










Serviços Personalizados
Journal

Artigo
 Português (pdf)
Português (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
 Similares em
SciELO
Similares em
SciELO Compartilhar

 Permalink
PermalinkRevista de Enfermagem Referência
versão impressa ISSN 0874-0283
Rev. Enf. Ref. vol.serIV no.3 Coimbra dez. 2014
https://doi.org/10.12707/RIII1399
ARTIGO DE INVESTIGAÇÃO
Cross-cultural adaptation and validation of the portuguese version of the Newest Vital Sign
Adaptação cultural e validação da versão portuguesa de Newest Vital Sign
Adaptación cultural y validación de la versión portuguesa del Newest Vital Sign
Anabela Correia Martins* § ; Isabel Maria Andrade** §
§ Contributed equaly
* Ph.D. Adjunct Professor, Instituto Politécnico de Coimbra, ESTESC-Dept. Fisioterapia, 3046 – 854, Coimbra, Portugal [anabelacmartins@estescoimbra.pt]. Adress for correspondence: Rua 5 de Outubro, S. Martinho do Bispo, Apartado 7006, 3046-854, Coimbra, Portugal.
** MSc. Adjunt Professor, Instituto Politécnico de Coimbra, ESTESC-Dept. Fisioterapia, 3046 – 854, Coimbra, Portugal [imandrade@estescoimbra.pt].
ABSTRACT
Theoretical framework: The Newest Vital Sign (NVS) test was designed for simple, easy administration on Health literacy (HL) measurement.
Objectives: To make available an instrument in Portuguese to assess the HL level of the Portuguese population.
Methodology: Translation and cross-cultural adaptation of the original English version of the NVS into the Portuguese language. The validation process included the factor analysis and the establishment of its psychometric proprieties and the study of the association with other individual factors, such as the self-efficacy, Body Mass Index (BMI), age and lifestyles.
Results: Reliability was acceptable with Cronbachs alpha coefficient between .67 and .83. Using factor analysis with varimax rotation, two subscales explained 60.97% of the variance. Construct validity was also supported by the confirmation of predefined hypotheses involving expected correlations between the Portuguese version (NVS-PT), BMI, age and SES (convergent-divergent validity). An additional predefined hypothesis was also confirmed with the older subjects obtaining a lower score in the NVS-PT (p = .001).
Conclusion: The NVS-PT evidenced acceptable psychometric characteristics.
Keywords: health literacy; Portugal; population; validation studies.
RESUMO
Enquadramento: O Newest Vital Sign (NVS) foi construído para ser um instrumento de administração simples e rápida de avaliação da Literacia em Saúde (LS).
Objetivos: Disponibilizar um instrumento em língua portuguesa para a avaliação de LS da população portuguesa.
Metodologia: Tradução para a língua portuguesa e adaptação cultural da versão original inglesa do NVS. O processo de validação incluiu a análise fatorial e a avaliação das propriedades psicométricas e o estudo da associação com a autoeficácia, Índice de Massa Corporal (IMC), idade e estilos de vida.
Resultados: A fiabilidade foi aceitável, com alfa de Cronbach entre 0,67 e 0,83. Da análise fatorial com rotação ortogonal varimax obteve-se uma solução de dois fatores que explicam 60,97% da variância. A validade de construção foi ainda suportada pela confirmação das correlações entre a versão portuguesa do NVS (NVS-PT) e a idade, IMC e SES (validade convergente-divergente) e pelo facto de os mais velhos pontuarem mais baixo no NVS-PT (p = 0,001).
Conclusão: A versão portuguesa do NVS evidenciou características psicométricas aceitáveis.
Palavras-chave: literacia em saúde; Portugal; população; estudos de validação.
RESUMEN
Marco contextual: El Newest Vital Sign (NVS) ha sido diseñado para ser un instrumento de administración fácil y rápida para evaluar la alfabetización en salud (LS, por sus siglas en portugués).
Objetivos: Poner a disposición un instrumento en lengua portuguesa para evaluar el nivel de alfabetización en salud de la población portuguesa.
