











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Improving quality presents itself as a challenge for all health professionals, including nurses. The identification of quality indicators of professional practice that highlight the health gains sensitive to nursing care is an area that must be developed (Virdun, Luckett, Lorenz, & Phillips, 2018). There is a growing concern to the construction and validation of indicators that can assess the quality of nurses’ practice. The quality evaluation through indicators is considered as an essential strategy to assure a safety environment (Silveira, Júnior, Siman, & Amaro, 2015; Santos, Lima, Hora, & Leão, 2020).
In Portugal, the majority of care provided to people in a situation of dependency, with chronic illnesses, with some type of disability, frailty, or other long-term health condition is provided by informal caregivers (Teixeira et al., 2017). Given the need of a closer care to people in situations of dependency and the increasing pressure to provide social and health care due to aging of population, the creation of a network to provide long-term care, social support and palliative care was approved by the Portuguese government (Decree-Law, 2006). This network provides services in the following areas: convalescence (short-term recovery); medium-term care and rehabilitation; long-term care; palliative care; day care and autonomy promotion (Unit Mission for Integrated Continuous Care, 2011). The Integrated Continuous Care at Home Teams are one type of services provided by this network which directed their assistance to people with functional dependency, terminal illness or in a convalescence process, with a social support network, whose situation does not require hospitalization. The objective is to support the qualification of the caregiver and family of the dependent person (Unit Mission for Integrated Continuous Care, 2011).
According to this reality, it is important to enhance the work done by nurses, in this type of units, to help clients and their caregivers to the new role. Thereafter the quality indicators of professional practice assume great significance to clearly translate the health gains obtained by nurses (Cook & Horrocks, 2016).
The objective of the study was identify the indicators that nurses of Integrated Continuous Care at Home Teams consider adequate to monitor the quality of their professional practice in the ambit of the caregiver role.
1. State of art
Nowadays, quality is seen as a strategic component in most countries, regardless of their level of development. The Portuguese National Health Program operative until 2020 adopts the definition proposed by the Iberian Program (program aimed at developing joint strategies between Portugal and Spain in the area of quality) in 1990, which states that quality refers to the provision of accessible and equitable care, with a great professional level, taking into account the resources available and which enables clients adherence and satisfaction (Healthcare Ministry, 2015).
There are several studies about quality in healthcare, however it has been highlighted the work of Avedis Donabedian (Gardner, Gardner, & O’Connell, 2013). According to this author, the assessment of health quality can be seen as a three-dimensional paradigm: structure (the attributes of the scenario where care is provided); process (what is done in care) and outcome (the effects of care on the health of clients) (Donabedian, 2003; Santos et al., 2020).
There is a growing concern to demonstrate the effectiveness and efficiency of care in health and communicate these results to the organizations’ leaders (McCance, Telford, Wilson, MacLeod, & Dowd, 2011; Evangelou, Lambrinou, Kouta, & Middleton, 2018; Santos et al., 2020).
The indicators appear as an important tool for the development of the profession, and are considered as a succinct measure to describe a system, helping to understand it, compare it and improve it (Evangelou et al., 2018; Santos et al., 2020). Identifying indicators that are sensitive to nursing care is a challenge, however, it is at the same time an opportunity to demonstrate the nature of the contribution of nurses to the recovery of their clients (McCance et al., 2011; Evangelou et al., 2018; Santos et al., 2020). The same authors, regarding the report of the National Nursing Research Unit 2008 about the state of the art in nursing, refer that the majority of indicators reported in the literature focus quantifiable areas; in general, the indicators reported refer to the incidence and risk of pressure ulcers, falls, infections, medication errors, hand hygiene, nutritional status and presenting complaints; and, finally, that there is a lack of indicators that measure the broader impact of nursing care (McCance et al., 2011).
It is understandable that the use of quality indicators of professional practice may contribute to the renovation and modernization of care provided by nurses, by identifying areas for improvement.
According to the National Statistics Institute (2011) referring to the Census in 2011, in Portugal for every 100 young people there are 131 elderly (65 years old and over), with a raise in the dependency ratio of the elderly of 25 to 30% people of working age. In fact, there is an increase in the dependency levels, either by economic and social factors or by disease.
