











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
In Portugal, 94% of women of childbearing age use a contraceptive method, with oral hormonal contraceptives the method of choice (76%) (DGS, 2018). However, 84% of them acknowledge that they have already forgotten to take the pill and 47% intend to change their method to one that does not require daily use, such as long-term reversible contraception (Bayer, 2017).
Currently, young people start their sexual activity earlier and have later maternity projects (Magalhães, 2007; Águas, Bombas & Silva, 2016), which leaves them more exposed to the risk of an unplanned, unwanted pregnancy, infections sexually transmitted diseases and the voluntary interruption of pregnancy. According to the Report on the Records of Voluntary Pregnancy Interruptions, the total number of pregnancy interruptions by the woman's choice in the first 10 weeks was 14 899, 96.2% of total abortions performed in Portugal in 2018 (DGS, 2018). Regardless of the reasons given for a voluntary interruption of pregnancy, what is at its origin is non-adherence to contraceptives, discontinuity, incorrect use and unmet needs for family planning (Águas, Bombas & Silva, 2016; Palma, 2017). When asked, women are able to list several contraceptives, but with little knowledge about them, and this information is based on beliefs and internet research (Greene, Joshi, & Robles, 2012; Matias, 2015; Águas, Bombas & Silva, 2016; Palma, 2017).
There is a perceived need to promote contraceptive counselling as a way to protect women from experiencing an unplanned and unwanted pregnancy, which can expose them to difficult economic and family situations. Prevention is an important line of intervention in the context of promoting health. There is a deficit in contraceptive decision making related to beliefs, cultural aspects, poverty, poor health literacy, difficulty in access to services and to health professionals and services, such as low availability, inefficient service response (OE, 2011) and lack of preparation on the part of professionals (OE, 2011; Bellizzia, Nagaic & Sobel, 2020; Palma, Presado & Ayres-dos-Santos, 2021).
In a literature review (Palma, Taborda, Nunes, Cardoso, & Presado, 2020), we found that quality contraceptive counselling favours adherence to contraceptive methods in general, and in particular to long-term reversible methods, which are considered the most efficient. Health professionals do not always provide counselling and when they do, it is very heterogeneous, the available resources influence the quality of response of professionals and services, which are often adapted to the individual case. The quality of counselling depends on the professional's qualifications and counselling should be centred on the needs of women (Palma, Taborda, Nunes, Cardoso, & Presado, 2020; Palma, Presado & Ayres-de-Campos, 2021).
Internationally, since the 1990s, there has been a concern with the quality of care in family planning motivated by a recognition that the women’s positive experiences with health professionals are essential for choice and adherence to a contraceptive (Holt et al., 2019). They are also essential for promoting trust in the health system (Kruk et al., 2018; Holt et al., 2018). Portuguese law states that family planning consultations and distribution of contraceptives are free in the national health system. However, there are accentuated regional inequalities in terms of access, which means the most disadvantaged, in addition to unmet needs for family planning, lack of information, poor adherence to consultations for contraceptive counselling, use of less effective methods or incorrect/discontinued use (Presado, Palma & Cardoso, 2018; Palma, 2017; Águas, Bombas & Silva, 2016).
Promoting quality contraceptive counselling, which promotes women’s literacy in decision-making and adherence to adequate contraception for their needs is paramount. This issue led us to conduct a survey to measure the quality of care in contraceptive counselling. To this end, our research focused on the Quality of Contraceptive Counselling Scale, 22 Items (Holt et al., 2018) as it met our requirements.
Studies carried out by Holt and his colleagues (Holt et al., 2018), found that providing high quality contraceptive healthcare is based on communication between the person receiving care and the healthcare professional. This interaction should be based on the exchange of information and interpersonal relationships (Holt et al., 2019). These researchers conducted studies in order to learn about best practices in contraceptive counselling, health communication and respect for human rights (Holt, Dehlendorf & Langer, 2017). Consequently, they developed the Quality of Contraceptive Counselling Scale (QCC) in order to assess the interaction of the person’s experiences with health professionals during quality contraceptive counselling (Holt, Dehlendorf & Langer, 2017).
