










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkMedicina Interna
versão impressa ISSN 0872-671X
Medicina Interna vol.27 no.1 Lisboa mar. 2020
https://doi.org/10.24950/Revisão/66/19/1/2020
ARTIGOS DE REVISÃO / REVIEW ARTICLES
The Impact of a Vegetarian Diet in Cardiovascular Risk
O Impacto da Dieta Vegetariana no Risco Cardiovascular
Ana Maria Lé1  http://orcid.org/0000-0002-3559-0413
http://orcid.org/0000-0002-3559-0413
Luís Leite2  https://orcid.org/0000-0002-8493-6935
https://orcid.org/0000-0002-8493-6935
Lino Gonçalves2 http://orcid.org/0000-0001-9255-3064
1Faculdade de Medicina da Universidade de Coimbra, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal
2Serviço de Cardiologia, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal
Abstract:
Introduction:Cardiovascular disease is a leading cause of death and chronic disability and optimizing its prevention and management remains a priority. This review aims to provide a critical analysis on the positive and negative aspects concerning the impact of a vegetarian diet in cardiovascular risk.
Results: Overall, vegetarian population presents better cardiovascular risk profile, expressed by lower body mass index, better blood pressure control, reduced pro-atherogenic lipids and better glycaemic control and insulin sensitivity. Other atherogenic paths seem to be influenced, such as chylomicron remnants removal from circulation, oxidative and inflammation profile, blood fluidity and intestinal microbiota. Furthermore, imaging methods have shown better structural and functional vascular properties among vegetarians. However, a non-balanced vegetarian diet might lead to nutrients deficit, which could nullify these advantages. These limitations may be overcome through a carefully planned diet and, in some cases, supplements or fortified foods. Ultimately, a beneficial effect is associated with a healthy vegetarian concept, with scarce intake of refined and processed food products, avoiding overconsumption of sugar and trans fats.
Conclusion: Vegetarian diet brings a positive impact in several independent cardiovascular risk factors. Despite the additional challenge in reaching specific macro and micronutrients which are less available in plant-based foods, their shortage can be avoided by planning a well-balanced and complete diet, based on healthy and natural food components. As there is the acknowledgment of its limitations and corresponding precautions are taken, a vegetarian diet could be used as an effective weapon towards prevention and management of cardiovascular disease.
Keywords: Cardiovascular Diseases; Diet, Vegetarian; Risk Factors; Vegetarians.
Resumo:
Introdução: A doença cardiovascular é uma causa major de morbimortalidade, pelo que otimizar a sua prevenção e gestão continua a ser uma prioridade. Este artigo de revisão tem em vista providenciar uma análise crítica dos aspetos positivos e negativos acarretados por uma dieta vegetariana no risco cardiovascular.
Resultados: Em geral, a população vegetariana apresenta melhor perfil cardiovascular, com valores mais adequados de índice de massa corporal, perfil lipídico e superior controlo tensional e glicémico. Novos mecanismos aterogénicos parecem ser também influenciados como a remoção dos remanescentes de quilomicrons da circulação, o estado inflamatório e oxidativo e a microbiota intestinal. Adicionalmente, métodos de imagem demonstraram características estruturais e funcionais vasculares mais favoráveis em ve-getarianos. No entanto, uma dieta vegetariana desequilibrada pode conduzir a défices nutricionais. Estes podem ser facilmente ultrapassados através de um plano nutricional completo e variado, e eventualmente recorrendo a suplementos e alimentos fortificados. Acima de tudo, um efeito benéfico do vegetarianismo estará sempre associado a uma dieta vegetariana equilibrada, com base em alimentos saudáveis, e escassez de produtos alimentícios processados, açúcares refinados e gorduras trans.
Conclusão: A dieta vegetariana resulta em impactos positivos em vários fatores de risco cardiovascular independentes. Apesar do desafio acrescido em obter macro e micronutrientes necessários que possam estar menos disponíveis em alimentos de origem vegetal, o seu défice pode ser evitado através de uma dieta planeada, alicerçada em alimentos naturais e saudáveis. Havendo noção das suas limitações e tomadas as devidas providências, uma dieta vegetariana pode ser utilizada eficientemente contra a doença cardiovascular.
Palavras-chave: Dieta Vegetariana; Doenças Cardiovasculares; Fatores de Risco; Vegetarianos.
Introduction
Cardiovascular disease presents itself as a leading global cause of death and chronic disability.1 Every minute someone dies from a heart disease related event.2 These alarming numbers make clear the need to optimize health care, not only with an early and effective treatment but specially by enhancing prevention.
Nutritional patterns have been connected to cardiovascular disease for many years. It has already been demonstrated that dietary factors among other pieces of a healthy lifestyle can largely contribute to reduce both incidence and mortality associated to the cardiovascular system.3
Table 1: The advantages of a vegetarian diet and their respective mechanisms
However, dietary plans are not addressed enough by healthcare providers during medical contact with their patients, probably due to their unawareness of the actual best pattern to follow. Its value goes beyond macro and micronutrients individually ingested, since this perspective does not account for their potentially synergistic interaction. This means the whole nutritional pattern is important, and it might work as a prevention and treatment target.4,5
Following a vegetarian diet means that one does not eat flesh from any animal, including meat or meat products, poultry, fish and seafood.6 There is not only one singular vegetarian diet – for example, ovo-lacto-vegetarian diets allow the ingestion of eggs, milk and dairy products, while having a vegan diet means one does not eat these food items.7,8
Several studies have found a positive impact of vegetarian diet in metabolic profiles and classic modifiable cardiovascular risk factors, such as lipid profile, body mass index, blood pressure and diabetes.9,10 Also, recent researches begin to propose new influencing mechanisms and representative biomarkers.11,12 On the other hand, it also raises some concerns about specific macro and micronutrient deficiencies.9
The goal of this review is to perform a critical analysis on the impact a vegetarian diet might have in cardiovascular risk. We aim to evaluate whether the advantages of a vegetarian diet concerning cardiovascular health surpass its potential risks, and in what way it might be used as a preventive weapon against cardiovascular events.
Results
How can a vegetarian diet influence the lipid pattern?
