











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
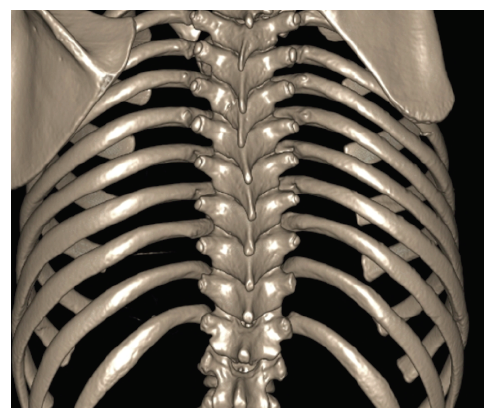
PermalinkA nine-year-old boy without relevant past medical history was referred to the Orthopedic Department due to shoulder asymmetry. He denied pain, other symptoms, or functional limitation in daily activities. On physical examination, the right scapula was at a higher level compared with the left and slightly limited abduction was noted on the right shoulder. Spine x-ray was performed, revealing mild scoliosis, and computed tomography (CT) scan revealed the upper location of the right scapula with ipsilateral clavicle verticalization.
What is your diagnosis?
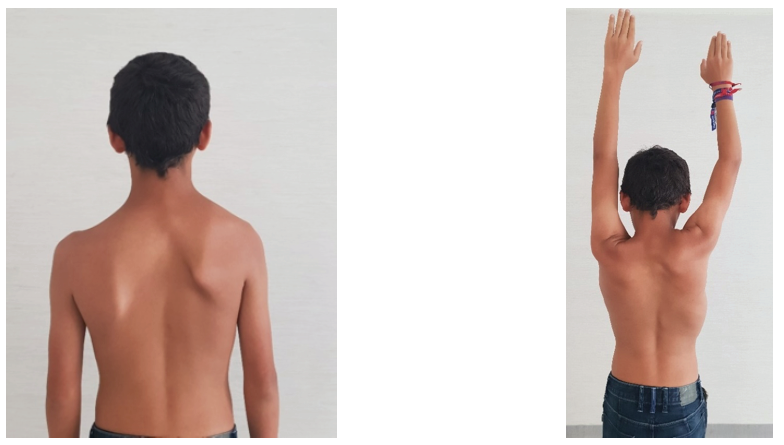
Figure 1 and Figure 2 Asymmetry in the position of scapular poles, with slightly limited abduction on the right shoulder
Discussion
Sprengel deformity is a congenital elevation of the scapula. Although rare, it is described as the most common congenital abnormality of the scapula.1-3 It has a male predominance (3:1) and may be associated with congenital anomalies in the family.3 The condition can occur on both sides concurrently, but is most often unilateral, with a predilection for the left side.4
The scapula develops embryologically during the fifth week in the upper dorsal/lower cervical region and descends up to the final anatomical position by 8-12 weeks of gestation. The pathology in Sprengel’s deformity, which sits the bone 2-10 cm higher, probably represents a continuation of the scapula fetal form joined by failure in descending. Maintenance of a high scapula position can lead to other musculoskeletal defects, such as hypoplasia, medialization, adduction and prominence of the upper angle of the scapula; distal rotation and lateral angulation of glenoid cavity; changes in the position of the clavicle, cervicothoracic vertebrae and ribs; and atrophy of the shoulder musculature.5,6 Moreover, other pathoanatomical anomalies can be found, such as omovertebral bone or costovertebral defects (spina bifida and kyphoscoliosis).5,7
Some syndromes are associated with Sprengel’s deformity, the most common being Klippel-Feil Syndrome, present in about 19-27% of patients with Sprengel’s deformity. Other linked syndromes include teratological conditions, such as anencephaly (a triad of occipital defect, spina bifida of cervical vertebrae, and fixed retroflexion of the head), X-linked dominant hydrocephalus, mental disturbance syndrome, and diastematomyelia. 4,8 In this case report, no evidence of any syndrome was found.
Among differential diagnoses, scapular winging should be considered, in which scapula alignment compared side to side for asymmetry reveals a declination of the affected shoulder, being a painful and debilitating condition. The most common reported causes are dysfunction of the serratus anterior or dysfunction of the trapezius.9
Treatment can be conservative or surgical. Surgery is considered in patients with severe limitation of scapular function, neck pain, or to improve cosmesis.5,8 Surgery should be performed between the ages of three and eight years, due to risk of nerve impairment below the age of eight. Surgical procedures involve a combination of scapular lowering with displacement of the origin or insertion of the scapular muscles on the spine/scapula and resection of the superomedial border. Associated congenital anomalies may be a contraindication to surgery.5 Since the present child had no symptoms, surgical correction was not performed. The patients had two annual follow-ups, during which no changes in signs or symptoms were noted.