The aim of this study is to adapt the QCC culturally and to assess the psychometric qualities of the Portuguese version of the QCC, i.e. the QCC-PT. Research Question: To what extent will the QCC-PT have adequate psychometric qualities to assess the quality of contraceptive counselling?
1. Methods
We started by requesting permission to translate, adapt and validate the QCC Scale to the Portuguese population, from the author, Kelsey Holt from the University of California at San Francisco. Permission was received on 18 June 2020. We then employed the translation/retranslation methodology (Beaton, Bombardier, Guillemin, & Ferraz, 2000), which comprises six stages: translation, synthesis, retranslation of the questionnaire (back translation), review by a committee of experts, pre-test and verification of the psychometric properties.
1.1 Translation from English to Portuguese and linguistic adaptation.
The QCC Scale was translated from the original language (English) to Portuguese while preserving the same meaning as the original version. We used two translators who did not know each other. The professionals contacted are fluent in the source language (English) and native speakers in the target language (Portuguese) and they had no prior contact with the scale. Our aim was to create two independent translations, even though one was knowledgeable about the objectives and concepts studied. One is an English teacher, the other a health professional.
1.2 Synthesis of the translations with the translators, resulting in a single version of the instrument.
At this stage and working with both translators, it was possible to obtain a linguistically correct Portuguese version, equivalent to the original English version. A report was produced in which we described all the differences that arose and how they were resolved by everyone involved. The new instrument was called QCC-PT (Quality of Contraceptive Counselling Scale - Portuguese Version. Escala de Qualidade de Aconselhamento Contracetivo, in Portuguese).
1.3 Retranslation of the questionnaire (back translation).
For this, two additional translators were selected and contacted by telephone. They were not familiar with the original version of the instrument, did not know the concepts under study and had not participated in the first translations. As advocated by Beaton, Bombardier, Guillemin, & Ferraz (2000) at this stage, the translators’ mother tongue must be the same as the original version of the instrument (English). These translators were both English-Portuguese teachers.
The retranslations were returned, one by email and the other hand-delivered and were named R1 and R2. After receiving the retranslations, their compatibility was checked, resulting in a single retranslation version (R3).
1.4 Review by an expert committee.
The members of the expert committee were intentionally and personally invited. They were all aware of the purpose of the scale, the concepts therein and the source language. The original version and the QCC-PT and R3 instruments, together with the corresponding written reports, which allowed them to explain their decisions. The data were analysed descriptively since notes were taken regarding the terms decided on by the committee until a consensus was reached.
Thus, it was possible to reach an agreement on any discrepancy, to establish semantic, idiomatic, experimental, cultural and conceptual equivalences, resulting in the final version to be tested. The experts are all bilingual and one of them is one of the re-translators (an English teacher), another is an expert in contraception (a nursing teacher) and a nurse specializing in maternal health and obstetrics (one of the translators).
1.5 Application of the QCC-PT scale in a pilot test.
The aim of this stage is to assess the equivalence between the original and final versions, which will provide understanding, clarity of the scale questions (Vilelas, 2020) and perceptions of deviations or errors in the translations (Oliveira, Hildenbrand & Lucena, 2015). We applied the pilot test to 30 women from the target population in the pregnancy interruption consultation at a central hospital in the Lisbon and Vale do Tejo area in August 2020.
The study was approved by the Ethics Committee and the Board of Directors of the hospital on 24 July 2020.
1.6 Sample
A convenience sample was used. Invitations were made by personal contact to all women aged 16 or over, who could read and write and were fluent in Portuguese at the end of the contraceptive counselling consultation and who wished to participate in the study. All others that were not included in the eligibility criteria were excluded.
Each woman completed the questionnaire and was interviewed in order to perceive the clarity and adequacy of the questionnaire through the meanings attributed to each item and the degree of difficulty in understanding the questions. The objective of this step was to obtain knowledge regarding the understanding of the data collection instrument. We concluded that 97% of women did not show any difficulty in understanding or ambiguity in interpreting the questions. When interviewed, they reported that the questionnaire was clear and easy to understand. The difficulties expressed and felt were related to the language barrier and illiteracy.
