










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkJornal Português de Gastrenterologia
versão impressa ISSN 0872-8178
J Port Gastrenterol. vol.20 no.3 Lisboa maio 2013
https://doi.org/10.1016/j.jpg.2012.08.003
ENDOSCOPIC SPOT
A rare cause of rectal ulceration
Úlcera rectal de etiologia rara
João Dinis Silva ∗, Nuno Veloso, Rogério Godinho, Lurdes Gonçalves, Isabel Medeiros, Celeste Viveiros
Serviço de Gastrenterologia, Hospital do Espírito Santo de Évora, Évora, Portugal
*Corresponding author
Introduction
Prostate cancer is the most common neoplasm affecting men, with an estimated 4,000 new cases diagnosed each year in Portugal.1 Currently, curative treatment options for men with localized prostate cancer include radical prostatectomy, external beam radiotherapy (EBRT) and prostate brachytherapy (BT) with permanent interstitial implants. This later modality is being increasingly used because it provides similar disease control with lower rates of incontinence and sexual dysfunction. However, it can lead to chronic radiation proctitis, because of the close proximity between the rectum and the implanted prostate.2 The main manifestations of chronic radiation proctitis are rectal bleeding, urgency, pain, strictures, mucous discharge and incontinence and they may take up to two years to develop. The association of BT with EBRT raises the incidence of proctitis from 1-19% to 39%.3
Treatment options include medical therapy (aminosalicylates, sucralfate, steroid enemas and hyperbaric oxygen), endoscopic therapy preferably with argon plasma coagulation (safer, less expensive and more widely available than heater and bipolar cautery, Nd:YAG laser and topical formalin) and surgery in cases of rectal strictures, fistula or in others not amenable to treatment with the previous options.
Rectal ulcers and fistula rarely occur (0.3-5.4%) but are the most feared complications of chronic radiation proctitis. Radiation dose administered to the rectal mucosa, the association with EBRT, previous transurethral resection of the prostate, diabetes, hypertension and inflammatory bowel disease are all risk factors.4 It has been shown that rectal ulcers have a favorable response to hyperbaric oxygen therapy with a partial or complete remission in at least half of the patients.5
Case description
The patient was a 59-year-old man, with a history of diabetes, and a prostate tumor formerly submitted to external beam radiation and brachytherapy. After six months of post therapy he developed tenesmus, rectal bleeding and pain that required daily analgesia for relief. In more than one occasion, he also needed to be transfused with blood units as an outpatient.
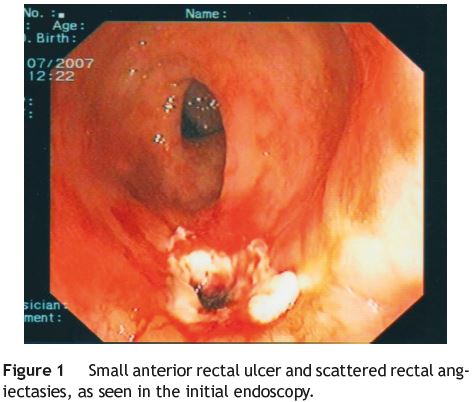
An initial diagnostic colonoscopy was performed, that revealed a small anterior rectal ulcer and scattered angiectasies in the distal 20 cm of the colon (Fig. 1). Treatment with mesalamine enemas was prescribed and argon plasma coagulation was subsequently performed in the bleeding lesions.
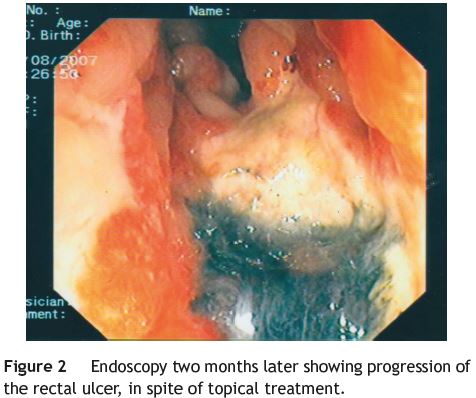
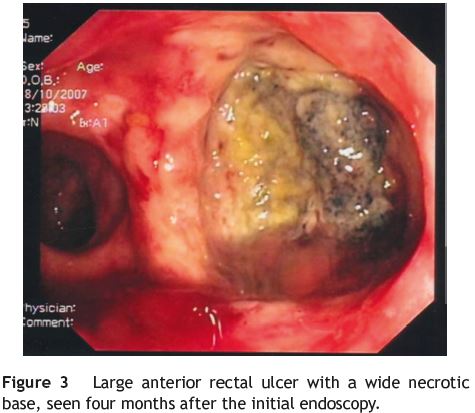
Follow-up endoscopies, two (Fig. 2) and four months later (Fig. 3), showed progressive resolution of the bleeding lesions, with both instituted treatments but no significant healing of the ulcer. In fact, it increased in size and became gradually deeper and wider with a necrotic base. At this time, the patient was referred to hyperbaric oxygen therapy that also proved ineffective.
Later on, he developed a rectovesical fistula that required an abdominoperineal resection of the rectum and the excision of the bladder and prostate.
References
1. Nunes P, Luís Pimentel F, Pina F, Rolo F. Registo nacional de cancro da próstata, em Portugal - ReNaCaP. Acta Urológica. 2010;3:39-45. [ Links ]
2. Phan J, Swanson DA, Levy LB, Kudchadker Rajat J, Bruno Teresa L, Frank Steven J. Late rectal complications after prostate brachytherapy for localized prostate cancer - incidence and management. Cancer. 2009;115:1827-39. [ Links ]
3. Mishra Mark V, Shirazi Reza, Barrett William L. Incidence and clinical course of hemorrhagic radiation proctitis after iodine- 125 prostate brachytherapy. Clin Genitourin Cancer. 2007;6: 397-400. [ Links ]
4. Budía Alba A, Bosquet Sanz M, Tormó Mico A, Boronat Tormo F, Alapont Alacreu JM, Francés A, et al. Braquiterapia de baja tasa en el tratamiento del cáncer de próstata localizado. Actas Urol Esp. 2007;31:452-68. [ Links ]
5. DallEra MA, Hampson NB, Hsi RA, Madsen B, Corman JM. Hyperbaric oxygen therapy for radiation induced proctopathy in men treated for prostate cancer. J Urol. 2006;176:87-90. [ Links ]
Conflicts of interest
The authors have no conflicts of interest to declare.
*Corresponding author.
E-mail address: jdinisilva@gmail.com (J. Dinis Silva).
Received 25 January 2012; accepted 9 July 2012

{kind=link}