











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Social Anxiety Disorder (SAD) is one of the most common mental disorders, characterized by an intense, disproportional, and persistent fear or anxiety of social events where one may be subjected to the scrutiny of others (American Psychiatric Association, 2013), namely interaction, observation or performance situations. Its onset is usually placed in adolescence (Beesdo et al., 2007), when acceptance by others becomes a developmental concern. SAD severely impairs diverse areas of adolescents’ daily life (i.e., school, leisure, social contact; Essau et al., 1998), including increased anxiety and avoidance when interacting with peers or potential romantic partners. It similarly affects taking part in academic activities, having poorer social performances (Rao et al., 2007), and having a higher risk of concurrent (Essau et al., 1998) or future (Beesdo et al., 2007) comorbidity with other psychiatric disorders. As such, it is important to provide interventions that may rapidly help adolescents manage SAD, thus changing its usually chronic and debilitating course (Beesdo et al., 2007).
Cognitive models for social anxiety (Heimberg et al., 2010; Wong & Rapee, 2016) propose that it arises from dysfunctional beliefs about the self as incapable of having an acceptable social performance and of others as likely to deliver a negative evaluation, which results in social-evaluative fears. These beliefs shape how one faces social events, specifically by allocating attention to congruent information, giving rise to negative automatic thoughts referring to fear of being negatively evaluated, embarrassed, or humiliated (Hope et al., 2010). More recently, the bivalent fear of evaluation model (Weeks & Howell, 2012) proposed that fear of general evaluation (i.e., negative and positive) is a relevant feature of social anxiety. Specifically, because individuals with SAD perceive a hierarchically intermediate position to be the safest, they not only fear that being negatively evaluated will lead to rejection, exclusion, or maltreatment by others, but also that being positively evaluated will lead others of higher social ranks to enter into a competition/conflict mode towards them. Previous evidence has been found for this model, precisely for the distinctive contribution of fear of both negative and positive evaluation to social anxiety (Fredrick & Luebbe, 2020; Reichenberger & Blechert, 2018). So, social events are judged against self-referent and, usually, threating information regarding one’s performance (either as too bad or too good), eliciting a rumination process and anticipatory anxiety when facing a new social event (Heimberg et al., 2010; Wong & Rapee, 2016).
As such, working to change negative automatic thoughts arising before, during, and after a social event, as well as allocating attention to the event itself, are recommended intervention strategies (e.g., Albano & DiBartolo, 2007). Changing automatic thoughts relevant to social anxiety may be achieved via cognitive restructuring (CR), which aims to identify and evaluate those thoughts; to understand their influence in everyday life; and to facilitate the use of more realistic and adaptive thoughts (Wild & Clark, 2011). CR has been applied to adult SAD as a stand-alone intervention and resulted in reduced social anxiety and related cognitive constructs (e.g., self-beliefs, fear of negative evaluation, Norton & Abbott, 2016; distress associated with negative automatic thoughts, Barrera et al., 2016). However, CR has not, to our knowledge, been used with adolescents as a stand-alone intervention, but rather as part of cognitive-behavioral interventions, which have been proved successful (Hayward et al., 2000; Warner et al., 2007).
Our study intends to explore if brief cognitive restructuring may produce changes in social anxiety, as a stand-alone intervention for adolescents with SAD. Short interventions may be specifically appealing to such adolescents, of which only a minority seek professional help (i.e., 8.53%, Beesdo et al., 2007). Specifically, change following a six weekly session intervention protocol based on CR was assessed using a pre- to post-intervention design and comparing with a waitlist control group. Moreover, we investigated the impact of cognitive change on post-intervention self-reported social anxiety.
Method
Sample
Recruitment and allocation. Prior to any data collection, this research was approved by the ethics committee of the host institution, within a broader research project intending to evaluate the outcomes from diverse therapeutic approaches to SAD in adolescence. Partnerships were established with four schools from the north and central regions of Portugal as contexts where potential participants would be recruited during the school year of 2016/2017. Schools provided parents and students with information about the study. They also requested parental informed consent for students attending the 10th and 11th grades to fill in the Social Anxiety Scale for Adolescents (Cunha et al., 2004) and then, if applicable, take part in a brief school-based intervention. Participants who scored one standard deviation above the mean value taken from a normative adolescent Portuguese sample on that self-report instrument were called for an individual structure clinical diagnosis interview (i.e., Mini-International Neuropsychiatric Interview for Children and Adolescents; Rijo et al., 2016). Inclusion (i.e., presenting with a primary diagnosis of SAD) and exclusion (i.e., presenting with no clinical diagnosis, with another primary diagnosis, with psychotic symptoms or being part of the special education system) were defined based on information taken from that interview. Participants who fulfilled those criteria and were available for one of three previously scheduled intervention groups constituted the intervention condition. Participants who, at that time, were not available for any of those schedules formed the waitlist condition. Participants in waitlist were not given any intervention during a six-week period, during which those in the intervention condition were receiving weekly sessions.