Total Cholesterol and LDL-C There is a strong and graded positive association between total cholesterol and cardiovascular disease risk. It is well known that along with the plasmatic total amount of cholesterol, the differential between its subtypes is also of extreme importance – the lipid pattern. Higher levels of plasmatic LDL-C are known roots to atherosclerosis, and evidence that its reduction decreases cardiovascular risk is unequivocal.13
Vegetarian diets can reduce total cholesterol and LDL-C plasmatic concentrations. This might occur because they are usually low in fat, specially saturated fatty acids.14
Concerning cardiovascular protection, saturated fatty acid ingestion should not exceed 10% of a daily diet, and polyunsaturated ones should be preferred instead.13 It has been shown that replacing saturated fats with vegetable oil rich in polyunsaturated fatty acids brings significant impact in heart disease prevention, specially by lowering LDL-C levels, with a reduction of cardiovascular risk of about 10%, comparable to a statin effect.15
The principal sources of saturated fat are dairy and meat.16 Therefore, a lack of ingestion of these products might be advantageous to cardiovascular disease avoidance. When major sources of protein change from red meat to nuts and fish, saturated fat, heme-iron and sodium all decrease, while polyunsaturated fats increase.17
Besides, a plant-based diet is high in fibre and many phytochemicals that are able to reduce intestinal absorption of cholesterol molecules.14 Among these phytochemicals there are phytosterols, which have been shown to decrease LDL-C levels by an average of 10% when ingested around 2 g/day, in addition to the reduction that can already be obtained through a low-fat diet. Phytosterols’ intake among vegetarians is almost two times greater than in a omnivores, which is round 200-400 mg/day.18
These effects can be obtained through consumption of soy and non-soy legumes, which are a frequent source of protein intake among vegetarians.19
HDL
HDL-C plasmatic levels, on the other hand, might be inversely correlated with cardiovascular events, which could be explained by its functions – cholesterol esterification and reverse transportation of cholesterol, made from tissues to the liver, which leads to its elimination. Low HDL-C is thought to be associated with increased cardiovascular risk, even though manoeuvres to increase it have not shown a decreasing in this risk.7,20
Concerning HDL-C the results are not consensual. Some came to the conclusion that vegetarian diets are prone to lower plasmatic HDL-C, but in some other ones there was no evidence that its concentrations differed in vegetarians and omnivores.14
On a specific study, a randomised controlled trial based on a 12-week vegetarian diet but with the particularity of being low in fat (representing only 7% - 15% of calorie intake), HDL-C tended to decrease which could be a disadvantage to cardiovascular health.21
Saturated fats increase HDL-C, as well as polyunsaturated fat even though in a smaller scale, which might be the explanation for this diversity. On this specific topic it is important to consider the subtype of vegetarian diet. Lacto-ovo-vegetarians have higher saturated fat and cholesterol intake than vegans, because they include egg yolk, milk and dairy products in their nutritional routine.7 Contrastingly, a vegan person does not consume these products which contribute greatly to HDL-C, and on that account they can reach lower values. Additionally, a great part of HDL-C levels variations in humans are genetically determined.20
Despite this tendency to a lower quantity of HDL-C, studies show vegetarians still achieve a lower TC: HDL ratio.22
Also, it has been shown that having low HDL due to reduced fat intake is not associated with less cardiovascular health.10
Triglycerides
Plasmatic triglyceride levels are already well established as a significant biomarker of cardiovascular risk. Even though it is still under research, it is thought lipoproteins rich in triglycerides also contribute to atherosclerotic mechanism, as well as LDL-cholesterol. Saturated fat intake reduction contributes to a lower triglyceride level, but a higher intake of carbohydrates is associated to its raise, which is something to be aware of in a vegetarian diet.16
Studies about vegetarian diet and plasmatic triglycerides levels ended up creating a controversy. In some of them, a higher number of plasmatic triglycerides was achieved, but this is thought to be due to high ingestion of refined carbohydrates, fructose or saturated fat. This was particularly noticed in lacto-ovo-vegetarian diets.10
Despite the conflicting levels of plasmatic triglycerides reached when comparing vegetarians and omnivores’ lipid profile, there were discovered potential advantages in taking either a vegan or an ovo-lacto-vegetarian diet concerning triglyceride-rich lipoproteins. During absorption of dietary fats two triglyceride-rich lipoproteins are produced: very low-density lipoprotein (VLDL) and chylomicrons. The intravascular catabolism of those lipoproteins leads to the formation of remnants that can be potentially atherogenic by several mechanisms, if accumulated.
Remnants are taken up by macrophages and induce macrophage cholesterol accumulation and foam cell formation. They can also cause endothelium injury by inducting apoptosis, impair endothelium-dependent vasodilation, stimulate arterial smooth muscle cell proliferation, and even increase platelet aggregation.
Chylomicron remnants removal from the circulation seems to be done more efficiently among vegetarians, either vegans and ovo-lacto-vegetarians, which means they might have a positive impact in cholesterol homeostasis and atherosclerosis prevention.7,23
Apolipoprotein B and Apolipoprotein A1
Apolipoprotein B is the main apoprotein of atherogenic lipoproteins, and it appears to be a similar risk marker to LDL-C concerning cardiovascular disease. Apolipoprotein A1, on the contrary, is the major apoprotein of high-density lipoprotein, and its ratio with Apolipoprotein B represents a very strong cardiovascular marker.13
A study comparing cardiovascular biomarkers between healthy vegetarians and omnivores discovered lower levels of apolipoprotein B among vegetarians, contributing to a better cardiovascular risk biomarker profile.24 Another cross-sectional study reported a significantly lower serum concentration of apolipoprotein B specifically in vegans when compared with omnivores, fish-eaters and other vegetarian patterns’ users.25
Concerning apolipoprotein B: apolipoprotein A-1 ratio, a significant difference has been detected between vegans and meat-eaters, even though apolipoprotein A-1 values alone are not conclusive. In men there were no significant differences, while considering women, after BMI adjustment, vegans had lower mean apolipoprotein A-1 than omnivores.25
Could we control body weight through plants?
Body mass index (BMI) and central obesity are considered risk modifiers, that are associated with an increased risk of cardiovascular death.
