











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Ewing’s sarcoma is a malignant bone tumor composed of small squamous cells. Although rare, it is the second most common cause of primary bone tumors (Grünewald et al., 2018). It mainly affects children and young adults, and current estimates indicate 1.5 cases per one million children and young adults among the European population (Ebrahimpour et al., 2020). Males are slightly more affected than females, in a 3:2 ratio (Grünewald et al., 2018).
The presence of Ewing’s sarcoma within the ribs is uncommon, at only 12% of cases (Cotteril et al., 2000). In 80% of cases, the tumor is located at the time of diagnosis, which improves prognostics. Treatment of Ewing’s sarcoma is performed with chemotherapy combined with local surgical resection and/or radiotherapy, when appropriate (Gaspar et al., 2015). Some of these treatments cause acute and chronical adverse effects which compromise the quality of life of surviving patients (Grünewald et al., 2018).
The pathology’s rarity, its location, and occurrence in a female adult means very few cases have been reported and published. The lack of specific symptomatology may lead to a significant delay in diagnosis and treatment, with consequent implications to the patient’s survival. The evolution of treatments has made it possible to extend the life expectancy of these patients, which in turn results in a specific clinical follow-up throughout several years. Therefore, the publication of this article aims to raise awareness on the existence of this pathology, the need to perform an early diagnosis and treatment, and how to continue the clinical follow-up after treatment.
1. Case description:
1.1 History of present illness
39-year-old female, caucasian, accountant.
The patient is part of a nuclear family in stage I of Duvall’s family cycle, of upper-middle socioeconomic class according to the adapted Graffar scale.
As personal precedents, the patient mentioned being followed-up in breast care appointments for hamartoma in the outer upper quadrant of the left breast, diagnosed via biopsy in 2015. Moreover, the patient presented active problems related to an anxiety disorder, under surveillance since 2015 and chronic gastritis without metaplasia with Helicobacter pylori-negative in 2019.
No prior history of pregnancy and uses subcutaneous progestative implant as contraceptive. No alcohol, tobacco or drug use. No relevant family history of disease.
On February 25, 2021, the patient requests an open appointment via e-mail at the local medical health center with complaints of chest pain. At the appointment, anamnesis was conducted and the patient presented chest pain in the lower region of the left breast, aggravated with movement, that had begun after some strain performing household activities. No respiratory complaints, no pain on local palpation and no changes in cardiopulmonary auscultation. Considering the assessment, a clinical condition of muscular strain was assumed and the patient was prescribed analgesics and anti-inflammatory drugs.
On June 7, 2021, the patient requests another open appointment at the medical health center with complaints of pain in the left hemithorax. The anamnesis identified that the discomfort located at the left base of the thorax remained throughout the prior 3 months, and that the patient was periodically taking the prescribed analgesic medication with partial relief of pain.
The patient noticed an aggravation of the chest pain in the two weeks prior to the appointment, mainly during the night, waking her up from her sleep. Moreover, the patient mentioned dyspnea and left lateral and dorsal decubitus pain when inhaling deeply. At this moment, the pain was not correlated with movement or strain and occurred even during her resting time. It presented a migratory nature between the anterior and posterior region of the left hemithorax. The pain was relieved with analgesic medication and when on orthostasis. The patient denied any history of fever, coughing or other respiratory symptoms. The patient’s clinical history excluded the existence of local trauma.
On the objective examination, the patient was conscious, cooperative and showing adequate space and time orientation. She was hemodynamically stable with a blood pressure of 127/63 mmHg, heart rate of 66 beats per minute, and no fever (axillary temperature of 36.5 °C). Eupneic on ambient air with a peripheral oxygen saturation of 98% and respiratory rate of 15 cycles per minute. Rhythmic cardiac auscultation with no audible murmurs, and pulmonary auscultation with unaltered pulmonary sounds on both sides, though with a slight decrease of sound in the lower 2/3 of the left hemithorax. No visible deformities on thorax inspection, no change to the breasts, except for the small scar from the hamartoma’s biopsy. The patient felt pain on palpation of the lower region of the breast. Breast examination showed a palpable node on the outer upper quadrant of the left breast, in line with prior diagnosis, and stable against previous objective examination.
Considering the clinical condition, urgent chest and rib cage radiography was requested, which the patient performed the day after. The radiography identified an expansive lesion in the thorax, on left anterior position with modelling of pulmonary parenchyma. This can be observed in figures 1 and 2.