Participants were 23 adolescent girls with a primary diagnosis of SAD aged 14 to 18 years old (see Table 1), who came from the northern (n = 10, 43.47%) and central (n = 13, 56.52%) regions of Portugal. These participants were divided into Cognitive Restructuring Therapy (CRT; n = 14, 60.57%) or a waitlist condition (WL; n = 9, 39.13%). Students within these groups had similar mean ages (z = -.88, p = .40), and were similarly distributed by schooling (ꭓ2(3) = .53, p = .77) and socioeconomic level (ꭓ2(2) = 1.36, p = .51). Moreover, a similar proportion of them had had previous psychological support (ꭓ2(1) = .07, p = .79), which had ended for a similar number of months (z = .94, p = .97).
All participants from both conditions were asked to fill in the self-report protocol describe below at concomitant times, namely one week before the CRT was scheduled to start (i.e., pre-intervention) and one week after that intervention ended (i.e., post-intervention). After the post-intervention assessment, participants in the WL condition were invited to take part in CRT; 5 adolescents agreed to do so.
Table 1 Participants’ characterization by groups.
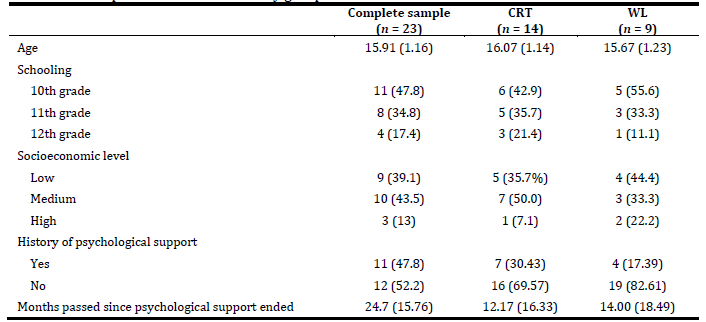
Note: Values for age and timing of psychological support are presented as M(SD); values for schooling, socioeconomic level, and history of psychological support are presented as n(%). CRT = Cognitive Restructuring Therapy; WL = Waitlist.
Intervention. The CRT focused on cognitive restructuring and consisted of six weekly sessions, each lasting approximately 60 minutes. The sessions addressed the following themes: psychoeducation on the cognitive vulnerabilities underlying social anxiety (session 1), cognitive distortions and their impact on behavior (session 2), changing negative automatic thoughts to realistic alternative thoughts (session 3), refocusing attention on external clues that may sustain realistic alternative thoughts (session 4), plan ways to gather external evidence from social situations (session 5), and review contents, competences and how to continuously apply them (session 6). For more information on each sessions’ key messages, see Table 2. For more detailed information on the intervention (including its dynamics and materials), please contact the corresponding author.

Instruments
Social Anxiety and Avoidance Scale for Adolescents (SAASA). Originally developed in Portuguese, it uses 34 items to assesses social anxiety and avoidance (Cunha et al., 2008) referring to six social contexts: Interaction in New Social Situations, Interaction with the Opposite Sex, Performance in Formal Social Situations, Assertive Interaction, Observation by Others, and Eating and Drinking in Public. Only the anxiety measure was used in the current study, which uses a five-point response scale ranging from ‘1 = none’ to ‘5 = very much’. Previous research has confirmed its six-factor structure, very good internal consistency levels (i.e., α ≥ .61 for the anxiety measures, Cunha et al., 2008; α ≥ .80 for the anxiety measures, Vagos et al., 2014) and construct validity in relation to anxiety and depression (Cunha et al., 2008). All measures achieved at least acceptable internal consistency values using the current sample at both evaluation moments: α ≥ .77 for Interaction in New Social Situations, α ≥ .89 for Interaction with the Opposite Sex, α ≥ .73 for Performance in Formal Social Situations, α ≥ .61 for Assertive Interaction, α > .66 for Observation by Others, and α ≥ .88 for Eating and Drinking in Public.