In addition to the amount of body fat, its distribution is important, and body fat stored in the abdomen carries a higher risk than subcutaneous fat. Therefore, waist-to-hip ratio and waist circumference are also important measurements with established thresholds.13
Excess adiposity increases cardiovascular risk by promoting dyslipidaemia, hypertension, impaired glycaemic control, inflammation, obstructive sleep apnoea and associated hypoventilation and a prothrombotic state.26
Correlation has been made between obesity and a higher rate of cholesterol synthesis, due to leptin resistance observed in this group of people. One of this hormone’s known action is to promote hepatic cholesterol clearance which might be diminished in obese population, leading to a weaker lowering effect of vegetarian diets on total cholesterol, LDL-C and non-HDL-C plasmatic concentrations.14
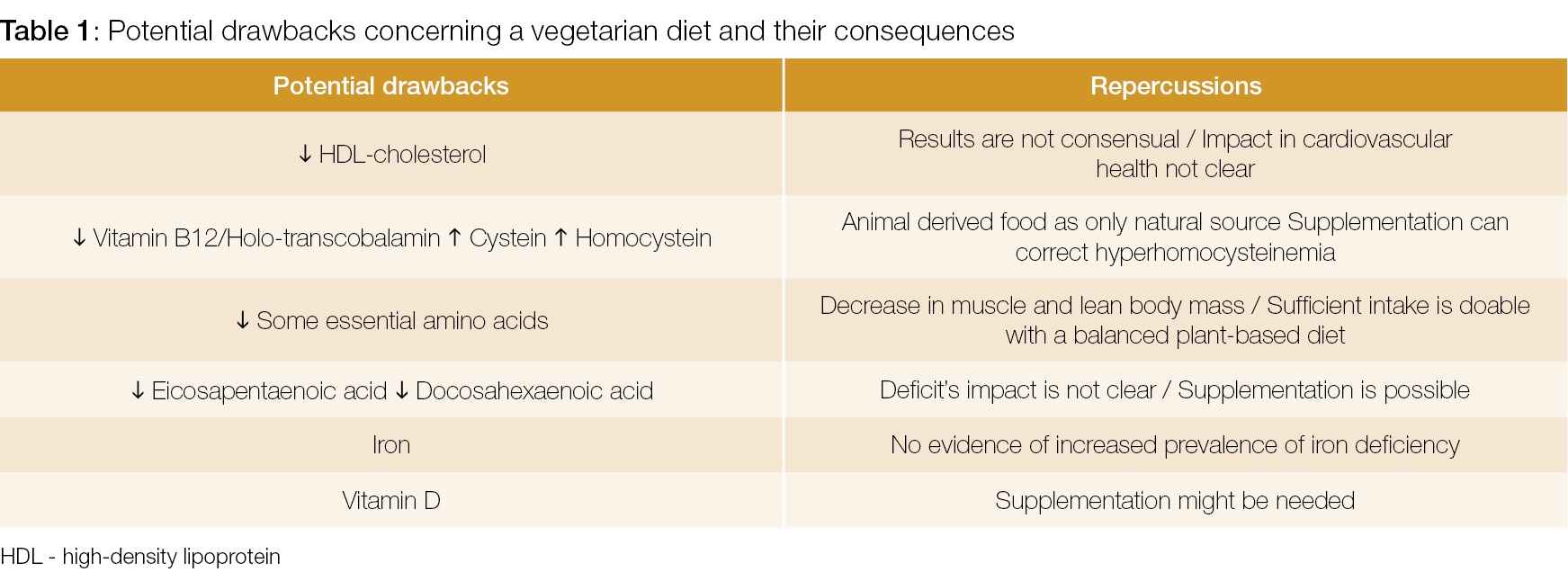
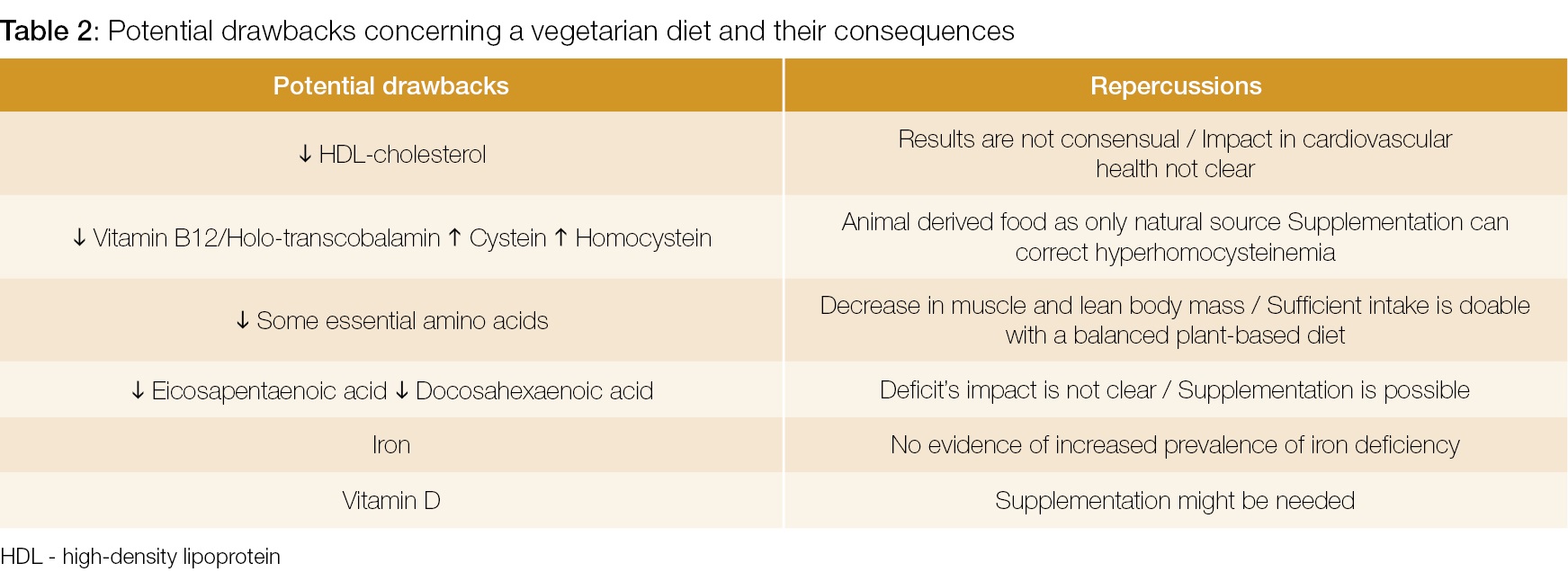
Table 2: Potential drawbacks concerning a vegetarian diet and their consequences
BMI and waist circumference have both been shown to be significantly lower in vegetarians when compared to non-vegetarians, even after age, sex, physical activities, alcohol consumption and education adjustment.10,27
A meta-analysis of randomized controlled trials compared body weight changes between vegetarians and non-vegetarians, confirming a reduction of about 2 kg in the plant-based population. Among vegetarian individuals, interventions with vegan diets resulted in a greater weight loss than those with ovo-lacto-vegetarian diets.28
On another level, as an intervention strategy, a six-month low-fat (7% - 15% of total energy) vegetarian diet, without any calorie restriction or mandatory regular exercise, has been shown to lead to a significant BMI and weight reduction in an either overweight or obese population. The mechanism behind this consequence is probably the lower caloric density of the food consumed, as well as the higher proportion of water and fibre, and it tends to be accentuated among vegans.21
Blood pressure and vascular changes in vegetarians
Vegetarian diets as well as other healthy dietary patterns are among the already well-established nutritional choices one can make to lower blood pressure, along with lower sodium intake, increased potassium ingestion and weight loss.29
It has been consistent over the years in several studies that vegetarians, and particularly vegans, have lower blood pressure levels and smaller preponderance of hypertension when compared to non-vegetarians. Vascular structural and functional changes have also been detected, namely a thinner intima-media thickness reflecting a better endothelial and smooth muscle cells’ function and arterial elasticity and vasodilation. Vasodilatory response and vasodilation’s degree has even been correlated to the vegetarian diet’s extent.27
This outcome might be partially related to a lower BMI detected in vegetarians, but differences in blood pressure between vegetarians and omnivores remaining after age, sex and BMI is adjusted have been demonstrated.30
Also, the higher intake of potassium through the ingestion of whole grains, fruits and vegetables in a bigger proportion is likely to be a great contributing factor.10
New studies have recently discovered that dietary nitrate is able to reduce systolic blood pressure, especially along with antioxidants that support its reduction to nitric oxide (NO). It may additionally play a role against atherosclerosis by preventing adhesion of blood cells to the endothelium and platelet aggregation.2 The provision of dietary nitrate is mainly done by vegetables, and it has been shown that the average nitrate intake might triplicate in vegetarian populations, which might be one of the causes behind this discrepancy.30
Even though with a lower strength of evidence, some studies have suggested that higher intake of protein from plant sources, specially nuts, seeds and soy protein, can reduce blood pressure levels.29 On the contrary, animal protein presents a substantial direct relation to blood pressure increase, mainly accounted by glycine, one of the predominant amino acids.31
Vegetarian diets have consistently been associated with decreased prevalence of insulin resistance, which is also believed to be a fundamental mechanism. This metabolic state might enhance sodium reabsorption in the kidney, leading to increased blood pressure.27
A recent study has gone even further, showing that a plant-based dietary intervention for four weeks might have a stronger impact lowering systolic and diastolic blood pressure than antihypertensive medication. A progressive reduction in chronic stable medication use was made alongside blood pressure decreasing, and participant’s blood pressure levels were better even after discontinuing it. This might mean that a well-defined plant-based diet could even be used as an effective therapeutic approach.32
Type 2 Diabetes: eluding and managing
When compared to non-vegetarians, vegetarian population shows significantly lower fasting glucose levels in healthy subjects.6 Even though these findings are still inconclusive, it has recently been published that impaired glucose tolerance, even in non-diabetic population, might be modestly associated with an increased risk of cardiovascular disease. At this point, lifestyle modifications such as better dietary options are essential.33,34
People with diabetes mellitus are at double the risk of cardiovascular morbimortality.13,34
It has been shown that vegetarianism can lead to about 50% reduction in risk of diabetes, even in previously non-vegetarians who switch their diet to a vegetarian one. In fact, changing to a totally plant-based diet improves glycaemic control in weeks. Vegetarians tend to have lower BMI, and weight loss is generally accompanied by better glycaemic control and insulin sensitivity. However, BMI seems to account for only a small percentage of the protective effect of a plant-based diet on diabetes.35,36
