











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Although the mini-implant has been used as an absolute anchorage during space closure to treat malocclusion with a high-anchorage demand,1-5distal movement of the entire dentition with mini-implants has not been studied extensively. The distal movement of the maxillary dentition using mini-implants involves retraction of all the teeth in the maxillary or mandibular arch and may be a preferred method for retraction of anterior teeth in patients with mild arch length/tooth size discrepancy as compared to inter-proximal reduction or second premolar extraction.
A thorough and systematic search in all the existing databases did not reveal any well-formulated clinical trial on the distal movement of the maxillary dentition using mini-implants, especially on a thicker arch wire. Although several articles describe molar distalization with an implant-supported system,6-11 few study the distal movement of the maxillary dentition using mini-implants.12-14 Earlier studies on the distal movement of the maxillary dentition12-14 evaluated it on 0.016” x 0.022” stainless-steel wire in a 0.018” / 0.022” slot and some had an insufficient sample size.12 Most studies evaluated the effect of this treatment’s mechanics on the molars and incisors, but a comprehensive overview of treatment change was not available.
Therefore, the present study proposed to evaluate the overall treatment outcome and side effects during distal movement of the maxillary dentition using mini-implants on a thicker wire: 0.018” x 0.025” stainless steel in a 0.022” slot. This study is unique as there is no published literature on distalization mechanics using the given arch wire/bracket slot combination.
The objective was to evaluate treatment change in the sagittal, vertical, and transverse dimensions and the undesirable side effects produced by distal movement of the maxillary dentition using buccal mini-implants on 0.018” x 0.025” stainless-steel wire in a 0.022” slot in the sagittal, vertical, and transverse dimensions.
Material and methods
This study was approved by the scientific review board and further reviewed by the ethical board. The sample consisted of 17 patients meeting the inclusion and exclusion criteria (Table 1). The inclusion criteria were: more than 15 years of age; mild-to-moderate arch length/tooth size discrepancy; full complement of teeth excluding the third molars; initial leveling and aligning phase of orthodontic treatment; no history of temporomandibular joint problems. The exclusion criteria were: <15 years of age; gross vertical discrepancy; severe skeletal Class II or Class III malocclusion; medically compromised; periodontally compromised; previous orthodontic treatment.
Based on earlier literature,14the power was calculated to be 97% for 16 patients to evaluate the amount of distal movement of the maxillary first permanent molar and the treatment outcome. The effect size was 0.934. After a detailed explanation of the procedure, written informed consent to perform the treatment and publish the images and the relevant findings of the study was obtained from all patients who matched the inclusion criteria and agreed to participate. Eighteen patients were selected for the study to compensate for dropouts. One patient dropped out during the study due to various reasons.
Of the 17 patients, six had an Angle’s Class I molar relation, five had an end on molar relation, and six had an end on one side and an Angle’s Class I on the other side on a Class I skeletal base. Since each patient required a different amount of tooth movement, the amount of distalization during six months was evaluated. Patients with an Angle’s Class I molar relation had a concomitant distal movement of the mandibular dentition. Distalization was carried out in both the upper and lower arch in these patients to correct the proclination of the maxillary and mandibular anterior teeth. These cases did not warrant extracting the premolars for gaining space.
Fixed orthodontic treatment using 0.022 MBT prescription (3M Unitek) was initiated for all patients. Leveling and aligning were sequentially carried out up to a 0.018” x 0.025” stainless-steel wire. The arch wire was sequentially changed from 0.016” nickel-titanium wire to 0.016” x 0.22” stainless-steel wire, followed by 0.017” x 0.025” stainless-steel wire and 0.018” x 0.025” stainless-steel wire. Third molars were removed prior to the placement of the mini-implant. Pre-distalization records, namely extraoral and intraoral photographs, study models, and lateral cephalogram (T1), were taken.
The width of the inter-radicular bone between the maxillary second premolar and the maxillary first permanent molar was assessed on the pre-treatment orthopantomogram to determine the feasibility of mini-implant placement. Indigenous mini-implants (1.2 x 8 mm) were placed bilaterally with a stent15 at the mucogingival junction between the maxillary second premolar and the maxillary first permanent molar at an angulation of 30°-40° to the long axis of the tooth.