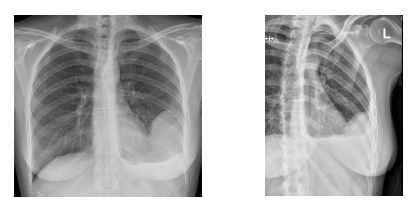
Figure 1 and 2 Thorax and left rib cage X-ray with left anterior expansive lesion modelling pulmonary parenchyma.
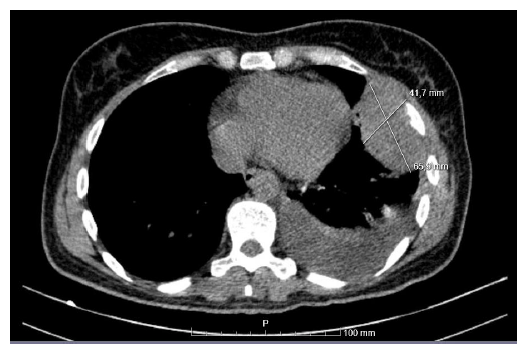
Given the imaging results, the patient was made aware by the radiology physician of the need to clarify the changes via chest CT scan. The patient received a prescription from the primary healthcare services on the same day and performed the diagnostic examination. The chest CT scan on June 8 showed hyperdense nodules, with 66x42x64 mm in the fifth left intercostal space in relation to the internal edge of the fifth left rib, together with bone thinning, where the rib showed a thinner thickness against the same rib on the opposite side. Figure 3 shows the CT scan slice with osteolytic lesion of the 5th rib and surrounding nodular formation.
Considering the results from the CT scan and the aggravation of pain, the patient was sent to the local Hospital’s emergency department with suspected tumor of the rib cage.
1.2 Evolution
After examination by a pneumologist, the patient was admitted to perform a biopsy of the suspected pleural nodular lesion. The histopathological result of the lesion with morphological and immunohistochemical appearance was compatible with Ewing’s sarcoma. The patient was later sent to the reference oncology center, where she currently keeps her follow-up appointments.
The subcutaneous progestative implant was removed at the primary healthcare services and later underwent chemotherapy cycles at the oncology center. Several infectious complications occurred during treatment resulting from pancytopenia caused by chemotherapy. One specific chemotherapy cycle was interrupted due to episodes of symptomatic bradycardia. On February 2022, the patient underwent expanded sarcoma removal from the 5th intercostal space with segmental resection of the 5th rib. Due to the presence of the tumor at the margins of the resection, the patient underwent surgical enlargement with complete costectomy of the 5th left rib in March 2022. Since the last surgical piece showed no signs of tumor at the margins, the oncology team considered there was no indication for complementing radiotherapy.
The patient is currently under surveillance at the oncology center and the primary healthcare services. She is in a rehabilitation stage, with local pain that is controlled via opioid analgesic medication and gabapentin, with imaging examination follow-up every three months.
2. Discussion
Ewing’s sarcoma is a malignant bone tumor composed of small squamous cells. Although rare, it is the second most common cause of primary bone tumors, after osteosarcoma (Grünewald et al., 2018).
It mainly affects children, teenagers and young adults, with an incidence peak at 15 years of age. The incidence is also greater in male children and male young adults, with less occurrences among adult females (Grünewald et al., 2018). The current estimates indicate 1.5 cases per one million children and young adults among the European population, with a greater incidence in comparison to both the Asian and African populations (Ebrahimpour et al., 2020). Despite being Caucasian and having European origins, the patient showed a lower probability of developing Ewing’s sarcoma due to being a female adult.
According to the European Intergroup Cooperative Ewing's Sarcoma Study (EICESS), the most frequent primary locations for this tumor are the hip bones (25%), the femur (16,4%), the leg bones (tibia 7,6% and fibula 6,7%) and the ribs (12%) (Cotteril et al., 2000). Ewing’s sarcomas in the ribs are significantly larger when compared with other locations (Shamberger et al., 2000), which is in line with the massive tumor reported at 66x42x64 mm.
On a clinical level, most Ewing’s sarcoma patients present local and region pain and local edema. Pain can be intermittent, occurring for several consecutive months and possibly aggravated during the night period. Intensity can be light to moderate at first, but a sudden aggravation is possible, as described in this clinical case (Grünewald et al., 2018). Pain aggravation and duration, as well as changes to its characteristics, such as waking patients up during their sleep and dyspnea in decubitus position, leads to the physician requesting imaging exams for better clarification of the clinical condition.
Pain is many times interpreted, by both the physician and the patient, as induced by muscle strain or small trauma, leading to delays in proper diagnostic. A study compared 26 sarcomas in the ribs and observed that the most common clinical conditions identified were pleuritic pain and palpation of a mass. Delays of up to 3 months between symptoms and diagnosis of Ewing’s sarcoma have been observed, which is in line with the clinical case described here (Widhe et al., 2007).
