











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Monozygotic pregnancies share a monochorionic placenta in 75% of cases. These monochorionic twins are at risk for several complications during pregnancy due to the possible development of vascular anastomoses connecting their fetoplacental circulations.1 Twin reversed arterial perfusion (TRAP) complicates approximately 2.6% of monochorionic multiple gestations and around 1:35000 pregnancies.1-3 In TRAP, arterial-arterial (A-A) anastomoses carry retrograde perfusion of poorly oxygenated blood from the pump twin (the donor/normal fetus) to the acardiac twin. Venous-venous (V-V) anastomoses divert circulation from the acardiac twin to the pump twin.4 These abnormalities affect both fetuses. The acardiac twin, having a poorly oxygenated blood supply, ends up having impaired growth due to the much greater perfusion of the lower compared to the upper parts of the body, with acephalic-acardiac malformation being the most consistent finding.5 As the acardiac twin continues to grow, the pump twin is also affected by blood overload, resulting in heart failure, hydrops fetalis, polyhydramnios, prreterm delivery, and perinatal death. Consequently, the pregnancy prognosis is largely influenced by the growth of the acardiac twin, with a mortality rate of approximately 50% for the pump twin if no treatment is performed.6-8
This report describes a spontaneous monochorionic multiple pregnancy complicated by TRAP sequence and illustrates how conservative management with a favorable outcome is possible in these cases. The patient provided written informed consent with assurance of confidentiality.
Clinical case
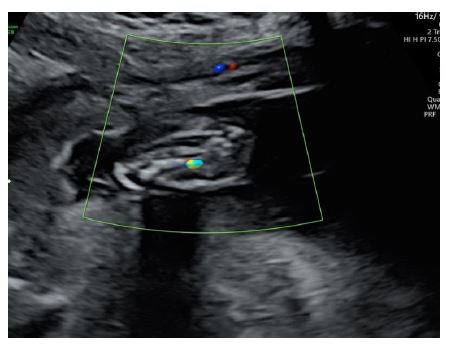
Herein is reported the case of a 21-year-old primipara with a monochorionic-diamniotic spontaneous pregnancy diagnosed at first trimester ultrasound (at 12 weeks’ gestation). The diagnosis of TRAP sequence was established on this first ultrasound after the identification of a structurally abnormal second fetus - an acardiac twin with acrania (acephalus) and limb deformities (Figure 1). These abnormalities persisted until an early second-trimester ultrasound (at 16 weeks’ gestation) with low amniotic fluid but a positive residual, low impedance Doppler signal. Mild growth was noted, with a fetal crown-rump length of 33mm. First trimester aneuploidy screening was negative for the normal fetus, with normal PAPP-A levels. Amniocentesis of the amniotic fluid of the first fetus was performed at 18 weeks, showing a normal karyotype (46-XY). From this moment, no growth was detectes in the acardiac twin, although the Doppler signal remained positive (Figure 2). Throughout the pregnancy, the ultrasound image showed the acardiac twin as a discoid structure in which only bony fragments (probably corresponding to reminiscent vertebral bodies) could be identified. Considering these aspects and taking into account the large size discordance between fetuses, growth cessation of the acardiac twin, and normal development of the pump (normal) twin, it was decided not to perform an invasive technique such as umbilical cord ablation or laser treatment.
The pump twin was evaluated with fetal echocardiogram at 28 weeks gestation, which was normal. Ecoanatomy was also normal, and amniotic fluid volume remained stable between standard values. Fetal growth was normal, with a percentile range of 14 to 25 during the third trimester. The acardiac/pump umbilical venous diameter ratio remained high and stable throughout gestation, suggesting a lower risk of complications for the current pregnancy8.
At 38 weeks, the patient was admitted to the hospital with spontaneous labor. The viable fetus was delivered with 2730 g (p 12), 48.5 cm in length, and Apgar scores of 8/9/9 at 1, 5 and 10 minutes, respectively. The placenta was sent for histologic examination.