An intraoral peri-apical radiograph was taken to check the mini-implants’ position. A distalizing force of 200 grams was applied bilaterally with pre-calibrated NiTi coil springs placed from the mini-implants to the crimpable hooks between the lateral incisor and the canine on both sides (Figure 1). The patient was reviewed periodically once every 3 weeks for 6 months. Post-distalization records, namely extraoral and intraoral photographs, study models, and lateral cephalogram, were taken (T2).

Figure 1 Distalization of the entire maxillary arch with buccal mini-implants placed between the maxillary second premolar and the maxillary first permanent molar
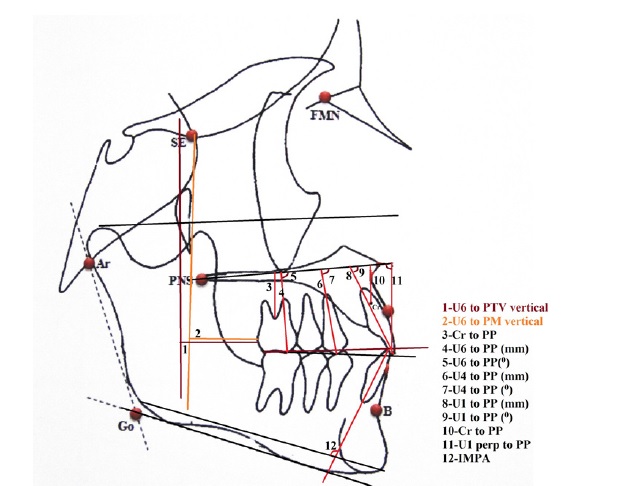
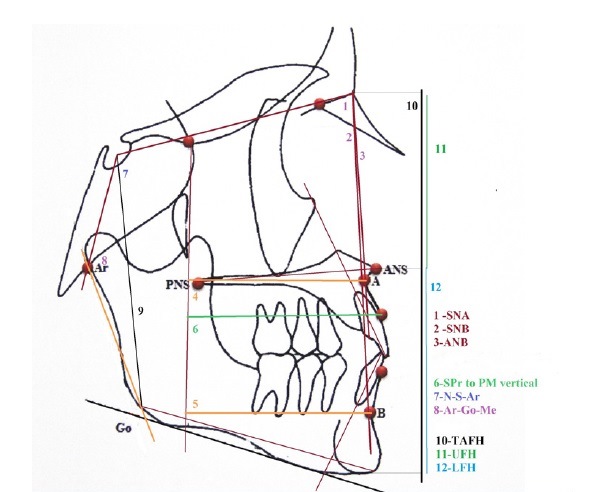
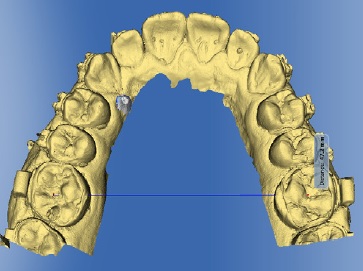
Lateral cephalograms were used to investigate the treatment outcome. The skeletal, dental, and soft-tissue parameters were evaluated (Figures 2 and 3). The facial proportion index16 was calculated using the following formula: (LAFH/TAFH minus UAFH/TAFH) x 100, where LAFH stands for lower anterior facial height, TAFH for total anterior facial height, and UAFH for upper anterior facial height. The extent of distalization of the maxillary first permanent molar was evaluated individually on the right and left sides. A short stainless-steel wire was placed in the auxiliary tube on the left first permanent molar to differentiate it from the right first permanent molar on the lateral cephalogram. This mark was made to precisely measure the extent of distalization of each maxillary first permanent molar and eliminate errors in measurement.
Root resorption was evaluated using intraoral periapical radiographs taken before the distalization and six months after. The extent of root resorption was evaluated as follows: 0 = no root resorption; 1 = blunting; 2 = irregular root outline; 3 = apical root resorption, less than 2 mm; 4 = apical root resorption, from 2 mm to one-third of the original root length; 5 = apical root resorption exceeding one-third of the original root length.
