










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Obstétrica e Ginecológica Portuguesa
versión impresa ISSN 1646-5830
Acta Obstet Ginecol Port vol.10 no.4 Coimbra dic. 2016
IMAGEM DO TRIMESTRE/IMAGE OF THE TRIMESTER
Prenatal diagnosis of sacrococcygeal teratoma
Diagnóstico pré-natal de teratoma sacrococcígeo
Margarida Cal*, Rui Marques de Carvalho**, Nuno Clode***
Hospital de Santa Maria, Departamento de Obstetrícia, Ginecologia e Medicina da Reprodução, Unidade de Ecografia
*Interna da formação específica de Ginecologia/Obstetrícia, Hospital de Santa Maria
**Assistente Hospitalar de Ginecologia e Obstetrícia, Hospital de Santa Maria
***Director do Serviço de Obstetrícia, Hospital de Santa Maria
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Sacrococcygeal teratoma (SCT) is the most common congenital tumor, with an incidence of 1:40,000 live births. It originates from multipotential embryonic stem cells and most tumors arise from the anterior surface of the sacrum or coccyx. On ultrasound, SCT presents as a heterogeneous mass of variable size that stands out from the sacrococcygeal region. Here we present a picture of a SCT detected at the 20-22 weeks ultrasound examination in our institution. The fetus, who had a normal ultrasound examination at 13 weeks, also presented other characteristics suggesting this diagnosis, later confirmed by an histopathological analysis.
Keywords: Prenatal; Diagnosis; Sacrococcygeal; Teratoma; Ultrasound
The picture presented here (Figure 1) shows a predominantly cystic mass arising in the fetal sacrococcygeal region, with 68 x 50 mm of major axis, vascularized, and detected at the 20-22 weeks ultrasound examination. The fetus, who had a normal ultrasound examination at 13 weeks, also presented hyperechoic kidneys with dysplastic aspect, a distended bladder and subjectively increased amniotic fluid. Echocardiography showed no anomalies. The couple opted for termination of pregnancy and the histopathological analysis confirmed an immature teratoma with an important extension into the pelvic cavity, causing anterior displacement of the perineum and pelvic organs. There was also hyperplasia of the erythroid lineage in the hepatic sinusoids, probably due to anemia related to the presence of the tumor.
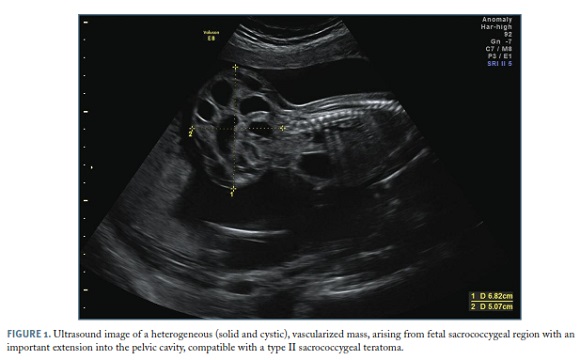
Sacrococcygeal teratoma (SCT) is the most common congenital tumor, with an incidence of 1:40,000 live births. It derives from multipotential embryonic stem cells from the anterior surface of the sacrum or coccyx. The majority of cases are sporadic, although a familiar subtype may be present in 25%1. On ultrasound, SCT presents as a heterogeneous mass of variable size that stands out from the sacrococcygeal region, with dense aspect or acoustic shadowing suggesting calcifications (not perceptible in this image)2. Other ultrasound signs include the presence of alterations caused by compression of adjacent structures, as the bladder distension and dysplastic kidneys evident on this image.
Most SCT are diagnosed on the 3rd trimester ultrasound. When the diagnosis occurs in the second trimester, as succeeded in this case, a worse prognosis is associated due to fast growth of the tumor and higher probability of arteriovenous shunts development with possible development of fetal hydrops or death. The differential diagnosis of SCT includes sacred meningocele, gastrointestinal pathology, retroperitoneal cystic tumor and ovarian cyst3.
Histologically, 90% of SCT are benign tumors and the vast majority of these occur in female fetuses (as in this case)4; cases of malignant histology have an equal incidence in both sexes5. SCT are usually extra-pelvic and subdivided into 4 types according to their pelvic extension that can be minimal (Type I) or total (Type IV); most cases (80%) are type I or II1.
85% of SCT are solid tumors with cystic component, being the remaining purely cystic. In the case described here, the ultrasound characteristics fall into a type II SCT with mixed component. Most fetuses with SCT are hemodynamically stable and surgical correction of the tumor can be performed in the postnatal period. However, in case of rapid tumor growth or arteriovenous shunt, there is a high probability of developing heart failure and intrauterine death1.
REFERENCES
1. Tsikhanenka I, Jeanty P. Fetal Tumors (in) Twining’s Textbook of Fetal Abnormalities (3rd Edition). Coady A, Bower S. Churchill Livingstone-Elsevier; 2015.
2. Woodward P. Spine: Sacrococcygeal Teratoma (in) Diagnostic Imaging Obstetrics (1st Edition). Woodward P, Kennedy A, Sohaey R. Amirsys-Elsevier; 2005.
3. Marković I, Stamenović S, Radovanović Z, Bošnjaković P, Ilić D, Stojanov D. Ultrasound and magnetic resonance imaging in prenatal diagnosis of sacrococcygeal teratoma - case report. Med Pregl. 2013; 66:54-57. [ Links ]
4. Maria Antonieta Melo, Nuno Clode. Diagnóstico das anomalias fetais mais frequentes (in) Medicina Materno-Fetal (4ª Edição). Graça, LM. Editora Lidel; 2012.
5. Lo Curto M, D’Angelo P, Cecchetto G, Klersy C, Dall’Igna P, Federico A, Siracusa F, Alaggio R, Bernini G, Conte M, De Laurentis T, Di Cataldo A, Inserra A, Santoro N, Tamaro P, Indolfi P. Mature and immature teratomas: results of the first paediatric Italian study. Pediatr Surg Int. 2007; 23:315-322. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Margarida Cal, Hospital de Santa Maria
PORTUGAL
E-mail: margarida.cal@gmail.com