According to the authors (Beaton, Bombardier, Guillemin & Ferraz, 2000), if agreement of answers is equal to or greater than 80%, it is not necessary to re-check the instrument with the expert committee. Thus, the final version of the QCC-PT instrument was generated. The QCC-PT consists of 22 items that are divided into three dimensions: Information Exchange (IE), with ten items; Interpersonal Relationship (IR) with seven items; and Disrespect and Abuse (DA) with five items.
1.7 Validation of the QCC-PT Scale.
The psychometric qualities of the QCC-PT, which were assessed through the validity and reliability (Coutinho, 2014) of the scale and its three dimensions individually in a sample of 200 women. The response rate was 86%, resulting in a final sample of 172 questionnaires (n=172), between August and November 2020 using the same inclusion criteria as the pilot study.
Analysing the responses QCC-PT, eight questionnaires were eliminated as they were not correctly filled in (duplicate responses or no response), without verifying a pattern in the responses given, nor in the type of participants. Data analysis to assess the psychometric qualities of the QCC-PT was performed using the R® Software (The R Project for Statistical Computing) (R Core Team, 2020), more specifically, the estimation of the factorial model was performed using the “Lavaan” Package (Latent Variable Analysis) Version 0.6-7 (Yves Rosseel, 2012).
The analysis of the sensitivity of the items was evaluated using the asymmetry (g1) and flatness (g2) coefficients, considering that the items with absolute values, no higher than 3 and 7 respectively, do not deviate from normality; that is, they have psychometric sensitivity (Marôco, 2014; Curado, Marôco, Vasconcellos, Gouveia & Thoyre, 2017). Construct validity was assessed using factorial and convergent validity, using confirmatory factor analysis, with robust weighted least squares (RWLS) estimation. For the QCC-PT Scale to be considered valid, we consider that all the constituent items should have factor weights above the reference value (0.40). The quality of the model’s fit to the data was assessed using empirical indices: Chi-square test statistics of fit (χ2/df) < 5, Comparative Fit Index (CFI) and Tucker Lewis Index (TLI) greater than 0.9 Root Means Square Error of Approximation (RMSEA) less than 0.05. The reliability of the created dimensions was estimated using Cronbach’s alpha considering an acceptable reliability if α ≥ 0.70. The composite reliability (CR) and the mean extracted variance (MEV) were calculated as indicators of convergent validity, where CR ≥ 0.70 and MEV ≥0.50 (Marôco, 2014).
The reliability estimate was based on the mean correlations between QCC-PT items, weighted by the respective variances. Reliability was considered acceptable if ᾳ ≥ 0.70. We also consider a composite reliability (CR) ≥ 0.70 and an extracted mean variance (AVE) ≥ 0.50 as indicators of convergent validity. With regard to discriminant validity, we considered that it was present for factors in which the VEM was greater than the square of the correlation between factors (Marôco & Garcia-Marques, 2006; Marôco, 2014).
In the first phase of the study, the factorial model of the QCC-PT, consisting of three dimensions and 22 items, adjusted to the sample of 172 women, presented poor quality of adjustment values (χ2/df = 2,566; CFI= 0, 869; TLI= 0,853; RMSEA = 0,097, P(RMSEA ≤ 0,05) < 0,001 . So, the initial model was refined.
Items 2, 3, 4, and 10 were removed from dimension one (Information Exchange). It initially had 10 items and now has 6. Items 13 and 14 of dimension two (Interpersonal Relationship), from seven initial items, it is now composed of 5. In the third dimension (Disrespect and Abuse), item 18 was removed, with four items remaining in the end, having had 5 initially. There was a need to refine the initial model because they presented sensitivity problems with high skewness values and kurtosis coefficients (|g₁|>3 e | g₂| >7) and low factorial weights (< 0,4).