The main prognostic factor of Ewing’s sarcoma is the presence or absence of metastases. The 5-year survival rate is at 70% among instances of localized disease, against 33% in the case of metastases at the time of diagnosis. There’s a greater probability of metastases in the case of primary bone tumors in the pelvic region, an elevation of the lactate dehydrogenase (LDH) levels at the time of diagnosis, a presence of fever, an interval greater than 3 months between symptom onset and diagnosis, and patient age above 12 years (Ferrari et al., 2001). Being an adult was a bad prognostic factor for this patient. A factor of good prognosis was the presentation of localized disease, which provides a life expectancy of 70% after five years.
The diagnostic assessment is started with a radiography of the affected area. The bone involvement of Ewing’s sarcoma is presented as a destructive bone lesion with the appearance of a “bite” associated with the mass of soft tissues. The CT scan provides a better assessment of the extent of cortical destruction, a definition of the tumor’s size and how affected is the bone’s interior and exterior. The MRI is useful for determining the tumor’s relation on the fascial planes, the vessels, the nerves and surrounding organs (Errani et al., 2020). Any patient presenting symptomatic bone lesions must perform a biopsy with molecular and cytogenetic study of the sample. According to guidelines from the NCCN (National Comprehensive Cancer Network®), besides the physical exam and imaging study of the primary location and possible metastatic locations, an analytical study including LDH must be performed for its prognostic value (Biermann et al., 2017). The patient initially underwent a chest and rib cage x-ray, as well as chest CT scan, and also an analytical study, but no LDH was requested due to a lack of knowledge of its prognostic value in these situations.
All patients with Ewing’s sarcoma must undergo primary treatment with chemotherapy and a growth factor for at least 12 weeks, followed by local treatment (surgery and/or radiotherapy) and further chemotherapy (Biermann et al., 2017). The initial chemotherapy improved these patient’s prognosis by controlling the primary lesion, evicting metastatic proliferation and diminishing relapses. Several essays show the efficacy of combining several agents, namely doxorubicin, vincristine, cyclophosphamide, ifosfamide, etoposide and dactinomycin (Gaspar et al., 2015). In the case described, the patient underwent cycles of initial chemotherapy and was later subject to local surgical resection. Resection started with a segmental removal of the rib. However, due to the presence of tumor at the margins of the surgical piece, a total costectomy of the 5th rib was later performed. Since the last surgical piece showed no signs of tumor at the margins, the oncology team decided there was no indication for radiotherapy, which complies with the NCCN guidelines (Biermann et al., 2017).
While multimodal treatment drastically improved the patient’s survival, there are acute and chronic adverse effects with negative impact on the patients’ quality of life. There are concerns that, in the long run, Ewing’s sarcoma survivors may see the occurrence of new primary tumors, pathologic fractures, the after-effects of radiotherapy (e.g. pulmonary fibrosis or neoplasia, neuropathy), and the after-effects of chemotherapy (infertility, renal failure and cardiomyopathy) (Friedman et al., 2017). In this case, the patient had several hospital admittances due to infections resulting from pancytopenia caused by chemotherapy toxicity. Even after double surgical intervention, a localized neuropathic pain remains, which is controlled via opioid analgesic medication and gabapentin.
Approximately 40% of Ewing’s sarcoma patients show localized or metastatic recurrence and a bad prognosis. Therefore, following the NCCN’s guidelines, surveillance must be maintained after treatment of Ewing’s sarcoma with a physical exam, chest CT scan every 3 months, radiography of the primary tumor location and analytical studies. The surveillance interval should be progressively increased, starting at every 6 months for the first 2 years, and then annually after 5 years (Biermann et al., 2017). The patient is currently being followed-up at the oncology center and has performed chest CT scans within the period recommended by the NCCN’s guidelines.
The pathology’s rarity, its location, and occurrence in a female adult means very few cases have been reported and published. The lack of specific symptomatology may lead to a significant delay in diagnosis and treatment, with consequent implications to the patient’s survival. On a daily basis, physicians make quick decisions based on the prevalence and incidence rates of diseases. There are, however, rare situations which require the physician to focus on warning signs and to know how to perform good anamnesis, objective examinations and make use of adequate diagnostic exams to perform swift diagnoses. The evolution of treatments has made it possible to extend the life expectancy of these patients, which in turn results in a specific clinical follow-up throughout several years. Therefore, the publication of this article aims to raise awareness on the existence of this pathology, the need to perform an early diagnosis and treatment, and how to continue the clinical follow-up after treatment.