The higher intake of whole grains and vegetables carries greater amounts of fibre, plant polyphenols and magnesium, that have been proven to affect insulin signalling and sensitivity and slow the rate of carbohydrate absorption. Furthermore, soy, a major source of protein in this population, has been shown to diminish insulin resistance when replacing meat.36,37
Additionally, regular consumption of meat is associated with an increased risk of diabetes. It is rich in saturated fats, which have been shown to trigger human B-cell apoptosis, which are responsible for insulin secretion.36 Furthermore, it has also been stated that the dietary source of the fatty acids is of greater relevance, and fatty acids specifically held in meat are negatively associated with insulin secretion and sensitivity.38
Vegetarian diets seem to be helpful not only in prevention but also in treatment and prognosis of the already established disease, and there was reported a significant reduction in plasma glucose levels and HbA1c in patients with type 2 diabetes, with a better glycaemic control.15,39
When compared to a conventional diabetic diet according to the European Association for the Study of Diabetes (EASD), an isocaloric and equally calorie restricted vegetarian diet has increased insulin sensitivity, associated with a reduction of visceral and subcutaneous fat, improvement of oxidative stress and adipokine which reflects loss of adipose tissue.40
Oxidative stress and inflammation – the key factor
Oxidative stress and inflammation play a major role in vascular disorders and circulation defects and contribute to the development of metabolic syndrome. Oxidative stress occurs when there is a disproportion between prooxidants and antioxidants, favouring the first ones.41
A low-calorie vegetarian diet adopted for three months by randomly overweight omnivores led to a significant improvement in oxidative stress profile, which supports this potential vegetarianism cardiovascular advantage.42 This beneficial effect is most likely related with higher intake of antioxidant compounds such as ascorbic acid, carotenoids and flavonoids that confer a protective role against oxidative damage, leading to a lower risk of cardiovascular disease. Additionally, the lipophilic antioxidant vitamin E is known to be an antiatherogenic and anti-inflammatory agent.43
Plasma ascorbic acid concentrations have been shown to be nearly 50% higher in a vegetarian population when compared to non-vegetarians. These numbers were inversely correlated with unstable coronary artery disease activity in patients with established cardiovascular disease, as well as cardiovascular disease mortality.43
Plasmatic biomarkers concerning oxidative profile and inflammatory status may also help assessing cardiovascular health, and C-reactive protein (CRP) is validated as an independent predictor biomarker of cardiovascular disease. A long-term vegetarian diet was found to be associated with lower values of high-sensitivity CRP,43 but this has not been consistent over the researches developed on the topic. Some studies found no significant disparity in CRP levels between vegetarians and omnivores. This could be because vegetarians have lower intake of other relevant nutritional components such as anti-inflammatory omega-3 (n-3) fatty acids and vitamin D, which may lessen the expected anti-inflammatory effect.24,27
New circulating biomarkers have been recently studied to be anticipatory of a higher cardiovascular risk. Higher concentration and activity of matrix metalloproteinases (MMPs) may predict a greater risk of cardiovascular disorders, specifically MMP-2 and MMP-9. These biomarkers are inflammation-related and have been associated with hypertension-induced cardiovascular remodelling, atherosclerotic mechanism development, and aneurysm related cardiovascular maladaptation. Additionally, myeloperoxidase (MPO) is an important prooxidant enzyme associated with cardiovascular diseases, which role is to produce reactive oxygen species (ROS) when in oxidative stress. In higher concentrations, ROS will cause endothelial dysfunction and arterial remodelling. It has been shown that vegetarian diets are associated to lower concentrations of the above mentioned biomarkers, which can reinforce evidence of a reduced predisposition to cardiovascular events in such population.11
Blood viscosity
Blood viscosity may influence cardiovascular health since it plays a role in atherosclerosis, thrombosis and ischemic events. It increases along with haematocrit levels and they both contribute to platelet adhesion and deposition, favouring thrombotic complications. Additionally, there is a positive association between total cholesterol and triglycerides concentrations and blood viscosity, because in elevated levels they cause impairment of erythrocytes morphology and flow behaviour, which enhance their aggregation.44
Increased erythrocyte aggregation and altered blood viscosity have additionally been linked to oxidative stress, as a result of oxidative damage to erythrocytes.41
It has already been shown blood fluidity can be increased by adopting a vegetarian diet, most likely by virtue of being a dietary pattern low in saturated fats and total cholesterol and, on the other hand, high in antioxidants.44
Intestinal microbiota – the latest breakthrough
Recently, another contributory cause to atherosclerotic mechanism has been studied: trimethylamine (TMA). It is contained in some dietary compounds of meat, milk, and other animal derived foods, namely lecithin, choline betaine and carnitine, which are converted by intestinal bacterial enzymes into TMA. TMA is posteriorly absorbed and oxidized into a toxic component – trimethylamine N-oxide (TMAO) - which has been shown to enhance oxidized LDL uptake by macrophages in atherosclerosis mechanism. TMAO appears to play a role in promoting atherosclerosis by activating macrophages and foam cells and it is elevated in patients with coronary heart disease.