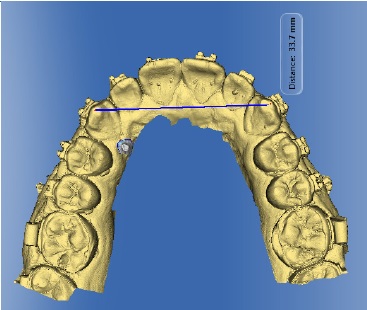
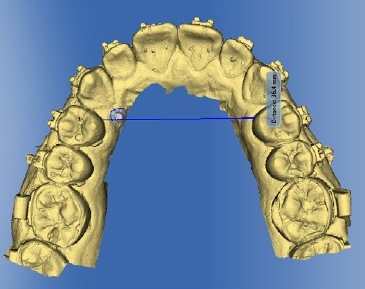
The transverse changes in the maxilla were assessed precisely on the dental casts using a CAD-CAM software (CEREC AC with CEREC BLUECAM 4.2 version). Inter-canine (Figure 4), inter-premolar (Figure 5), and inter-molar (Figure 6) widths were measured between the cusp tip of both maxillary canines, the mesial pit of both maxillary first premolars, and the central pit of both maxillary first permanent molars, respectively.
The various parameters were measured and entered in a proforma sheet. The values obtained were subjected to statistical evaluation. The non-parametric Wilcoxon signed-rank test was done to evaluate treatment changes within the group using the SPSS version 20 software as the sample size was small. The level of significance was evaluated at a 95% confidence interval with p≤0.05. One week after the initial evaluation, five radiographs were retraced in each group by the same investigator. The intra-operator error was assessed using Cohen’s kappa coefficient.
Results
The results obtained from the statistical evaluation are in Tables 1-5. There was no intra-operator error (the value of kappa was 0.9).
The mean age of the patients was 21 + 3.1 years in males and 18 + 3.0 years in females. The patients included in the study tended toward skeletal Class II malocclusion and horizontal growth pattern (Table 1).
Skeletal evaluation (Table 2) showed a reduction in the vertical proportions of the face with a statistically significant reduction in the lower anterior facial height and facial proportion index. There was a significant remodeling of the maxillary and mandibular alveolar bone. There was no statistically significant change in the position of the maxillary and mandibular skeletal bases and their relation to each other with no evident change in SNA, SNB, and ANB. No significant change in basal plane angle, mandibular plane, angle of inclination, upper anterior facial height, posterior facial height, total facial height, gonial angle, and saddle angle was observed.
Table 2 Comparison of treatment changes (T1-T2): Skeletal parameters
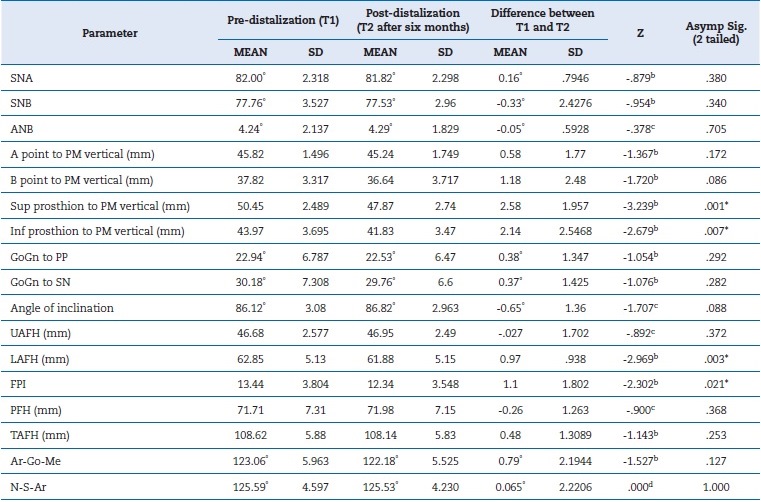
b. Based on positive ranks
c. Based on negative ranks
d. The sum of negative ranks equals the sum of positive ranks
* Statistically significant
Dental evaluation (Table 3) showed significant intrusion of the entire maxillary dentition. There was a significant retraction of the maxillary anterior teeth. Significant distal tipping of the maxillary first permanent molar by 3.88° was noted. The right and left maxillary first permanent molars were evaluated separately to determine the effect of distalization on each molar individually, and their extent of distal movement was almost similar: 1.71 ± 1.687 mm and 1.77 ± 1.48 mm with p=0.004 and p=0.007, respectively. The inter-incisal angle increased. There was a slight clockwise rotation of the maxillary occlusal plane and a marginal decrease in the incisor mandibular plane angle. A significant reduction in overjet occurred.