Specific Brief Fear of Negative Evaluation Scale - Straightforward items only. This instrument was based on the straightforward items of the Brief Fear of Negative Evaluation Scale, which were found to be one single construct when assessing community and clinical samples (Rodebaugh et al., 2011). Those 8 items were adapted to refer specifically to fear of negative evaluation (instead of general fear) when facing social situations (Correia et al., 2014). They are answered using a five-point response scale ranging from ‘1 = not at all like me’ to ‘5 = very much like me’. Previous studies using adolescent samples point to that instrument’s internal structure validity, good internal consistency, and construct validity in relation to social anxiety and avoidance measures (α = .92, Correia et al., 2014; α = .91, Vagos et al., 2015). At least very good internal consistency values (i.e., α ≥ .87) were found using the current sample at both evaluation moments.
Fear of Positive evaluation. This instrument uses 8 items to evaluate fear of positive evaluation via a five-point response scale ranging from ‘1 = not at all like me’ to ‘5 = very much like me’. Previous studies have argued for its internal structure validity, internal consistency, and construct validity in relation to fear of negative evaluation and other social anxiety measures, both in its original form applied to adults (α ≥ .83, Weeks et al., 2012) and in its Portuguese version applied to adolescents (α = .87, Vagos et al., 2015). At least very good internal consistency values (i.e., α ≥ .83) were found using the current sample at both evaluation moments.
Automatic Thoughts in Social Situations Scale - Adolescents. Originally developed in Portuguese, it includes 19 items that address automatic thoughts occurring in feared social situations based on a frequency four-point scale ranging from ‘0 = never’ to ‘4 = almost always’. Its scores previously showed a unifactorial structure, good internal consistency, test-retest reliability, and convergent validity (α = .95, Bento & Salvador, 2011). Excellent internal consistency values were found for all assessment moments using the current sample (α > .92).
Data analyses procedures
Descriptive analyses were used to characterize our sample, namely presenting frequencies and percentages about schooling, socioeconomic level, history of previous psychological support, and presenting mean and standard deviation values for age and time that had elapsed since previous psychological support had ended. Given the limited sample size, the CRT and WL were compared on those measures using non-parametric tests. The (un)even distribution of participants from both groups concerning schooling, socioeconomic level, and history of previous psychological support was analyzed using the chi-square distribution test. The mean level differences between participants from both groups on age and time that had elapsed since previous psychological support had ended were analyzed based on Mann-Whitney tests.
Most of the outcome measures under analysis followed a normal distribution, except for eating and drinking in public at pre- (W = .86, p = .006) and post-intervention (W = .88. p = .01), interaction in new social situations at pre-intervention (W = 85, p = .004), and assertive interaction at post-intervention (W = .91, p = .05). Still, Mixed ANOVAs were used to test for change from pre- to post-intervention across conditions for all measures. This a necessary statistical approach to accomplish the goals of this research and have no non-parametric equivalent. Specifically, our goals were to simultaneously compare change over time (i.e., within-subject effect), compare groups at assessment points (i.e., between-subject effect), and ascertain if that change was (dis)similar across groups (i.e., interaction effect). Homogeneity of variance for all measures was assumed based on the Levent Test. Additionally, the Greenhouse-Geiser correction was considered when the sphericity assumption was refuted. A priori analyses using the G*Power software show that, for a sample of 23 participants and power analyses set at .80, only large effect sizes would be found (i.e., > .40). Finally, hierarchical multiple regressions were conducted to test for predictors of post-intervention social anxiety within the CRT group. Pre-intervention scores on each anxiety measure and change in negative thoughts from pre- to post-intervention were entered as independent variables predicting the variance of post-intervention scores on that anxiety measure.