TMAO’s synthesis is an intestinal-microbiota-dependent mechanism, which means conversion into TMA from substrates only happens with enzymes from some specific microorganisms, which may or may not be present in each host’s microbiota. Long-term vegetarians, not only do not ingest these substrates found in animal food products, but they also lose the ability to produce TMA due to their different type of microbiota.9,12,45
According to this new hypothesis, it is clear why a dietary routine which does not include animal derived items might be advantageous in minimizing atherosclerotic cardiovascular disease.46
There is no rose without a thorn
Despite all the benefits shown above regarding this nutritional pattern, a non-balanced vegetarian diet could lead to nutrients deficit which could nullify these advantages.47
Vitamin B12
The main source of cobalamin intake in general population comes from animal derived foods, with a significant contribution from dairy products. Recommended dietary intake values vary among authors, ranging between 2.4 to 4 ug per day in adults. With aging, there is a reduction in absorptive capacity and some researchers believe this amount may not be sufficient anymore.47
Recent studies report low plasmatic cobalamin among vegetarian population. This vitamin can actually be found in some plant derived foods, such as mushrooms, seaweeds, fermented soy products like tempeh, but not in consistently relevant amounts. However, the use of supplements or fortified food products are able to prevent deficiencies, indicating that a well-planned vegetarian diet is potentially sustainable.48,49
The association between low levels of holo-transcobalamin, the functional available form of vitamin B12, and higher rates of coronary artery disease among vegetarian people has already been demonstrated.50
Concerning this cardiovascular impact, it is known that plasmatic homocysteine and cysteine tend to accumulate in vegetarian population due to vitamin B-12 deficiency. A few studies have reported a relationship between raised homocysteine plasmatic levels and increased arterial stiffness, atherogenicity and inflammation, as well as higher likelihood of cardiovascular events.46,24 More recently, cysteine has been linked to coronary artery disease in a vegetarian population study.50
Even though it has been shown that vitamin B12 supplementation is able to quickly correct hyperhomocysteinemia, there is no solid proof that it brings a significant positive impact in vegetarians’ cardiovascular health.48
Besides vitamin B12 deficiency-induced hyperhomocysteinemia, lacking of this vitamin may lead to macrocytosis and increased RDW, which is associated with circulatory problems and a higher rate of cardiovascular events.48
Also, a causal relationship between vitamin B12 deficiency and low levels of HDL has been proven and explained by a downregulation of peroxisome proliferator-activated receptor a (PPAR a), which is responsible for HDL’s major protein component synthesis, apolipoprotein A1.50
There is no unanimity on supplementing vegetarian population. Lacto-ovo-vegetarians can get adequate vitamin B-12 from dairy foods and eggs, but for vegans it must be obtained from fortified foods or supplements.51 It is also important to point out that supplementation with multivitamins can actually be counterproductive since cobalamin can be degraded in the presence of vitamin C and copper.47
Protein
Protein intake is one of the most popular concerns when one choses to embrace a vegetarian diet. Protein is made up of smaller units called amino acids, some of which must be obtained from food since they cannot be synthesized by the human body – these are called essential amino acids. Contrarily to popular belief, these special amino acids are not exclusively found in meat, dairy products and eggs. Their intake is also possible through a well-balanced plant-based diet as long as there is a proper combination of food products.9 Actually, vegetarian, including vegan, diets with an adequate caloric intake usually meet or even exceed recommended protein intake.52
Furthermore, vegetarians get protein from different sources than omnivores, which appears to be advantageous to cardiovascular health. As mentioned above, red meat, specially processed meat, has been positively correlated to cardiovascular disease risk.17
On the other hand, soy products might have a positive impact on lipid profile, blood pressure and insulin resistance,14,29,36 and protein derived from nuts and seeds carries a protective cardiovascular effect. Nuts carry high content glutamic acid, which has been shown to have lowering blood pressure effects, as well as L-arginine, a precursor of nitric oxide, which is essential to vascular health.53,54
However, restrictive vegan diets may be low in protein and essential amino acids such as leucine, lysine and methionine. This deficiency can lead to a decrease in lean body mass which might be another cause of hyperhomocysteinemia, even in the absence of vitamin deficiency.55
Low intake of n-3 fatty acids
Several studies concluded that greater intake of long-chained n-3 fatty acids, such as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), is associated with lower risk of fatal cardiovascular disease. Also, Omega-3 Index, which represents the percentage of EPA and DHA among all fatty acids in red blood cells’ membrane, works as an independent risk predictor for cardiac disease, and it is validated as a representative biomarker of long-term n-3 fatty acid status.56 Small intakes of EPA and DHA were also associated in previous studies to insulin resistance 37 and enhanced platelet aggregability, which might explain their association with cardiovascular disease risk.46
a-linolenic acid (ALA) is the most relevant n-3 fatty acid found in plants, and it can be obtained through the ingestion of vegetarian friendly foods like walnuts and soybeans. ALA does not present the same protective effects regarding cardiovascular health.37 Despite ALA may be endogenously transformed into EPA and DHA, this conversion is very sparse.22
Even though Omega-3 Index and plasmatic DHA were shown to be significantly lower in vegetarians, this population still shows reduced cardiovascular risk when compared to omnivores, and this changes’ impact in overall heart health of this population is yet to be discovered.46 However, it is possible that cardiovascular risk could be even more reduced by correcting this shortfall.8,56
When supplementation with these long-chained n-3 PUFAs was tested in vegetarians, a reduction in platelet aggregation percentage was observed along the raise in plasmatic EPA and DHA. Additionally, EPA was proven to reduce the risk of major ischemic events and cardiovascular mortality in patients with elevated triglyceride levels.57 On the contrary, supplementation with ALA seems to be ineffective increasing conversion to long-chained n-3 PUFAs, so it is probably useless.46,58
Nowadays, ESC recommends fish consumption 1-2 times per week, one of which to be oily fish, which would provide around 400-500 mg EPA and DHA a day. For people who do not consume fish, this intake might be replaced with fish oil capsules or DHA-rich microalgae. However, guidelines are not universally consensual, and little is still known about what the most cardioprotective supplement dosage would be. Therefore, more investigation should be performed in order to effective supplementation can be prescribed.13,59
Positive effects of w-6 fatty acids on total and LDL-cholesterol and blood pressure have also been proven, so adequate intake of both subtypes is important to lower risk of cardiovascular disease.35
Iron
Iron shortage is a very common nutritional disorder, and it can lead to anaemia and interfere with cardiovascular health. It has been shown risk of coronary artery disease rises with iron depletion, independently of concomitant anaemia.60
Meat is usually the biggest contributor regarding iron supply when compared to other food groups. Even though there is a great amount of iron in a plant-based diet, absorption of heme iron abundant in red meat is better than non-heme iron found in plant foods.61
Notwithstanding, a meta-analysis suggested that heme iron intake may be considered a cardiovascular disease risk factor.62
Furthermore, there is no evidence iron shortage is more frequent in vegetarians, who tend to consume larger amounts of food rich in vitamin C, which improves non-heme iron absorption and nullifies a potential deficiency risk.9
Vitamin D
Dietary vitamin D intake among vegetarians is significantly lower when comparing with omnivores. Plus, it is mainly consumed in the form of vitamin D2 which is less bioavailable than animal derived Vitamin D3.9,63,64
Vitamin D plays a role in regulating endothelial nitric oxide synthase and arterial stiffness. Previous studies showed that vitamin D deficiency is associated with raised arterial calcification, inflammation, imbalanced vasoconstriction and vasodilation score and, therefore, an increased cardiovascular risk.64,65
However, higher levels of vitamin D can also be deleterious towards cardiovascular health, forming a an U-shaped dose-response curve between vitamin D levels and systolic blood pressure and arterial stiffness.63
This means considering supplementation might be needed, but it must be carefully evaluated in each situation so plasmatic levels do not surpass the point where they represent an adverse cardiovascular effect. Plus, there is no certainty that correction of vitamin D deficiency will have an impact in CVD.63,64
Are all vegetarian diets healthy?