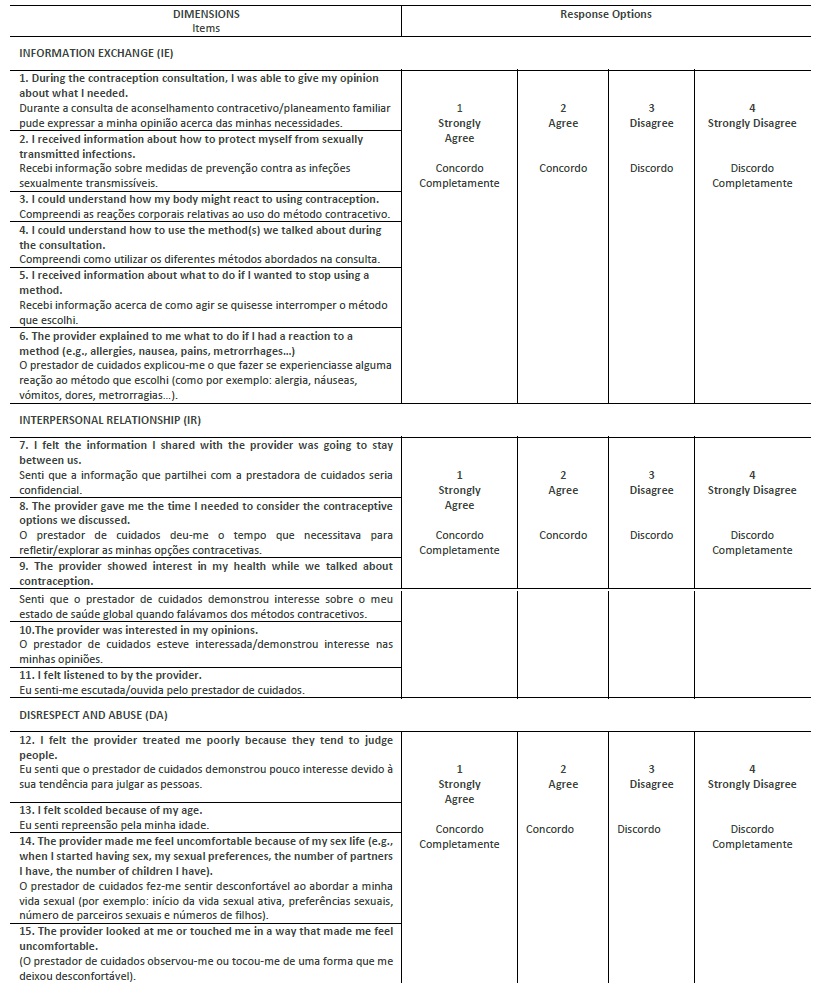
The modified QCC-PT scale consists of 15 items and three dimensions: Information Exchange (IE), with six items; Interpersonal Relationships (IR), with five items; and Disrespect and Abuse (DA), with four items. The IE dimension reflects the information that women are given about contraceptive methods and follow-up options, as well as the information they share with healthcare professionals about their preferences and needs. The IR dimension covers items related to privacy, confidentiality, respect, trust and empathy and the DA dimension includes the way health professionals treat women, discrimination and physical abuse (Table 1).
2. Results
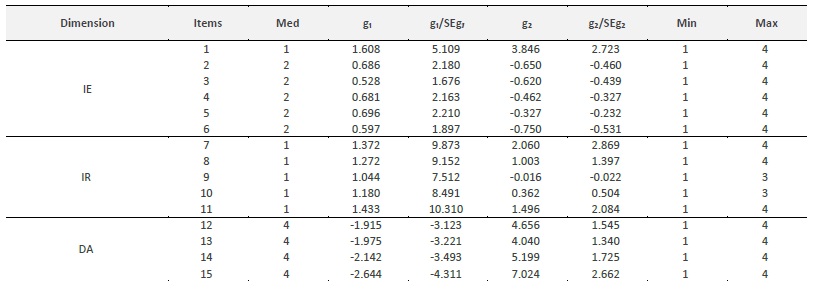
The psychometric qualities of the modified QCC-PT were evaluated by calculating the sensitivity, robustness and reliability of the items of the three dimensions of the scale for a sample of 172 women who were included in the previously established eligibility criteria. The women were aged between 21 and 30 years, were mostly Portuguese, single and with secondary education. In table 2, the following statistical results of the items on the QCC-PT scale are presented: medians, maximums, minimums, shape measures (g₁ and g₂), as well as their critical ratios.