Metodología: Traducción y adaptación cultural al portugués de la versión original inglesa del NVS. El proceso de validación incluyó el análisis factorial, la evaluación de las propiedades psicométricas y el estudio de la asociación con la autoeficacia, el índice de masa corporal (IMC), la edad y los estilos de vida.
Resultados: La fiabilidad ha sido aceptable, con el alfa de Cronbach entre 0,67 y 0,83. Del análisis factorial con rotación ortogonal varimax se obtuvo una solución de dos factores que explican el 60,97 % de la varianza. La validez de constructo ha sido además sostenida por la confirmación de los valores de correlación entre la versión portuguesa del NVS (NVS-PT) y la edad, el IMC y la autoeficacia (validez convergente-divergente) y por el hecho de que los adultos mayores tuviesen una puntuación más baja en el NVS-PT (p = 0,001).
Conclusión: La NVS-PT ha mostrado propiedades psicométricas aceptables.
Palabras clave: alfabetización en salud; Portugal; población; estudios de validación.
Introduction
The concept of Health Literacy (HL) evolved from a history of defining, redefining, and quantifying the functional literacy needs of the adult population. Along with these changes has come the recognition that sophisticated literacy skills are increasingly needed to function in society and that low literacy may have an effect on health and health care (Berkman, Davis, & McCormack, 2010).
HL is increasingly recognised as one of the key determinants of health with growing evidence that lower HL is independently associated with higher rates of morbidity and mortality. Low HL creates difficulties in communicating with clinicians, poses barriers in managing chronic illness, lessens the likelihood of receiving preventive care, adds to the possibility of experiencing serious medication errors, increases the risk of hospitalisation, and results in poorer quality of life (Eichner & Dullabh, 2011).
Various studies show that levels of HL are lowest among socially disadvantaged groups; these same populations have higher rates of preventable non-communicable diseases, and experience greater difficulties accessing health services and managing their own health. Thus, improving HL has been identified by the World Health Organization (WHO) as a key strategy for enhancing the health of disadvantaged populations and tackling health inequalities in developed and developing countries (World Health Organization, 2009).
Portugal is lacking an assessment of its population HL level. More, the most frequently used HL measurements instruments are in English; therefore theres a need of HL assessment tests available in Portuguese. Our objective was to have a quick and accurate screening test for HL assessment in the Portuguese population, available in the Portuguese language, and at the same time suitable for use in primary health care settings.
Our choice was the Newest Vital Sign (NVS) test, which is a functional HL instrument, based on a nutrition label that is accompanied by 6 questions and requires 3-5 minutes for administration. Since its original version is in English, it is necessary to proceed with its translation into Portuguese, back-translation, cultural adaptation and its validation for the Portuguese population.
Background
HL concerns the knowledge and capacities of people to meet the complex demands of health in modern society and measuring HL will help to increase the awareness of patients HL skills, tailor health information for delivery to patients in a format they can understand and act upon, in their daily lives.
Although the importance of HL is increasingly recognised, the lack of consensus about the definition of HL or its conceptual dimensions limits the possibilities of measurement and comparison. Recently, Sorensen et al. (2012) published the results of a systematic literature review including 17 definitions and 12 models on HL: this review enabled the development of an integrated definition of HL and of a conceptual model containing evidence-based dimensions referring to knowledge, motivation and competencies of accessing, understanding, appraising and applying health-related information within the healthcare, disease prevention and health promotion settings.
Across Europe, for the first time, the assessment and comparison of HL level were undertaken by the European Health Literacy Project 2009-2012 conducted by the European Health Literacy Survey Consortium (HLS-EU Consortium), in eight countries: Austria, Bulgaria, Germany, Greece, Ireland, the Netherlands, Poland and Spain. The final results showed that across the eight countries, almost one in two, on average 47%, has risk of limited HL and that the levels vary between the countries. In certain subgroups of populations there are higher risks, such as among the elderly, people with low levels of education, with low socio-economic status and among people considering having a bad health condition (European Health Literacy Survey Consortium, 2012).
Sorensen et al. (2012) also show that an individual with an adequate level of HL has the ability to take responsibility for ones health as well as ones family health and community health.