It is important to be aware that a vegetarian diet per se may have many different approaches, and it is possible to be a vegetarian and still have a great ingestion of refined and processed food products, with overconsumption of sugar and trans fats.66
Three prospective cohort studies were developed to compare the coronary heart disease impact between an overall plant-based diet, a healthy plant-based diet and an unhealthy plant-based diet. This last option included fruit juices, refined grains, potatoes, sugar sweetened beverages and sweets or desserts. They realized that a healthier version of a plant-based diet is in fact associated with lower coronary heart disease. Contrarily, when intake of less healthy plant foods mentioned above was emphasized, the opposite association was observed.67
Whole grain cereals are rich in fibre which makes them advantageous by lowering insulin resistance, facilitating weight control and improving lipid profile, endothelial function and inflammatory status.3,68
A meta-analysis of prospective cohort studies said daily intake of 30 g of nuts diminishes cardiovascular disease risk by 30%, and they are a very good alternative to protein and fatty acids intake. Even though it is crucial to acknowledge that energy density of nuts is high, it has unexpectedly been found an inverse association between nut consumption and body weight, BMI and waist circumference. Legumes are also a great source of vegetable protein, which may help improving blood cholesterol and controlling body weight.13,17,69
In contrast to natural vegetarian food items containing fruits, vegetables and whole grains, refined grains and carbohydrates and processed foods often increase the risk of type 2 diabetes, such as white rice, fried snacks, or sugar added products like sugar-sweetened beverages.35
The trans fatty acids are a subtype of unsaturated fats that have been shown to be especially harmful on cardiovascular health, and they can be naturally found in meat and milk of ruminant animals or be synthetized during fats industrial processing. Therefore, they can still be found in vegetarian diets for example in margarine, fast-food and bakery products and packaged fried snacks, and carry a great influence increasing total cholesterol, LDL-C, apolipoprotein B, triglycerides, and decreasing HDL-C and apolipoprotein A1.
On average, a 2% increase in energy intake from trans fats increase cardiovascular disease risk by 23%. It is recommended that less than 1% of total energy intake derives from trans fatty acids, considering that the less the better. Hence, this unnatural food products intake should also be discouraged within a vegetarian diet.13,16
Processed food also contributes, on average, to 80% of salt intake, which should not overpass 5 g per day according to recommendations. Salt reduction is an important strategy to prevent coronary artery disease, which is an additional motive to reduce these products’ intake.13
Conclusion
Cardiovascular disease is a leading cause of morbimortality which makes it crucial to find new prevention and management strategies.1
We realized through this review that following a vegetarian diet brings a beneficial effect in several independent cardiovascular risk factors. Recent studies on the topic keep on finding new mechanisms through which such positive impact is done.
Even though there are some challenges in reaching specific macro and micronutrients which are less available in plant-based foods, their insufficiency can usually be avoided by planning a well-balanced and complete diet, built with healthy and natural food components.
Overall, even despite some potential deficiencies, vegetarian population showed a reduced cardiovascular risk. Therefore, a vegetarian diet can represent an effective therapeutic approach concerning cardiovascular risk reduction, considering there is the awareness of its potential limitations and corresponding precautions are taken.
REFERENCES
1. Roth GA, Johnson C, Abajobir A, Abd-Allah F, Abera SF, Abyu G, et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J Am Coll Cardiol. 2017;70):1–25. doi: 10.1016/j.jacc.2017.04.052.
2. Bryan NS. Functional Nitric Oxide Nutrition to Combat Cardiovascular Disease. Curr Atheroscler Rep [Internet]. 2018;20:21. doi:10.1007/s11883-018-0723-0%0A [ Links ]
3. Dinu M, Pagliai G, Sofi F. A Heart-Healthy Diet: Recent Insights and Practical Recommendations. Curr Cardiol Rep. 2017;19 :95. doi: 10.1007/s11886-017-0908-0. [ Links ]
4. Widmer RJ, Flammer AJ, Lerman LO, Lerman A. The Mediterranean diet, its components, and cardiovascular disease. Am J Med. 2015;128:229–38. doi:10.1016/j.amjmed.2014.10.014
5. Dinu M, Pagliai G, Casini A, So F. Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses of observational studies and randomised trials. Eur J Clin Nutr. 2017;72:30–43. doi: 10.1038/ejcn.2017.58.
6. Dinu M, Abbate R, Gensini GF, Casini A, Sofi F. Vegetarian, vegan diets and multiple health outcomes: A systematic review with meta-analysis of observational studies. Crit Rev Food Sci Nutr [Internet]. 2017;57:3640–9. doi:10.1080/10408398.2016.1138447
7. Vinagre JC, Vinagre CCG, Maranha RC. Plasma kinetics of chylomicron-like emulsion and lipid transfers to high-density lipoprotein (HDL) in lacto-ovo vegetarian and in omnivorous subjects. Eur J Nutr. 2014;53:981–7.
8. Harris WS. Achieving optimal n–3 fatty acid status: the vegetarian’s challenge… or not. Am J Clin Nutr. 2014;100:449–52.
9. Patel H, Chandra S, Alexander S, Soble J, Allan K, Sr W. Plant-based nutrition: an essential component of cardiovascular disease prevention and management. Curr Cardiol Rep. 2017;19:104. doi: 10.1007/s11886-017-0909-z. [ Links ]
10. Chiu YF, Hsu CC, Chiu THT, Lee CY, Liu TT, Tsao CK, et al. Cross-sectional and longitudinal comparisons of metabolic profiles between vegetarian and non-vegetarian subjects: A matched cohort study. Br J Nutr. 2015;114:1313–20.
11. Navarro JA, de Gouveia LA, Rocha-Penha L, Cinegaglia N, Belo V, Castro MM de, et al. Reduced levels of potential circulating biomarkers of cardiovascular diseases in apparently healthy vegetarian men. Clin Chim Acta. 2016;461:110–3. doi:10.1016/j.cca.2016.08.002
12. Spector R. New insight into the dietary cause of atherosclerosis: implications for pharmacology. J Pharmacol Exp Ther. 2016;358:103–8. doi: 10.1124/jpet.116.233296.
13. Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur Hear J. 2016;37:2315–81. doi: 10.1093/eurheartj/ehw106.
14. Wang F, Zheng J, Yang B, Jiang J, Fu Y, Li D. Effects of vegetarian diets on blood lipids: A systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc. 2015;4 :e002408. doi: 10.1161/JAHA.115.002408. [ Links ]
15. Kahleova H, Levin S, Barnard N. Cardio-metabolic benefits of plant-based diets. Nutrients. 2017;9: E848. doi: 10.3390/nu9080848. [ Links ]
16. Sacks FM, Lichtenstein AH, Wu JHY, Appel LJ, Creager MA, Kris-Etherton PM, et al. Dietary fats and cardiovascular disease: A presidential advisory from the American Heart Association. Circulation. 2017;136:e1–e23. doi: 10.1161/CIR.0000000000000510.