Table 2 Median, maximum, minimum, shape measures (asymmetry - g₁ and kurtosis - g₂), with the respective critical ratios (g₁/SEg₁ and g₂/SEg, for the 15 items of the QCC-PT scale (n=172).
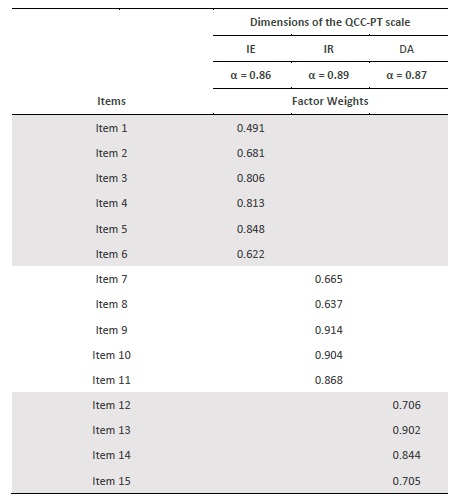
The factorial weights of each dimension of the QCC-PT scale and the Cronbach’s Alpha per dimension are presented in table 3. The internal consistency of the IE dimension presents Cronbach’s Alpha values = 0.86, less high than the IR dimension (Cronbach’s Alpha = 0.89) and the DA dimension (Cronbach’s alpha = 0.87). The CR in the three dimensions is: CRIE = 0.863; CRIR = 0.901 and CRDA = 0.87. The convergent validity estimated through the VME ranges between (IE) 0.52; (RI) 0.65 and (DA) 0.629. All values are above the reference.
Table 3 Factor weights obtained through confirmatory factor analysis and internal consistency (Cronbach’s alpha) of the three factors of the QCC-PT
The correlations between IE and IR and between DA and IR are of medium magnitude and the correlation between DA and IE is negligible, as shown in table 4.

There is a negative correlation between the DA dimension and the other two, which was to be expected. This fact is related to the way the questions are formulated in the DA dimension.
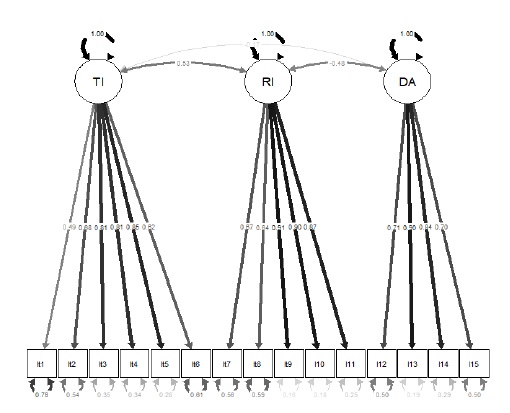
Figure 1 shows the models with the three factors of the QCC-PT with the respective factor weights and goodness-of-fit indices that support the dimensions of the scale (Figure 1).
3. Discussion
Using the conventional methods of translation and adaptation of questionnaires, it was possible to develop a version of the QCC scale adapted to the Portuguese reality - the QCC-PT scale. In the first stage of the study, the factorial model of the QCC-PT, consisting of three dimensions and 22 items, adjusted to the sample of 172 women, presented poor quality of adjustment values (χ2/df = 2,566; CFI= 0,869; TLI= 0,853; RMSEA = 0,097, P(RMSEA≤ 0,05) < 0,001. The initial model was thus refined.
The reliability of the three dimensions of the QCC-PT presents good Cronbach’s Alpha values, and it can be said that the scale presents good internal consistency with a standardized alpha higher than the reference. For CR we considered values above 0.70 as a good reliability indicator, which was observed in this scale (CRIE = 0.863; CRIR = 0.901 and CRDA =0.87). Convergent validity, assessed through average extracted variance (AEV) presented values above the reference values (AEVIE = 0.52; AEVIR = 0.65 and AEVDA =0.629).