Like HL, the concept of self-efficacy is also considered an individual-level construct: it lies at the centre of Banduras social cognitive theory, emphasizing the role of observational learning, social experience, and reciprocal determinism in the development of personality. According to the same author, a persons attitudes, abilities, and cognitive skills comprise what is known as the self-system, which plays a major role in how situations are perceived and how one behaves in response to different situations. Self-efficacy plays an essential part of this self-system. Those who have a high sense of efficacy visualise success scenarios that provide guidance, support a good performance and produce positive outcomes (Bandura, 1997).
When addressing health education and health promotion, the evaluation of self-efficacy has been perceived as a key factor to obtain better health outcomes (Pajares, 2002). Various levels of self-efficacy may promote or limit the motivation to act; supposedly a high level of self-efficacy is associated to better health or even better social participation and responsibilities (Bandura, 1997).
Although low levels of HL are present among all populations, it is more commonly observed among the elderly (Barrett, Puryear, & Westpheling, 2008). Older adults have more chronic illnesses and use more health care services than other segments of the population, and they face unique issues related to physical and cognitive functioning that can make it difficult for them to find and use appropriate health information (Federal Interagency Forum, 2008).
In a meta-analysis research study, Dewalt, Boone, and Pignone (2007) showed that limited HL has been linked to increased hospitalization rates, diminished use of preventive care measures and inadequate compliance to medical therapy.
The American Medical Association Foundation has also previously shown that those with low HL skills are also those with the highest proportion of persons not able to use preventive care services, and estimated that the costs of this low level of HL in the economy of the United States of America (USA) may be higher than 73 billion dollars/year (White, 2008).
Because HL is a key determinant of health, it was the aim of this study to obtain a Portuguese version of a quick and easy instrument to assess functional HL, suitable for use in primary health care settings, and evaluate its association with self-efficacy and individual lifestyle/behavioural factors.
Methodology
Cross-cultural adaptation
Translation of instrument measures into a foreign language demands different kinds of equivalences, such as lexical (language) and cultural.
The Portuguese version of the NVS (NVS-PT) was developed through a forward–backward translation procedure, according to the recommendations for translating questionnaires proposed by the Scientific Advisory Committee of the Medical Outcomes Trust (2002).
The authors of the Portuguese version, native speakers of Portuguese, with a high level of fluency in English, independently translated the nutrition label and the scoring sheet with six questions of the English, spoken in the USA, version of NVS. Both translated versions were then discussed in a first consensus panel. The consensus version was obtained after an adjustment of the ice cream nutrition label to European/Portuguese regulations. This preliminary version was then back-translated into English by two independent bilingual translators who were blinded to the original version. All inconsistencies between the resulting English version and the original version were examined and resolved in a second consensus panel to attain a comprehensible instrument, conceptually consistent with the original. Although always maintaining the consistency with the original scale, some expressions or sentences were slightly altered in order to be totally understood by the Portuguese citizens.
The preliminary Portuguese version was administered to a pilot group of 10 in order to identify and solve any potential problem in translation. After completing the questionnaire, subjects were asked about each item (e.g. if it was difficult to understand or confusing).
Validation Procedure
Subjects
The validation process was based on data from two samples. Sample 1 included students in grade 1 to 4 from all scientific areas of the College of Health Technology of Coimbra and also the College of Education, Polytechnic Institute of Coimbra. Subjects were 457, age ranging from 18 to 50 years (M = 20.89; SD = 4.43). Sample 2 comprised women and men recruited from a health community centre and a senior university. Subjects were 78, age ranging from 45 to 94 years (M = 69.82; SD = 9.16). These two samples were chosen due to the fact that they correspond to distinct age groups acknowledged in the literature as having different levels of HL.
The study was approved by the institutional Review Boards and was conducted in accordance to the ethical principles of the Declaration of Helsinki. Subjects provided informed consent.