17. Bernstein AM, Sun Q, Hu FB, Stampfer MJ, Manson JE, Willett WC. Major dietary protein sources and risk of coronary heart disease in women. Circulation. 2010;122:876–83.
18. Ras RT, Geleijnse JM, Trautwein EA. LDL-cholesterol-lowering effect of plant sterols and stanols across different dose ranges: A meta-analysis of randomised controlled studies. Br J Nutr. 2014;112:214–9.
19. Bazzano LA, Thompson AM, Tees MT, Nguyen CH, Winham DM. Non-soy legume consumption lowers cholesterol levels: A meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2011;21:94–103. doi:10.1016/j.numecd.2009.08.012
20. Zhang Z, Wang J, Chen S, Wei Z, Li Z, Zhao S, et al. Comparison of vegetarian diets and omnivorous diets on plasma level of HDL-c: A meta-analysis. PLoS One. 2014;9 :e92609. doi: 10.1371/journal.pone.0092609. [ Links ]
21. Wright N, Wilson L, Smith M, Duncan B, Mchugh P, Wright N. The BROAD study: A randomised controlled trial using a whole food plant-based diet in the community for obesity, ischaemic heart disease or diabetes. Nutr Diabetes. 2017;7:256–66. doi:10.1038/nutd.2017.3
22. Burns-whitmore B, Haddad E, Sabaté J, Rajaram S. Effects of supplementing n-3 fatty acid enriched eggs and walnuts on cardiovascular disease risk markers in healthy free-living lacto-ovo-vegetarians : a randomized , crossover, free-living intervention study. Nutr J. 2014;13:29. doi: 10.1186/1475-2891-13-29. [ Links ]
23. Vinagre JC, Vinagre CG, Pozzi FS, Slywitch E, Maranha RC. Metabolism of triglyceride-rich lipoproteins and transfer of lipids to high-density lipoproteins ( HDL ) in vegan and omnivore subjects. Nutr Metab Cardiovasc Dis. 2013;23:61-7. doi: 10.1016/j.numecd.2011.02.011. [ Links ]
24. Acosta-Navarro J, Antoniazzi L, Oki AM, Bonfim MC, Hong V, Acosta-Cardenas P, et al. Reduced subclinical carotid vascular disease and arterial stiffness in vegetarian men: The CARVOS Study. Int J Cardiol. 2017;230:562–6. doi: 10.1016/j.ijcard.2016.12.058.
25. Bradbury KE, Crowe FL, Appleby PN, Schmidt JA, Travis RC, Key TJ. Serum concentrations of cholesterol, apolipoprotein A-I and apolipoprotein B in a total of 1694 meat-eaters, fish-eaters, vegetarians and vegans. Eur J Clin Nutr. 2013;68:178–83. doi:10.1038/ejcn.2013.248
26. Trepanowski JF, Varady KA. Veganism is a viable alternative to conventional diet therapy for improving blood lipids and glycemic control. Crit Rev Food Sci Nutr. 2014;55:2004–13.
27. Chuang S-Y, Chiu THT, Lee C-Y, Liu T-T, Tsao CK, Hsiung CA, et al. Vegetarian diet reduces the risk of hypertension independent of abdominal obesity and inflammation. J Hypertens. 2016;34:2164–71. doi: 10.1097/HJH.0000000000001068.
28. Huang R, Huang C, Hu FB, Jorge E. Vegetarian diets and weight reduction: a meta-analysis of randomized controlled trials. J Gen Intern Med. 2016;31:109–16.
29. Appel LJ. The Effects of Dietary Factors on Blood Pressure. Cardiol Clin. 2017;35:197–212. doi:10.1016/j.ccl.2016.12.002
30. Ashworth A, Bescos R. Dietary nitrate and blood pressure: evolution of a new nutrient? Nutr Res Rev. 2017;30:208-219. doi: 10.1017/S0954422417000063. [ Links ]
31. Pressure B, Stamler J, Brown IJ, Daviglus ML, Chan Q, Miura K, et al. Dietary glycine and blood pressure: the International Study on Macro/Micronutrients and Blood Pressure. Am J Clin Nutr. 2013;98:136–45.
32. Moore CE, Montgomery BD, Najjar RS. A defined, plant-based diet utilized in an outpatient cardiovascular clinic effectively treats hypercholesterolemia and hypertension and reduces medications. Clin Cardiol. 2018;41:307–13. doi: 10.1002/clc.22863.
33. Li G, Zhang P, Wang J, An Y, Gong Q, Gregg EW, et al. Cardiovascular mortality, all-cause mortality, and diabetes incidence after lifestyle intervention for people with impaired glucose tolerance in the Da Qing Diabetes Prevention Study: a 23-year follow-up study. Lancet Diabetes Endocrinol. 2014; 2:474-80. doi: 10.1016/S2213-8587(14)70057-9.
34. The Emerging Risk Factors Collaboration. Diabetes mellitus , fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet Diabetes Endocrinol. 2010;375:2215–22. doi:10.1016/S0140-6736(10)60484-9
35. Kahleova H, Pelikanova T. Vegetarian diets in the prevention and treatment of type 2 diabetes. J Am Coll Nutr. 2015;34:448–58.
36. Chiu TH, Pan WH, Lin MN, Lin CL. Vegetarian diet, change in dietary patterns, and diabetes risk: a prospective study. Nutr Diabetes. 2018;8:12–25. doi: 10.1038/s41387-018-0022-4.
37. Tonstad S, Stewart K, Oda K, Batech M, Herring RP, Fraser GE. Vegetarian diets and incidence of diabetes in the Adventist Health Study-2. Nutr Metab Cardiovasc Dis. 2013;23:292–9. doi:10.1016/j.numecd.2011.07.004
38. Wanders AJ, Alssema M, Koning EJP De, Cessie S, Vries JH De, Zock PL, et al. Fatty acid intake and its dietary sources in relation with markers of type 2 diabetes risk: The NEO study. Eur J Clin Nutr. 2017;71:245–51. doi:10.1038/ejcn.2016.204
39. Bittner VA. The New 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease Circulation. 2019 (in press). doi:10.1161/CIRCULATIONAHA.119.040625 [ Links ]
40. Kahleova H, Matoulek M, Malinska H, Oliyarnik O, Kazdova L, Neskudla T, et al. Vegetarian diet improves insulin resistance and oxidative stress markers more than conventional diet in subjects with type 2 diabetes. Diabet Med. 2011;28:549–59. doi: 10.1111/j.1464-5491.2010.03209.x.
41. Gyawali P, Richards RS. Association of altered hemorheology with oxidative stress and inflammation in metabolic syndrome. Redox Rep. 2015;20:139–45.
42. Sofi F, Dinu M, Pagliai G, Cesari F, Gori AM, Sereni A, et al. Low-calorie vegetarian versus mediterranean diets for reducing body weight and improving cardiovascular risk profile. Circulation. 2018;137:1103–13. doi: 10.1161/CIRCULATIONAHA.117.030088.