Of the three dimensions of the scale, only IE and IR, which are positively correlated with correlations of moderate intensity and statistically significant (p<0.001). The correlation between the DA and IE dimension is negative and negligible, i.e., only statistically significant at the 5% level (p = 0.044) and the correlation between DA and IR is moderately negative and statistically significant (p < 0.001). The negative relationships are due to the way in which DA issues are formulated in relation to IE and IR issues.
The final adjustment of the QCC-PT model is good with all factor weights above the reference value (0.40) and the goodness-of-fit statistics showing good values (χ2(87) = 174,756; p < 0,001; n = 172; χ2/df = 1,698; CFI = 0,959; TLI = 0,951; RMSEA = 0,064, P[rmsea ≤ 0,05] > 0,10). Thus, as shown in figure 1, dimension 1 with 6 items, 2 with 5 and 3 with 4 items, allows us to conclude that this scale has factorial validity, sensitivity and reliability in the sample.
The QCC-PT contributes to assessing women’s experiences with health services and professionals during contraceptive counselling. With this scale, health professionals can assess and propose improvements in the quality of contraceptive counselling provided to women receiving care. This assessment is carried out in three dimensions: information exchange, interpersonal relationships, and disrespect and abuse. The QCC scale, developed by North American researchers and applied in Mexico, provides steps for high quality contraceptive counselling that respect the principles of human rights such as privacy, confidentiality, non-discrimination, as well as concepts of communication in health including respect, empathy and trust. Considering the great importance of this type of instrument, the scale was applied to a group of Portuguese women in its modified version and has adequate sensitivity, reliability and factorial validity, so it can be considered an instrument that should be used, not only in its practical component during contraceptive counselling, but also in research. The adjustment of the factorial model allows us to propose a modified version of the instrument (QCC-PT), to be used to identify problems and propose adjusted interventions and in partnership with the women receiving care.
Conclusion
The purpose of contraception is to protect women from unwanted pregnancies. The quality of contraceptive counselling is essential to ensure that these pregnancies occur less often. It is known that a large number of women who undergo a voluntary interruption of pregnancy were using contraception, which denotes the existence of flaws in the counselling provided by health professionals. The choice of a contraceptive must be based on knowledge and the main source of information is based on quality contraceptive counselling that guarantees women’s rights, sociocultural and economic aspects, promotes and respects choice, proper use and continuity of the selected method. We consider it essential to know how women perceive the counselling given to them in order to suit their individual reproductive needs.
We found a lack of Portuguese studies that assess the quality of contraceptive counselling provided to the population, which is why we consider validation and cross-cultural adaptation of the QCC-PT to be pertinent, as it allows us to assess the three most important dimensions of the quality of contraceptive counselling: information exchange, interpersonal relationships, and disrespect and abuse. The scale allows the assessment of women’s experiences during contraceptive counselling. Thus, it is an important instrument to assess and improve this care in Portugal.
Limitations in the validation and cross-cultural adaptation of the QCC Scale for the Portuguese Population
There were aspects that we considered interesting to investigate, but that were not considered in this context, including cultural influences, educational level and the women’s age.
Implications for practice and research
We believe that it is imperative to apply the QCC-PT to different epidemiological and clinical contexts, not only in the voluntary interruption of pregnancy, but also in contraception/family planning and school health consultations so that contraceptive counselling interventions focused on women will be implemented. This scale also contributes to the development of research aimed at quality care in terms of sexual and reproductive health. It is also suggested that professionals and managers of health units become aware of the issue of contraceptive counselling as a factor that promotes good care practices.
Author contributions
1. Conception, project: Sara Palma, Helena Presado, Diogo Ayres-de-Campos;
2. Data analysis and interpretation: Sara Palma e Helena Presado;
3. Article writing and relevant critical review of the intellectual content: Sara Palma e Helena Presado;
4. Final approval of the version to be published: Sara Palma, Helena Presado, Diogo Ayres-de-Campos.