Validation measures
All measures used to evaluate the construct validity of the NVS-PT were those included in the study protocol and were obtained at the same time the NVS-PT was administered. Demographic and clinical assessments included lifestyle/behavioural (healthy diet and physical activity) and Body Mass Index (BMI). Self-efficacy was assessed by the Portuguese version of the Self-Efficacy Scale (SES) (Ribeiro, 1994). It has 15 items, using a 7-point scale (1- strongly disagree to 7 - strongly agree) and the final score is the sum of the 15 items, ranging from 15 to 105, with higher scores corresponding to higher self-efficacy. The original version demonstrated good psychometric characteristics, with adequate reliability (Cronbachs alpha = .84) and validity.
Statistical Analysis
The description of the variables used for all demographic and clinical characteristics was carried out using frequency tables, means and Standard Deviations (SD).
Univariate Analysis of Variance (ANOVA) was used to explore differences between subgroups.
According to the recommendations of Barrett, Smith, and Wellings (2004), missing scores in one or two items of the SES were replaced by the mean value of the items to which subjects had responded. Missing data on socio-demographic and lifestyles variables were low-level and random and therefore not substituted.
To explore the NVS-PT internal consistency, Cronbachs alpha was obtained, as well as item-total correlations and alpha values when the item was deleted. Nunnaly and Bernstein (1994) have indicated .70 to be an acceptable reliability coefficient but lower thresholds are sometimes used in the literature. For these authors, a corrected item-total subscale correlation of .30 or higher was considered acceptable for each item in the subscales.
Although the original version presents only one domain, the construct validity was studied by exploratory factor analysis to test the hypothesis that the 6 items on the questionnaire represent 2 factors. Items with factor loadings and communalities ≥ .40 were considered acceptable (Staquet, Hays, & Fayers, 1998). Simultaneously, construct validity was assessed through correlations with measures hypothesized to be more strongly (convergent) or more weakly (divergent) related, according to a priori expectations based on the theoretical constructs (Scientific Advisory Committee of the Medical Outcomes Trust, 2002).
Item convergent and divergent validity was examined through item-scale correlations, inter-items correlations and correlation with the SES, BMI and age, using Pearsons correlation coefficient. We hypothesized that older people, those with higher BMI and with SES lower scores would have lower NVS-PT score.
For hypothesis testing, prior assessment of the metric variables assumptions was taken: for symmetry we used the coefficient of Skewness and for the flattening of distribution we used the coefficient of kurtosis. To assess adherence to normal distribution, we used the nonparametric tests Kolmogorov-Smirnov (Lilliefors correction factor) for samples > 50 individuals and/or Shapiro-Wilk for samples ≤ 50 individuals.
To further analyse the validity of NVS-PT, differences between gender and age group (≥ 65 years old and <65 years old) were analysed using t-Student and differences between lifestyle/behavioural factors (healthy diet and physical activity) were analysed using ANOVA with Scheffe test for multiple comparisons, when more than two groups were available. When homogeneity of variances was not assumed (Levene test), the Brown-Forsythe test (robust test of equality of mean values) was applied, and the non-parametric Kruskal-Wallis test, if data did not follow a normal distribution. A p value < .05 was taken as the reference level of significance. All analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 19.
Results
Cross-cultural adaptation
The second preliminary version of the NVS-PT was well accepted in the pre-test. In general, a good understanding of items and no major difficulties in responding to the questionnaire were reported. A third consensus panel was formed to achieve the final version of NVS-PT, which was used in the validation study (see Figure 1).
Validation Study
Subjects
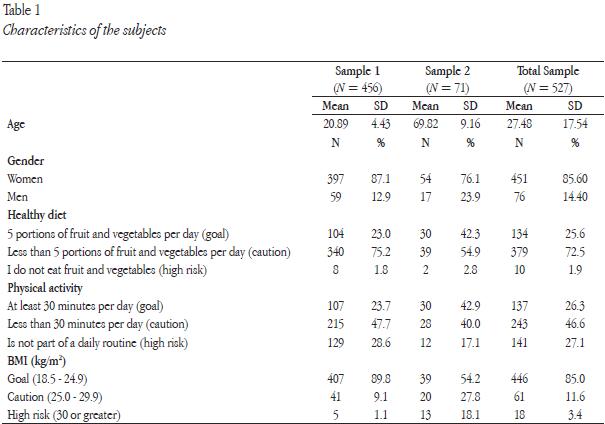
Demographic and clinical characteristics of the subjects, such as lifestyle/behavioural factors (healthy diet and physical activity), and BMI are presented in Table 1.