Table 3 Comparison of treatment changes (T1-T2): Dental parameters
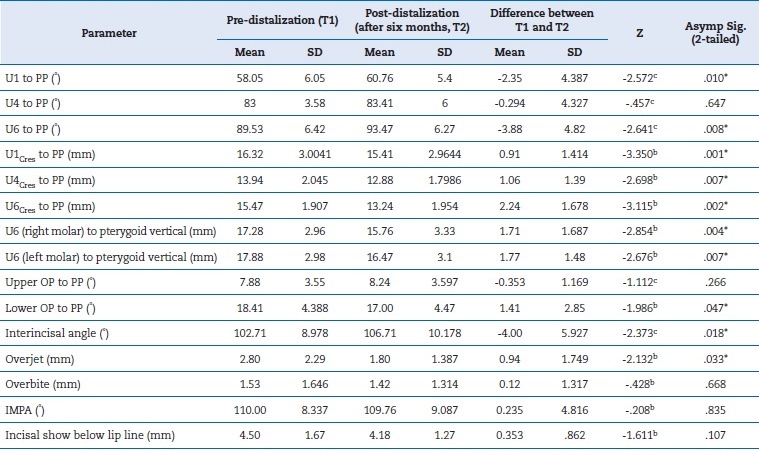
b. Based on positive ranks.
c. Based on negative ranks.
* statistically significant
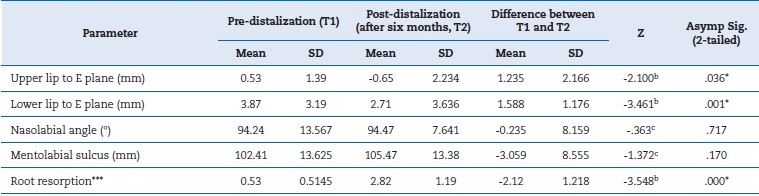
The cephalometric evaluation of soft tissue (Table 4) revealed a significant change in the position of the upper and lower lips. Root resorption was noted in the anterior teeth, with most cases showing irregular root outlines.
Table 4 Comparison of treatment changes (T1-T2): Soft Tissue/Root resorption
b. Based on positive ranks.
c. Based on negative ranks.
* Statistically significant
*** Degree of root resorption: 0= no root resorption; 1=blunting, 2= irregular root outline; 3= apical root resorption, less than 2 mm; 4= apical root resorption, from 2 mm to one-third of the original root length; 5= apical root resorption exceeding one-third of original root length
The effect of treatment mechanics on the maxillary arch measured in the transverse plane showed no statistically significant change in inter-canine and inter-premolar width. The inter-molar width increased by 0.38 mm, which was statistically significant (Table 5). The rate of molar distalization achieved on each side was 0.29 mm per month. The incisors retracted 0.39° per month.

Discussion
Distal movement of the maxillary dentition can be considered in cases of borderline skeletal Class II malocclusion with an end on molar relation to achieve a Class I molar relation and concomitantly correct the axial inclination of anterior teeth. It is also indicated in bimaxillary prognathism with mild proclination of the maxillary and mandibular anterior teeth in patients not willing to undergo orthognathic surgery.
Moreover, it can be considered in individuals with Class I malocclusion with mild bidental proclination or mild crowding of the maxillary anterior teeth. However, in these situations, distal movement of the mandibular dentition should be done concomitant with the upper arch. For distal movement of the maxillary dentition to be effective, extraction of third molars is mandatory except when the third molar is deep-seated and located relatively high up in the maxillary tuberosity.17 Fully erupted maxillary third molars will offer resistance to the distal movement of the maxillary arch, reducing the magnitude of distalization. Only individuals older than 15 years were included in the study to eliminate the effects of growth on the treatment outcome.
The quality of bone may not be satisfactory in younger patients, resulting in failure of the mini-implant.18,19The mean age of the patients included in the study was 19.06 years + 3.2 months.