Results
Mean level differences
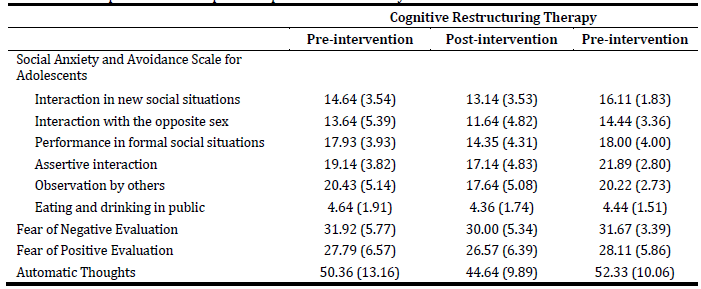
Descriptive values show decrease from pre- to post-intervention for all measures for CRT. The same was found for WL, except for Eating and Drinking in Public and fears of evaluation (Table 3).
A significant effect was found for Performance in Formal Social Situations, for time (F(1,21) = 4.99, p = .036, ƞ2 = .19); the effects for group (F(1,21) = 1.02, p = .324, ƞ2 = .046) and for group*time interaction (F(1,21) = 3.03, p = .097, ƞ2 = .13) were non-significant. Post-hoc comparisons show a significant difference from pre- to post-intervention (p = .036), which was significant for the CRT group (p = .005) but not for the WL group (p = .75). Other than that, only post-hoc comparisons on the frequency of negative automatic thoughts seem to point to a tendency for a significant change from pre- to post-intervention (p = .034) for the CRT but not the WL (p = .60). No significant or meaningful results were found in relation to the measures of fear of evaluation. For a detailed description of results on mean-level comparisons, see Supplementary Material.
Predictors of post-intervention results
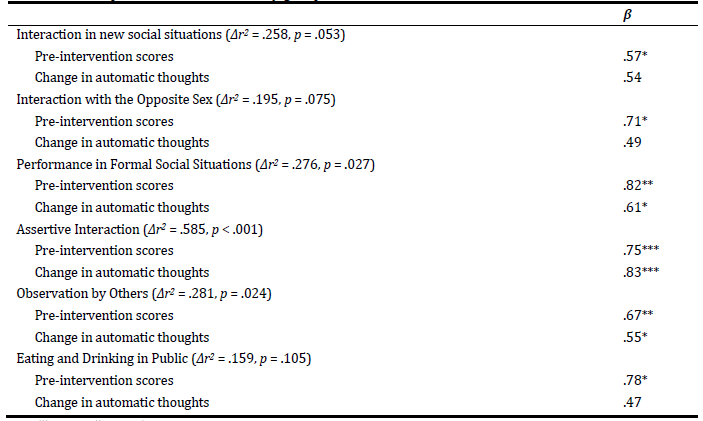
The regressive model under analysis (see ‘Data analyses procedures’ section) was not statistically significant for interacting in new social situations [F(2.13) = 3.63, p = .061, r2 = .288]. It was statistically significant for post-intervention anxiety when interacting with the opposite sex [F(2.13) = 4.47, p = .038, r2 = .348] and eating and drinking in public [F(2.13) = 4.31, p = .04, r2 = .337], though only pre-intervention anxiety scores were significant predictors. The same regressive model was statistically significant for predicting post-intervention anxiety in Assertive Interaction [F(2.13) = 17.17, p < .001, r2 = .757], Performance in Formal Social Situations [F(2.13) = 6.24, p < .015, r2 = .446], and Observation by Others [F(2.13) = 6.57, p = .013, r2 = .544]. In these cases, both predictors were statistically significant and change in automatic thoughts significantly increased the variance explained by pre-intervention anxiety scores (see Table 4).
Discussion
The current research sought to preliminarily evaluate changes in social anxiety and cognitive variables related to it, from before to after a brief cognitive-restructuring based intervention, using a sample of adolescents presenting with SAD. The relevance of this stand-alone intervention had only been examined with adults so far (Barrera et al., 2016; Norton & Abbott, 2016). Furthermore, we investigated if change in automatic thoughts contributed to explain post-intervention social anxiety, based on the theoretical assumptions that biased negative cognitions explains the development and maintenance of SAD (Heimberg et al., 2010).
Overall, social anxiety fluctuated over a period of eight weeks, regardless of adolescents being provided with specialized help or not. This may be related to natural ongoing exposure to social events in the adolescents’ daily lives. Accordingly, Social Effectiveness Therapy, a long-lasting intervention focused on exposure to feared social events, led to reduction in adolescent social anxiety (Spence et al., 2000). A natural exposure to social events may be particularly experienced in adolescence for interaction events, such as in new social events, with the opposite sex, and eating and drinking in public. The way these events were experienced was, therefore, not dependent on the condition (i.e., CT/WL) nor on cognitive change.