The majority of elderly people are integrated in their families and the lack of preparation of caregivers usually causes physical, social and emotional consequences either to the dependent person or to the caregiver. The caregiver can be understood as the person who "(...) assists with identification, prevention, or treatment of illness or disability; attends to the needs of a dependent." (International Council of Nurses, 2011, p.115). There are two types of caregivers: informal (family and friends) or formal (employed and paid individuals for that purpose, which care can be provided at home or in institutions) (European Commission, 2009). For the purpose of this study it was considered just the informal caregivers which are object of the intervention of Integrated Continuous Care at Home Teams nurses. These nurses must ensure the provision of care every day of the year, from 8 a.m. until 8 p.m. on working days and, as the needs, on weekends with minimum guarantee from 9 a.m. to 5 p.m., and should also provide telephone service to the user and/or caregiver. Clients of these teams are people in situations of dependency and their caregivers who need care in the following areas: nursing home care to preventive level, curative, rehabilitative and palliative care and also education activities for health (Unit Mission for Integrated Continuous Care, 2007).
2. Methods
The paradigm of this research is qualitative, with a descriptive and cross-sectional nature, since it was intended to explore and deepen these themes. A semi-structured interview was conducted in a focus group.
2.1 Sample
Participants were 11 nurses from three Integrated Continuous Care at Home Teams of the northern region of Portugal. These institutions were selected due to their previous participation in programs related to nursing information systems and quality improvement projects, being considered as privileged informants. These nurses work in a rural region with an increasing elderly rate and with high dependency levels. The average wage of the habitants of this region is inferior to the rest of the country, the access to public facilities and health institutions is harder, and the quality of home infrastructures is frequently much poorer.
Participants were selected through a non-probability sampling process.
2.2 Data collection instruments and procedures
Data was collected through a focus group, which is considered a rich technique because it allows group dynamics that facilitate individuals’ participation and to obtain a lot of information, exploring people's thoughts, ideas, attitudes, and experiences in relation to a particular topic, especially in sensitive areas such as nursing (Silva, Veloso & Keating, 2014). The focus group interview lasted 2 hours and 10 minutes, referring to what is advocated in the literature, in which the duration can vary between an hour and a half to two and a half hours (Silva, Veloso & Keating, 2014).
A semi-structured interview guide was developed, addressing the main questions: with regard to the caregiver which are the main nursing intervention areas? What is your opinion about the use of quality indicators of professional practice of nurses? Which quality indicators of professional practice of nurses do you use in the ambit of the caregiver? Which are the advantages for the clinical practice with the use of quality indicators of professional practice of nurses?
The interview was recorded on audiotape.
2.3 Content analysis
The interviews were transcribed and after that were submitted to content analysis. They were first analysed by the first author and then by the second and third authors. The content analysis according to Bardin was used as it focuses on mixed messages, allowing to methodically and systematically process information and evidence with a certain degree of depth and complexity (Quivy & Campenhoudt, 2019).
2.4 Procedures
To respect the ethical principles the agreement of the Ethics Committee for Health of the Northern Health Authority of Portugal, the National Data Protection Committee, and also the Executive Director and Nurse Administrator responsible for the three Integrated Continuous Care at Home Teams involved was requested and received. All participants signed an informed consent model. Regarding the data analysis, codification was used for identification purposes in order to remain anonymous (interviewed from 1 to 11 = E1, E2, ...).
3. Results and dicussion
Nurses aged 30 to 53 years (M=44years; SD=8.49years). The length of their professional activity varied between 7 and 31 years. With regard to the length of professional activity in the Integrated Continuous Care at Home Teams, this ranged between two and five years. These data reflect the recent creation of such units, promulgated in 2006. Of the 11 participants in the study, 90.9% (n=10) were female. Concerning the professional category, 18.2% of nurses (n=2) were generalists, 45.5% (n=5) were specialists, 27.3% (n=3) were head nurses and 9.1% (n=1) was an administrator nurse. Nine nurses had a specialization qualification in nursing and one had a master degree in nursing.
After detailed analysis of the nurses’ speech, two thematic areas were identified: Process indicators and Outcome indicators. These thematic areas lead to the Donabedian’s model so it was decided to organize the content analysis considering this model. To Donabedian (2003), the triad, structure, process and outcome, its intuitive nature and its simplicity, has been widely broadcasted and accepted. He states that the structure, the process and the outcome are related to each other and that inferences about the quality are not possible unless we keep in mind this relationship. The structure influences the process, and the process influences the outcome in a complex reality, with causes and effects, wherein each of them has its functions and limitations.