Anatomopathologic findings revealed a placenta consistent with monochorionic multiple gestation. In addition, a 25 x 21 x 4mm white compact discoid area was identified adherent to the membranes, showing devitalized embryonic tissue with the spinal cord and a long bone recognizable. In the placental area corresponding to this fetus, the examination showed avascular, sclerotic villi, vasculitis lesions, thrombi, and hemorrhage in the chorionic plate.
The living child is currently two years old and developing normally.

Figure 1 First trimester ultrasound showing multiple gestation with identification of a structurally abnormal second fetus.
Discussion
Acardiac anomaly is a rare complication of monochorionic multiple pregnancies. The cardinal feature is the presence of abnormal vascular connections between the fetuses, which can be observed on the surface of the placenta or in the umbilical cord, suggesting uneven embryonic splitting.7 The consequence is reversed arterial perfusion from the pump twin to the acardiac twin through A-A anastomoses in the placenta with return of blood through V-V anastomoses, creating an extremely hypoxic environment for the acardiac fetus to grow.3 As in this case, if the hypoxia is deep enough and begins early in gestation, organ development is unlikely, and atrophy is higher in the cranial part because the caudal part predominantly consumes all the blood.9 Death of the acardiac twin is certain. In the pump twin, heart failure is common and mortality rate can reach 50%.10 The literature reports that rare cases can survive the third trimester without invasive manipulation, such as ligation and laser ablation.11 Therefore, the option of in utero intervention to reduce the acardiac twin is currently offered as a first-line treatment option to allow the pump twin to develop normally and avoid complications such as polyhydramnios, heart failure, or preterm labor.5 In a meta-analysis of 26 retrospective studies of TRAP sequence, intervention (either by cord occlusion or ablation) conferred a better prognosis than conservative management, especially in cases where poor prognostic features (such as monoamniotic pregnancies, pump twin hydrops or heart failure, pump twin Doppler abnormalities) were present (odds of miscarriage/fetal death with conservative management versus intervention: odds ratio 8.58, 95% confidence interval 1.47-49.96).12
In contrast, Sullivan and colleagues suggested that the neonatal mortality of the pump twin may be considerably lower than reported.13 They believed that conservative management was the best initial approach, as it achieved a 90% survival rate for the normal twin. They considered the cessation of blood flow to the acardiac fetus (which may occur spontaneously) and the size of the acardiac twin, which may remain small and pose no complications. In addition, Ziki et al. also reported a case in which the patient was managed with twice-weekly ultrasound and Doppler evaluation while monitoring for the development of polyhydramnios or heart failure in the pump twin, with a good outcome for the normal twin.14
In the present case, although invasive treatment was a viable option, given growth cessation of the acardiac twin, close pregnancy follow-up with ultrasound (initially every 2 weeks and after growth cessation of the acardiac twin, every 4 weeks) ensured growth stability of the acardiac twin and avoided unnecessary invasive in utero procedures. The pregnancy proceeded without further complications under close monitoring.
The lack of genetic information from the acardiac fetus is a limitation of this study, as it could help to understand the genetic basis of the TRAP sequence.
This case is of particular interest because, although data in the literature indicate that intervention results in better survival than expectant management, the medical team was able to perform close ultrasound follow-up and ensure the safety of a non-invasive approach to this condition. This not only resulted in a term delivery, with a healthy baby, but also avoided iatrogenic damage. Given the high risk of complications, it remains difficult to assess the prognosis of these pregnancies, with or without treatment.15 There was probably no optimal or consensus approach in this case. Each case should be assessed and managed individually, with close follow-up and ultrasound evaluation as key for decision making. The present case suggests the need for caution in the assessment of this type of rare syndromes and to always consider the benefits of a non-invasive approach.
Authorship
Ana Mesquita Varejão - Data curation; Writing - original draft; Writing - review & editing; Investigation
Mariana Dória - Writing - review & editing; Investigation
Mafalda Laranjo - Writing - review & editing; Investigation
Fátima Soares - Supervision
Inês Sarmento Gonçalves - Supervision; Validation