In the total sample, 85.6% of the subjects were women, and the mean age was 27.50 years (SD 17.50). Regarding lifestyle, 25.6% of individuals eat five portions of fruit and/or vegetables per day, 72.5% eat less than five portions of fruit and vegetables per day and 1.9% do not eat fruit and vegetables. Concerning physical activity, 26.3% spend at least 30 minutes per day in moderate activity, 46.6% practice less than 30 minutes per day, and for 27.1% physical activity is not part of a daily routine. 85.0% of the subjects presented a BMI value between 18.5 and 24.9 Kg/m2 (goal), 11.6% were at a caution level (25.0 - 29.9) and 3.4% were at high risk, with values equal or higher than 30 Kg/m2 (Total Sample Mean = 22.15, SD = 3.07).
HL level assessed by the NVS-PT shows that 10.3% of the subjects presented limited literacy, 13.7% showed possibility of limited literacy while 76.0% have adequate literacy. The total sample mean score of the NVS-PT was 4.44 (SD 1.70) and of SES was 76.02 (SD 15.30) (Cronbach´s alpha = 0.89).
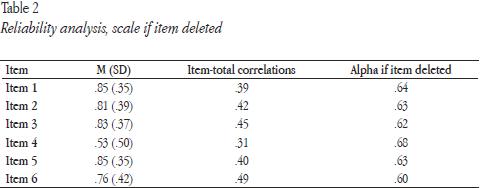
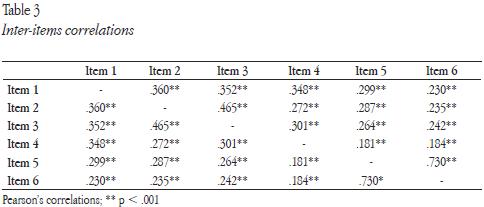
Reliability
Cronbachs alpha was .67 for the total items, .67 for the subscale 1 and .83 for the subscale 2, revealing that the NVS-PT has acceptable internal consistency. The corrected item-total correlations ranged from .31 to .45 (Table 2) and the inter-items correlations were positive and statistically significant (Table 3).
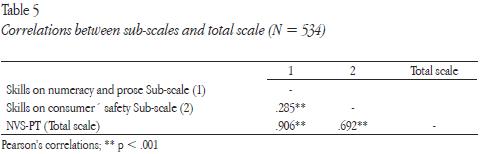
Construct validity
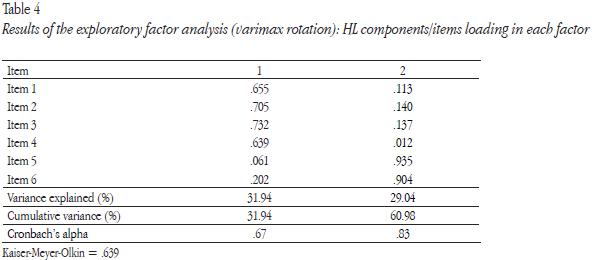
Using factor analysis with varimax rotation, two subscales explained 60.97% of the variance in the 6-item questionnaire. The domains reflect two aspects of functional HL: skills on numeracy and prose (factor 1) and skills on consumer´ safety (factor 2) (Table 4), confirmed by the association of sub-scales (Table 5).
The validity analysis examined by the associations between the NVS-PT measure and the construct validity measures was also studied. NVS-PT tool was hypothesized to be positively associated with better scores on self-efficacy measure and better lifestyles and more strongly with subjects age; rationale – in older people there is high likelihood of limited literacy.
Support for the convergent validity of the scale was demonstrated by associations between the NVS-PT and its sub-scales and the BMI, age and SES. Concerning age, large sized associations were found with total scale (r = -.599, p < .001), sub-scale 1 (r = -.535, p < .001) and sub-scale 2 (r = -.241, p < .001); weak sized associations were observed between the total scale (r = .291, p < .001), sub-scale 1 ( r= .319, p < .001) and sub-scale 2 ( r= .109, p < .05) and the self-efficacy; finally, weak associations between total scale (r = -.251, p < .001) and sub-scale 1 (r = -.214, p < .001) and BMI. Non-significant associations were found with the lifestyles.