Alternatively, fears of evaluation only decreased when specialized help was provided, though not significantly so. This cognitive feature of social anxiety may only benefit meaningfully from exposure if it is done from a stance of behavioral experiments (i.e., facing social events while acknowledging that interpretation of those events may be biased by cognitive distortions and self-focused attention). Behavioral experiments may be an indispensable aspect to the previously found efficacy of CBT interventions for adolescent social anxiety (Hayward et al., 2000; Warner et al., 2007). The fact that such experiments were not part of the current intervention may be informative about the limited changes that were found.
Significant pre to post-intervention change was found for frequency of negative automatic thoughts, validating the specific goals intended by CRT, and aligning with specific cognitive gains from CR with adults (Norton & Abbott, 2016). This change was a significant predictor of post-intervention social anxiety for Assertive Interaction, Observation by Others and Performance in Formal Social Situations. This concurs with the theoretical (Heimberg et al., 2010) and applied (e.g., Albano & DiBartolo, 2007) framework positing the importance of changing negative thoughts to change social anxiety. Social anxiety for Performance in Formal Social Situations additionally decreased significantly from pre- to post-intervention for the CRT group only. Performance fears had been singled out as more characteristic of late adolescent social anxiety specifically and as pertaining to a theme of ‘me in front of others’ (Kodal et al., 2017). So, cognitive restructuring and its resulting decrease in the frequency of negative automatic thoughts had a demarcated effect on events when the focus is on the self, and not on ongoing exchanges between self and others (i.e., interaction events).
Importantly, change in negative thoughts may occur at their frequency, as currently assessed, or content, as focused on CRT. It may be that changing frequency of negative thoughts is relevant to these more structured events, whereas change in content and the way it progresses through therapy may sustain more generalized improvements in social anxiety. Given that addressing other-referent thoughts usually happens later in therapy (Hope et al., 2010), adding sessions to the current intervention might have resulted in more generalized gains. Additionally, considering other variables posed as vulnerability cognitive factors to social anxiety (e.g., mental imagery, Leigh et al., 2020 or self-focused attention, Canvin et al., 2016) might enhance changes following this intervention and provide information to better understand how change unfolds.
Limitations to the current study warrant caution when interpreting and generalizing current findings. First, we relied on a small non-treatment seeking and all girl sample, which was distributed to intervention and control groups based on availability, resulting in those groups having different sample sizes. Though this sample was thoroughly assessed for the presence of SAD and this disorder is more prevalent in girls (Jystad et al., 2021), and though the sample size is comparable to that previously used to explore change following new intervention approaches (e.g., Masia et al., 2001), further research is warranted on which to suggest for the applicability and relevance of this intervention to adolescent boys presenting with SAD and to investigate the effect of the intervention based on randomly assigned groups more systematically. Also, because the current sample size only allowed for large effect sizes to be found, investigating larger and more diverse samples may add information to other, currently indistinctive, changes following CRT. Finally, no information was gathered on the potential continuity of change throughout time. Gathering follow-up data would be essential to ascertain if gains are kept and/or generalized, or simply lost over time. Such information is particularly important in the light of SAD’s usually chronic course (Beesdo et al., 2007).
Current findings suggest that cognitive restructuring alone has had a limited effect on adolescent SAD, noticeable only in performance, which nevertheless is a recurrent and relevant experience in adolescence (Kodal et al., 2017). If these findings hold using larger and more diverse samples and employing a more rigorous clinical trial design, CRT may be recommended to adolescents presenting specifically with this subtype of SAD, thus making for a tailored intervention that has previously been called for (D’Avanzato & Dalrymple, 2016). As such, the modest and exploratory findings brought about by this research will hopefully be an incentive to future studies that may more thoroughly explore if, why, and for whom is cognitive restructuring useful in changing the course of adolescent social anxiety, at its moderate and clinical levels.
CRediT authorship contribution statement
Ana Félix: Data curation; Methodology; Resources; Visualization; Writing - Original draft; Ana Ferreira: Data curation; Methodology; Resources; Validation; Visualization; Writing - Original draft; Paula Vagos: Conceptualization; Formal analysis; Funding acquisition; Methodology; Project administration; Writing - Original Draft; Writing - Review & Editing