43. Szeto YT, Kwok TC, Benzie IF. Effects of a long-term vegetarian diet on biomarkers of antioxidant status and cardiovascular disease risk. Nutrients. 2004;20:863–6.
44. Naghedi-baghdar H, Nazari S, Taghipour A, Nematy M, Shokri S, Mehri M, et al. Effect of diet on blood viscosity in healthy humans: a systematic review. Electron Physician. 2018;10:6563-70. doi: 10.19082/6563. [ Links ]
45. Tuso P. A Plant-Based Diet, Atherogenesis, and Coronary Artery Disease Prevention. Perm J. 2015;19:62–7.
46. Rosario VA, Fernandes R, Trindade EBSDM. Vegetarian diets and gut microbiota: important shifts in markers of metabolism and cardiovascular disease. Nutr Rev. 2016;74:444–54.
47. Rizzo G, Laganà AS, Maria A, Rapisarda C, Maria G, La G, et al. Vitamin B12 among vegetarians: status, assessment and supplementation. Nutrients. 2016;8:101–24.
48. Pawlak R. Is vitamin B12 deficiency a risk factor for cardiovascular disease in vegetarians? Am J Prev Med. 2015;48:11–26. doi:10.1016/j.amepre.2015.02.009
49. Wegmüller RSR, Bui CBM, Aeberli IH. Micronutrient status and intake in omnivores, vegetarians and vegans in Switzerland. Eur J Nutr. 2017;56:283–93.
50. Basak T, Garg G, Bhardwaj N, Tanwar VS, Seth S, Karthikeyan G, et al. Low holo-transcobalamin levels are prevalent in vegetarians and is associated with coronary artery disease in Indian population. Biomarkers. 2016;21:436–40. doi: 10.3109/1354750X.2016.1153718.
51. Diets V. Position of the American Dietetic Association: Vegetarian Diets. J Am Diet Assoc. 2009;109:1266–82.
52. Melina V, Levin S, Craig W. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J Acad Nutr Diet. 2016;116):1970–80.
53. Tharrey M, Mashchak A, Barbillon P, Delattre M, Fraser GE. Patterns of plant and animal protein intake are strongly associated with cardiovascular mortality: the Adventist Health Study-2 cohort. Int J Epidemiol. 2018;47:1603-1612. doi: 10.1093/ije/dyy030. [ Links ]
54. Otero J, Camacho PA, Fornasini M, López-Jaramillo P, Baldeón M. Reevaluating nutrition as a risk factor for cardio-metabolic diseases. Colomb Med. 2018;49:175–81.
55. Ingenbleek Y, McCully KS. Vegetarianism produces subclinical malnutrition, hyperhomocysteinemia and atherogenesis. Nutrition. 2012;28:148–53. doi:10.1016/j.nut.2011.04.009
56. Sanders TAB. Plant compared with marine n–3 fatty acid effects on cardiovascular risk factors and outcomes: what is the verdict? Am J Clin Nutr. 2014;100:453–8.
57. Bhatt DL, Steg PG, Miller M, Brinton EA, Jacobson TA, Ketchum SB, et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N Engl J Med. 2019;380:11-22. doi: 10.1056/NEJMoa1812792. [ Links ]
58. Hall WL. The future for long chain n-3 PUFA in the prevention of coronary heart disease: do we need to target non-fish-eaters? Proc Nutr Soc. 2017;76:408–18. doi:10.1017/S0029665117000428.
59. Gebauer SK, Psota TL, Harris WS, Kris-etherton PM. n-3 Fatty acid dietary recommendations and food sources to achieve essentiality and cardiovascular benefits. Am J Clin Nutr. 2006;83:1526–35.
60. Haehling S Von, Jankowska EA, Veldhuisen DJ Van, Ponikowski P, Anker SD. Iron deficiency and cardiovascular disease. Nat Rev Cardiol . 2015;12:659–69. doi: 10.1038/nrcardio.2015.109
61. Richi EB, Baumer B, Conrad B, Darioli R, Schmid A, Keller U. Health Risks Associated with Meat Consumption: A Review of Epidemiological Studies. Int J Vitam Nutr Res. 2015;85:70–8.
62. Fang X, An P, Wang H, Wang X, Shen X, Li X, et al. Dietary intake of heme iron and risk of cardiovascular disease: A dose-response meta-analysis of prospective cohort studies. Nutr Metab Cardiovasc Dis. 2015;25:24–35.
63. Mirhosseini NZ, Knaus SJ, Bohaychuk K, Singh J, Vatanparast HA, Weber LP. Both high and low plasma levels of 25-hydroxy vitamin D increase blood pressure in a normal rat model. Br J Nut. 2016;116:1889–900.
64. Rai V, Agrawal DK. Role of vitamin D in cardiovascular diseases. Endocrinol Metab Clin North Am . 2017;46:1039–59.doi: 10.1016/j.ecl.2017.07.009
65. Ou S, Chen M, Huang C, Chen N. Potential role of vegetarianism on nutritional and cardiovascular status in Taiwanese dialysis patients: a case-control study. PLoS One. 2016;11:e0156297. doi: 10.1371/journal.pone.0156297 [ Links ]
66. Misra R, Balagopal P, Raj S, Patel TG. Vegetarian diet and cardiometabolic risk among Asian Indians in the United States. J Diabetes Res. 2018;2018:1675369. doi: 10.1155/2018/1675369. [ Links ]
67. Satija A, Bhupathiraju SN, Spiegelman D, Chiuve SE, Manson JAE, Willett W, et al. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in U.S. adults. J Am Coll Cardiol. 2017;70:411–22. doi: 10.1016/j.jacc.2017.05.047.
68. Aune D, Giovannucci E, Boffetta P, Riboli E, Vatten LJ, Tonstad S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality a systematic review and dose-response meta-analysis of prospective studies. Int J Epidemiol. 2017;46:1029–56.
69. Brown RC, Id ARG, Tey SL, Chisholm A, Burley V, Id DCG, et al. Associations between nut consumption and health vary between omnivores, vegetarians, and vegans. Nutrients. 2017;9:12–6.
Responsabilidades Éticas
Conflitos de Interesse: Os autores declaram a inexistência de conflitos de interesse na realização do presente trabalho.
Fontes de Financiamento: Não existiram fontes externas de financiamento para a realização deste artigo.
Ethical Disclosures
Conflicts of interest: The authors have no conflicts of interest to declare.
Financing Support: This work has not received any contribution, grant or scholarship
© Autor (es) (ou seu (s) empregador (es)) 2019. Reutilização permitida de acordo com CC BY-NC. Nenhuma reutilização comercial.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use.
Correspondence / Correspondência:
Ana Maria Lé – anamariafle@gmail.com
Faculdade de Medicina da Universidade de Coimbra, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal
R. Larga 2, 3000-370 Coimbra
Received / Recebido: 12/03/2019
Accepted / Aceite: 10/06/2019
Publicado / Published: 17 de Março de 2020


{kind=link}
{kind=link}