The discriminant validity of the NVS-PT was further assessed by comparing differences between subjects aged ≥ 65 years old (n = 50) and < 65 years old, respectively 1.76 and 4.76 (range 0-6): total scale (t = 14.44, p = .001), sub-scale 1 (t = 12.58, p = .001) and sub-scale 2 (t = 6.41, p = .001).
Discussion
This study concerns the process of cross-cultural adaptation of the NVS to the Portuguese language and provides evidence of its reliability and validity.
The procedures of translation and cultural adaptation represented no major problems and gave rise to a reasonably intelligible Portuguese version of the NVS. Weiss et al. (2005) also reported similar findings regarding the cross-cultural adaptation of the NVS Spanish version.
Acceptable Cronbachs alpha coefficients for the two subscales and total scale, and satisfactory item-total coefficients for the 6 items confirmed that the NVS-PT subscales are internally consistent, with the correspondent items properly correlated with each other. The results for internal consistency were similar to those obtained by Weiss et al. (2005): Cronbach α = .76 and .69 respectively for the original NVS English version and the Spanish version (administered to English-speaking and Spanish-speaking primary care patients).
HL promotion takes place within a larger context, thus it makes sense to associate it with other measures such as self-efficacy and lifestyles. This study has shown that low HL levels correlate with low self-efficacy and worst IMC, what represents an important issue in health promotion interventions (Zarcadoolas, Pleasant, & Greer, 2006).
Moreover, as Barrett et al. (2008), we also confirmed that the elderly are those with higher likelihood of limited HL. Women scored higher than men, however, that difference was not statistically significant, in opposite to Peerson and Saunders (2009) findings. Therefore, the NVS-PT has the potential to be used for identifying those who may benefit from a strategic intervention.
The potential applicability of the NVS-PT as a standard assessment tool for gauging HL and improve patient-clinician communication in primary health care is high. Within a clinical environment, the NVS-PT instrument could be used to provide a general estimate of patient functional HL-related skills, in order to inform clinical decision making and health promotion planning with individuals or specific populations.
The NVS-PT test is easy to use; the time needed to complete it across subjects ranged from 3 to 6 minutes.
This study suggests that tools like the NVS-PT could be an important addition to the compendium of instruments used to assess health literacy, and also contribute to potentiate disease prevention and health outcomes, improving communication between patients and clinicians in health settings or to support health promotion planning (Institute of Medicine, 2009).
Limitations of the study
Some limitations of this study should be acknowledged. The sample used is not representative of the entire Portuguese population. Although associations between healthy diet, physical activity and HL were described in literature, our study did not confirm them.
Conclusions
The Portuguese version of the NVS obtained in this study demonstrated psychometric properties comparable to other NVS versions.
The NVS-PT instrument has shown promise as a measure of the concept of HL in the Portuguese population.
The NVS-PT acceptable levels of internal consistency suggest that it has utility in examining HL over time to both assess baseline level and evaluate HL intervention outcomes. However, more testing is required in order to confirm its responsiveness.
While other HL assessment tools exist, most require significant time resources to administer and analyse. The NVS test was designed for simple, easy administration and thus can be used on its own or incorporated with other measures of health, as part of a standard health assessment battery in primary care or to support health promotion planning.