The 0.022” x 0.025” slot was used as it is preferred by many orthodontists and has several advantages over the 0.018 X 0.025” slot. Previous literature20 suggests the use of 0.016” x 0.022” stainless-steel arch wire for distalization. However, we selected a thicker arch wire - 0.018” x 0.025” stainless-steel wire in a 0.022” x 0.25” slot, as it will offer better rigidity and torque control than the 0.016” x 0.022” stainless-steel wire.
Despite these precautions, root resorption was noted during treatment. This problem may be minimized by reducing the magnitude of applied force or increasing the time between activation.
The mini-implant site,21 diameter,22,23and placement angulation13,24 were determined considering that the entire maxillary dentition moves upon application of the distalizing force, and the resulting root proximity may result in mini-implant failure. The average success rate of the mini-implant was 82%, and six mini-implants were re-positioned throughout the treatment.
In the present study, the distalizing force was applied from the crimpable hooks placed in the anterior region to the mini-implant, resulting in an oblique force vector with retraction and a tendency toward the intrusion of the maxillary anterior teeth. Application of the point of force at the center of resistance of the maxillary dentition at approximately the same height as the mini-implant will result in a direction of force almost parallel to the occlusal plane, preventing rotational forces on the dentition.5 Some may say that the width of the inter-radicular bone on the buccal aspect may be insufficient between the maxillary second premolar and maxillary first permanent molar for distal movement of the maxillary dentition and loosening of the mini-implant may occur due to root proximity. Mild mobility of the mini-implants IS ACCEPTABLE AND may be considered successful if mini-implant mobility and orthodontic forces are periodically monitored.25
Evaluation of the treatment results showed significant retraction of the maxillary anterior teeth with remodeling of the alveolar bone as shown at the superior prosthion. Significant reduction in the lower anterior facial height and facial proportion index was noted and may be due to the significant intrusion of the maxillary premolars and molars with mild autorotation of the mandible. Hence, this appliance system may be beneficial in vertical growers.
Significant distalization of the maxillary first permanent molar with mild distal tipping was seen. There was a mild reduction in the inter-incisal angle, possibly improving post-treatment stability. Reduction in overjet was seen due to improvement in the axial inclination of the maxillary anterior teeth.
The extent of intrusion from anterior to posterior increased gradually, probably due to the posterior location of the mini-implant. If the direction of force application passes through the center of resistance of the maxillary dentition, only intrusion and distalization of dentition will occur. Otherwise, rotational forces should be anticipated.
Evaluation of the soft tissue showed a change in the position of the upper and lower lips at the end of treatment with improvement in profile. In the transverse plane, no significant change in inter-canine and inter-premolar width was noted. Mild expansion of about 0.38 mm was noted in the molar region.
The rate of molar distalization was around 0.29 mm per month and the rate of retraction of maxillary anterior teeth was 0.39°. The results showed no skeletal change, but the patient was evaluated for only six months.
The extent of distalization was comparable with that of Park HS,20 greater than that of Bechtold et al.,12 and less than that of Yamada et al..14 However, the extent of molar intrusion in the current study was greater than the latter study14 and may be due to a rigid arch wire and a better bracket-arch wire fit. All the above studies had a longer treatment duration than the current study.
Comparison with other conventional methods of molar distalization like the pendulum appliance and the bone-anchored pendulum appliance (BAPA) showed a lesser extent of distalization and distal tipping.6-8The distal jet appliance/skeletonized distal jet appliance supported by mini-implant anchorage26 and the first-class appliance showed greater molar distalization but significant premolar anchorage loss.27
Molar distalization with the skeletal anchorage system using bone plates was about 3.3 to 3.5 mm greater with slight distal tipping of teeth.7,8However, the bone plate placement is a very invasive procedure compared to the mini-implant placement and must be contemplated with care.
Conclusions
The overall treatment outcome of the maxillary dentition distalization on 0.018 x 0.25” stainless-steel wire in a 0.022 slot was good. Mild root resorption was noted in the maxillary anterior teeth. This method can be applied in cases with a mild-to-moderate arch length/tooth size discrepancy, especially Class II cases. It is beneficial in patients who require intrusion of the maxillary dentition, vertical growers requiring a reduction in the lower anterior facial height, and those with end on molar relation.