Structure indicators will not be target of study, since these are not consistent with the objectives previously defined for research. This decision is consolidated with the nature of the structure, which refers to conditions in which care is provided, including material resources, human resources and organizational characteristics (Donabedian, 2003).
To organize findings, data was grouped in process indicators and outcome indicators and only some examples of each will be presented.
3.1 Process Indicators
Process in Donabedian's triad, refers to the activities that constitute the health care provided by professionals (including diagnosis, treatment, rehabilitation, prevention and customer education) but also takes into account the client's own contributions and respective family (Donabedian, 2003).
Aiming to help customers to achieve maximum health potential, nurses play a key role in identifying their needs of health and also promotion and prevention of complications. Nurses recognize the potential of health education and the use of learning strategies in interaction with clients (Portuguese Nurses Association, 2012).
Teaching represents an important area of nursing intervention, since it helps in the acquisition and modification of clients’ behaviors. In the Andrade (2009, p. 68-69) study it was stated that the activities developed by nurses with the caregivers consisted of "(...) information, counseling, support, training of technical skills to the provide care (...)."
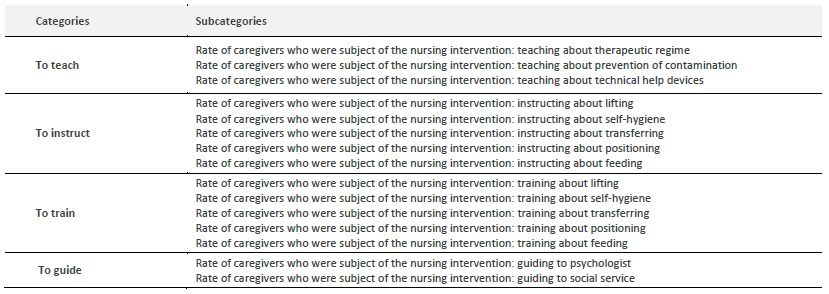
To clarify the data we highlight the following examples:
Rate of caregivers who were subject of the nursing intervention: teaching about therapeutic regime
We have an action in terms of management of the therapeutic regimen. (...) We try to educate and sensitize the caregiver to participate in the management of therapeutic regime and explain the implications that non-cooperation may have. (...) Home visits always have an educational component to the family and to the caregiver."E1.
Rate of caregivers who were subject of the nursing intervention: instructing about self-hygiene
We instruct the caregiver on how to provide hygiene care to the patient. E2.
Rate of caregivers who were subject of the nursing intervention: guiding to psychologist
We have our psychologist. We guide to him, and he does the visits with the frequency he considers adequate, and sometimes it helps the caregivers. It depends also on the characteristics of the caregivers. E1
Process indicators are considered current, which means, it refers to care that is happening at the moment, aiming immediate indications about the quality of care and are easily obtained (Donabedian, 2003).
In this context, emerged four categories "To teach", "To instruct", "To train" and "To guide" and 15 subcategories (Table 1).
3.2 Outcome Indicators
The outcome, in the Donabedian’s model, regards to changes (desirable or undesirable) in individuals and in population, which may be attributed to health care, including changes in health status, and changes in behavior and knowledge acquired by clients and respective family, which may influence care provided (Donabedian, 2003).
Scientific evidence points towards the preparation of the caregiver to play their role through knowledge and learning skills of the areas inherent to the satisfaction of the dependent person's needs. It has been referenced indicators as gains in knowledge and learning skills by the caregiver. This type of indicators provide guidelines to nurses for the promotion of the caregiver adaptation to the new role, especially in what concerns to the “know and know-how” giving and adequate response to their needs (Petronilho, 2008).
The preparation of the caregiver should not only focus on education and support but also in an interactive component that encourages the involvement and the interest in the new role (Brookman, Holyoke, Toscan, Bender, & Tapping, 2011).