References
Bandura, A. (1997). Self-efficacy: The exercise of control. New York, NY: Freeman. [ Links ]
Barrett, G., Smith, S. C., & Wellings, K. (2004). Conceptualisation, development and evaluation of a measure of unplanned pregnancy. Journal of Epidemiology and Community Health, 58(5), 426-433. [ Links ]
Barrett, S. E., Puryear, J. S., & Westpheling, K. (2008). Health literacy practices in primary care settings: Examples from the field. The Commonwealth Fund, 81(11). Retrieved from http://www.commonwealthfund.org/~/media/Files/Publications/Fund%20Report/2008/Jan/Health%20Literacy%20Practices%20in%20Primary%20Care%20Settings%20%20Examples%20From%20the%20Field/Barretthltliteracypracticesprimarycaresettingsexamplesfield_1093%20pdf.pdf [ Links ]
Berkman, N. D., Davis, T. C., & McCormack, L. (2010). Health literacy: What is it?, Journal of Health Communication: International Perspectives, 15(Suppl. 2), 9-19. doi:10.1080/10810730.2010.499985 [ Links ]
Dewalt, D. A., Boone, R. S., & Pignone, M. P. (2007). Literacy and its relationship with self-efficacy, trust, and participation in medical decision making. American Journal of Health Behaviour, 31(Suppl. 1), S27-35. doi:10.5555/ajhb.2007.31.supp.S27 [ Links ]
Eichner, J., & Dullabh, P. (2011). Accessible health information technology (Health IT) for populations with limited literacy: A guide for developers and purchasers of Health IT. Rockville, MD: Agency for Healthcare Research and Quality. [ Links ]
European Health Literacy Survey Consortium. (2012). Comparative report of health literacy in Eight EU Member States. Retrieved from http://www.health-literacy.eu [ Links ]
Federal Interagency Forum on Aging-Related Statistics. (2008). Older Americans 2008: Key indicators of well-being. Retrieved from http://www.agingstats.gov/agingstatsdotnet/Main_Site/Data/Data_2008.aspx [ Links ]
Institute of Medicine. (2009). Toward health equity and patient-centeredness: Integrating health literacy, disparities reduction, and quality improvement: Workshop summary. Washington, DC: National Academies Press. [ Links ]
Nunnally, J. C., & Bernstein, I. H. (1994). Psychometric theory. New York, NY: McGrawHill. [ Links ]
Pajares, F. (2002). Overview of social cognitive theory and of self-efficacy. Retrieved from http://www.emory.edu/EDUCATION/mfp/eff.html [ Links ]
Peerson, A., & Saunders, M. (2009). Mens health literacy: Advancing evidence and priorities. Critical Public Health, 19(3), 441-456. doi:10.1080/09581590902906229 [ Links ]
Ribeiro, J. L. P. (1994). Adaptação do Self-Perception profile for College Students à população portuguesa: Sua utilização no contexto da psicologia da saúde. In L. Almeida & I. Ribeiro (Eds.), Avaliação psicológica: Formas e contextos. Braga, Portugal: Apport. [ Links ]
Scientific Advisory Committee of the Medical Outcomes Trust. (2002). Assessing health status and quality-of-life instruments: Attributes and review criteria. Quality of Life Research, 11(3), 193-205. [ Links ]
Sorensen, K., Van den Broucke, S., Fullam, J., Doyle, G, Pelican, J, Slonska, Z., & Brand, H. (2012). Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health, 12, 80. doi:10.1186/1471-2458-12-80. [ Links ]
Staquet, M. J., Hays, R. D., & Fayers, P. M. (1998). Quality of life assessment in clinical trials: Methods and practice. Oxford, England: Oxford University Press. [ Links ]
Weiss, B. D., Mays, M. Z., Martz, W., Castro, K. M., DeWalt, D. A., Pignone, M. P., Hale, F. A. (2005). Quick assessment of literacy in primary care: The newest vital Sign. Annals of Family Medicine, 3(6), 514-522. doi:10.1370/afm.405 [ Links ]
White, S. (2008). Assessing the Nations Health Literacy - Key concepts and findings of the National Assessment of Adult Literacy (NAAL). Retrieved from http://www.ama-assn.org/resources/doc/ama-foundation/hl_report_2008.pdf [ Links ]
World Health Organization (2009). Background note: Regional Preparatory Meeting on Promoting Health Literacy. Retrieved from http://www.un.org/en/ecosoc/newfunct/pdf/chinameetinghealthliteracybackgroundpaperv2.pdf [ Links ]
Zarcadoolas, C., Pleasant, A., & Greer, D. S. (2006). Advancing health literacy. A framework for understanding and action. San Francisco, CA: John Wiley & Sons. [ Links ]
Received for publication: 09.04.13
Accepted for publication: 26.05.14


{kind=link}
{kind=link}
{kind=link}