may cause ossification centers to fail to unite during the development process.2,3,5,6,9 This explains the right-sided predominance of the condition and presence of dextrocardia when CPC develops on the left side. Bilateral involvement is rare and normally associated with presence of cervical ribs, cleidocranial dysostosis, or genetic syndromes, namely Ehler-Danlos, Al-Awadi/ Ras-Rothschild, Kabuki, and Prader-Willi.2,3 Clinical diagnosis is accomplished through observation of a painless prominence in the middle third of the clavicle present at birth, without functional incapacity of the affected upper limb.3,8,10 The deformity tends to become more obvious as the child grows and marked mobility is found at pseudarthrosis site.2,3,10
CPC may be left undiagnosed in the neonatal period due to confusion with clavicular fracture. With a frequency of 15 per 100.000 live births, this is a more common entity, also preferentially manifesting on the right side, but differently from CPC it is usually painful and tends to regress within the first months of life.6
Case report
A ten-month-old girl presented with a painless prominence on the right clavicle, present since the neonatal period and initially attributed to a traumatic birth fracture. It became more obvious as the child grew, but no functional limitation of the upper limb was observed. The girl was born by vaginal delivery, with no obvious traumatic birth history. Anthropometric measurements were appropriate for gestational age and she presented normal growth and development. Family history was unremarkable.
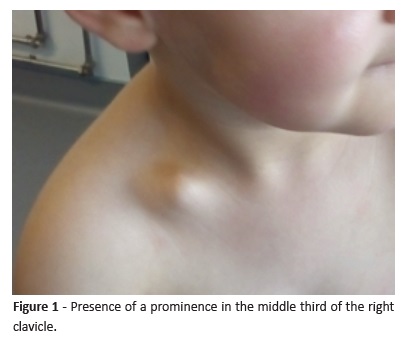
Physical examination revealed a soft mass between the middle and distal third of the right clavicle (Figure 1), with size increasing with abduction of the right arm but causing no pain or functional limitation. No asymmetry with contralateral limb or muscular atrophies were observed. The remaining physical examination was unremarkable.
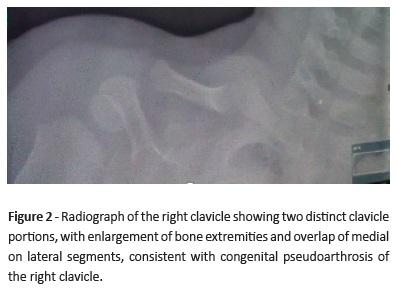
Radiograph of the right clavicle (Figure 2) showed two separate and distinct clavicle portions, with border enlargement and overlap of the medial on lateral segment, consistent with CPC.
Discussion
CPC is a rare entity not properly documented in the literature, making diagnosis challenging.5,6 Because it manifest in newborns, the condition may be mistaken with clavicle fracture, as in the present case.
Differential diagnosis is mainly established due to clavicle fracture, but other pathologies − as cleidocranial dysostosis, osteogenesis imperfecta, neurofibromatosis, and previously mentioned genetic syndromes − may occur with CPC.5,8 Clavicle fracture should be suspected in cases of difficult vaginal delivery, pain or limited range of motion in the upper limb, and posterior callus formation evidenced on radiograph.2,4
The present case referred to a young female patient with affected right side and no mobility or function limitation of the upper limb, consistently with the literature.1-10
Clavicle radiograph is usually sufficient to establish CPC diagnosis when history and physical examination are concordant.4,8 Two distinct, non-continuous segments with extremity enlargement, usually overlapping the medial on lateral segments, are usually observed.3,10 No callus or reactive bone are present.
As previously mentioned, most patients are asymptomatic and have no sort of functional limitation, and for that reason some authors recommend no treatment.2,3,8 However, surgical treatment should be considered in symptomatic patients with functional limitation, for cosmetic reasons, and to prevent thoracic outlet syndrome.2-4,6,10 The optimal age for surgery is controversial, with some authors arguing that it should be performed between two and six years of age, with better outcomes when performed between two and four years, given the higher consolidation probability.2,3,10 Surgical treatment consists of pseudarthrosis excision and internal fixation of bone ends with bone grafting.2,3,6,10 In the present case, the girl’s parents chose not to perform surgical treatment.
In summary, with this clinical case the authors intend to alert to CPC as a rare malformation and contribute to recognition of its characteristic physical and radiological findings. It should be noted that persistence of clavicular swelling beyond the first months of life, initially attributed to a neonatal clavicle fracture in this case, should raise suspicion of this entity.
REFERENCES
1. Fitzwilliams D. Hereditary cranio-cleido-dysostosis. The Lancet 1910;2:1466. [ Links ]
2. Beslikas T, Dadoukis D, Gigis I, Nenopoulos S. Congenital pseudarthrosis of the clavicle: a case report. Journal of Orthopaedic Surgery 2007;15:87-90. [ Links ]
3. Figueiredo J, Braga S, Akkari M, Prado J. Congenital Pseudarthrosis of the Clavicle. Rev Bras Ortop. 2012; 47:21-6. [ Links ]
4. Walker B, Vangipuram S, Kalra K. Congenital Pseudoartrosis of the Clavicle: A Diagnostic Challenge. Glob Pediatr Health. 2014; 1:2333794X14563384. [ Links ]
5. Koman L, Thomson J. Congenital Pseudoarthrosis of Clavicle: Background, Pathophysiology, Etiology. Medscape article. 2016. [ Links ]
6. Sung T, Man E, Chan A, Lee W. Congenital pseudarthrosis of the clavicle: a rare and challenging diagnosis. Hong Kong Med J. 2013; 19:265-7. [ Links ]
7. Kalagiri R, Govande V, Hemingway M, Beeram M. Bilateral congenital pseudoarthrosis of the clavicles. Proc (Bayl Univ Med Cent) 2016; 29:387-8. [ Links ]
8. Manashil G, Laufer S. Congenital Pseudarthrosis of the Clavicle: Report of Three Cases. AJR. 1979; 132:678-9. [ Links ]
9. Muradás R, Sevéro M, Silveira J. Pseudoartrose congênita da clavícula. Revista da AMRIGS, Porto Alegre 2009; 53:410-2. [ Links ]
10. Morrissy R, Weinstein S. Lovell and Winter´s Pediatric Orthopaedics. 5th edition, volume 1; Lippincott Williams and Wilkins; 2008; p:359-61. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Juliana Maciel
Department of Pediatrics
Centro Hospitalar de Leiria
Rua das Olhalvas
2410-197 Leiria, Portugal.
Email: julianamaciel@live.com
Received for publication: 27.05.2018
Accepted in revised form: 28.02.2019