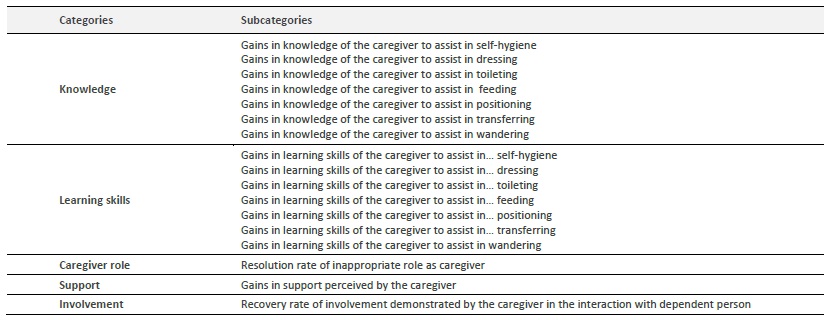
To clarify the data we highlight the following examples:
Gains in knowledge of the caregiver to assist in self-hygiene
It is important for us the percentage of caregivers with knowledge shown in a specific area that previously didn’t exist. For instance, knowledge about self-hygiene that previously didn’t exist and that after sometime was acquainted. E3
Resolution rate of inappropriate role as caregiver
I think that the performance of the caregiver should be evaluated. E1; We can have the indicator resolution rate of inappropriate role as caregiver. E4; Our intervention is to obtain gains within the caregiver. E3
Gains in support perceived by the caregiver
As we [nurses] are available and concerned with the patient, I think the caregiver feel support from us. E7; There has to be something to measure it; our availability all the time, our resolution of problems on time. E3; Perception of nursing support for the role of caregiver. We have a nursing diagnosis like this. E4.
Outcome indicators have been related to consequences of care, reflecting not only the care provided but also its efficacy (Donabedian, 2003).
In Table 2 are presented the categories that emerged from the speech of participants, as well as the respective subcategories related to this subject area.
The indicators that nurses of the Integrated Continuous Care at Home Teams believe are most appropriate for monitoring the quality of their professional practice in the ambit of the caregiver focus mainly on the acquisition of cognitive and instrumental skills necessary to meet the needs of the dependent person, essentially regarding self-care, which is consistent with previous studies (Pereira, Paiva e Silva, Mendonça, & Delaney, 2010). Due to this study, 32 quality indicators of professional practice of nurses emerged from the speech of the participants. According to these results the importance of knowledge and learning skills were highlighted, translating the majority of the indicators and enhancing the relevance of nursing interventions in the dimension of “informing”. These results can be explained by the area of care of these professionals, which focuses on education not only of the caregiver, but also of the dependent person and respective family.
The use of quality indicators of professional practice of nurses can establish itself as an extremely useful tool to monitor the quality of care (Cook & Horrocks, 2016; Evangelou et al., 2018; Virdun et al., 2018; Santos et al., 2020). It is essential that the use of indicators does not focus only in an evaluative nature, but also in a reflective nature and change of practices, increasing their use in professional development and improvement. Avoiding that it is associated with a purely evaluative and punitive character.
The Integrated Continuous Care at Home Teams have been promoting interdisciplinary care, which address the diverse needs of its clients in home context. The high number of older people with chronic and disabling disease, associated with increased life expectancy, has generated numerous difficulties with regard to meeting the needs of these users and their families, since there are lacks of community resources to meet their needs.
Currently there is at least one dependent person within many Portuguese families. Mostly the preparation of the homecoming of the patient, as well as the preparation of the caregiver to assume the new role is quick and performed in a hospital setting, so a support network is not always guaranteed to deal with any difficulties that the family may confront at home. It is essential to analyze the care provided at home by caregivers to improve their skills as well as to develop a relationship with patients and their caregivers, in order to understand the relationships between them and the concepts related to care experiences, which allows nurses meet the needs of caregivers and support them in providing care (Cook & Horrocks, 2016). Considering the context in which nurses of the Integrated Continuous Care at Home Teams who participated in this study carry out their functions, an essentially rural environment and with few resources, it is essential to make clear health gains obtained through the care provided by these professionals, because only in this way it can be demonstrated the important role of nurses.
Conclusion
The quality in health is assumed as vital in ensuring that health care meets clients’ needs. The need for evaluation of care provided to clients by organizations has been encouraging the progressive use of indicators in all areas and at all levels of care.
The nurses from this study consider 32 indicators to monitor the quality of their professional practice in the ambit of the caregiver. Those indicators are mainly related with positive evolutions in knowledge and abilities of the caregiver and point the health gains sensitive to nursing care.
Since the research was developed with a very specific population and with very particular necessities, it is advisable to replicate the research in other contexts (whether in a rural setting or in an urban environment), in the interest of consolidate or refute the obtained results. It is also essential more studies in this field in order to highlight indicators of professional practice of nurses in process and outcome basis that can translate the autonomous nursing gains in health.
One limitation of the study is the fact that there was only one focus group, but the participants were from different health care centres.

