










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Obstétrica e Ginecológica Portuguesa
versão impressa ISSN 1646-5830
Acta Obstet Ginecol Port vol.13 no.4 Coimbra dez. 2019
CASE REPORT/CASO CLÍNICO
Acute myocardial infarction due to spontaneous coronary artery dissection in a twin pregnancy
Disseção espontânea das artérias coronárias numa gravidez gemelar: descrição de caso clínico
Inês Coutinho1, Manuel Oliveira-Santos2, Rui Baptista3, Etelvina Fonseca4, Paulo Moura5
Serviço de Obstetricia A do Centro Hospitalar e Universitário de Coimbra Serviço de Cardiologia do Centro Hospitalar e Universitário de Coimbra
1 Interna de Formação Específica em Ginecologia e Obstetrícia,Serviço de Obstetrícia A, Centro Hospitalar e Universitário de Coimbra (MDM/CHUC)
2 Assistente Hospitalar do Serviço de Cardiologia do CHUC
3 Assistente Hospitalar do Serviço de Cardiologia do CHUC; Assistente convidado de Cardiologia da FMUC
4 Assistente Hospitalar Graduada do Serviço de Obstetrícia A, MDM-CHUC
5 Diretor do Serviço de Obstetrícia A do CHUC; Professor Associado de Obstetrícia da FMUC
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
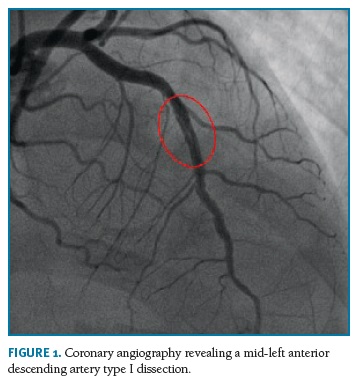
Spontaneous coronary artery dissection is a rare event during pregnancy, resulting in significant acute maternal and foetal mortality rates. We report a case of a mid-left anterior descending artery type I dissection in a 34-year-old primigesta with a 24-weeks monochorionic diamniotic twin pregnancy. She was treated medically with favourable outcome. Although quite rare in obstetric practice, spontaneous coronary artery dissection should be considered in the differential diagnosis of chest pain in pregnant women.
Keywords: Chest pain; Myocardial infarction; Spontaneous coronary artery dissection; Twin pregnancy; Pregnancy complications.
Introduction
Spontaneous coronary artery dissection (SCAD) represents an important but underrecognized cause of acute coronary syndrome (ACS) and myocardial infarction (MI) in pregnant and post-partum patients1. Up to 1 in 16,000 pregnancies are complicated by an acute MI2,3. It is a potentially catastrophic condition, with a fatality rate reaching 4.5%4.
Pregnancy-related SCAD commonly occurs during the late third trimester or the first month after delivery3,5. Clinical presentation can vary widely, posing a diagnostic challenge4. Prompt recognition of cardiac symptoms and coronary angiography tends to improve maternal and foetal survival rates6. Given the potential for severe outcomes and a recurrence risk of up to 12.5%3, pregnancy is not recommended after a SCAD-event3,5. Thus, proper contraceptive counselling must be provided7.
Case Report
We present the case of a 34-year-old primigesta with a spontaneous monochorionic diamniotic twin pregnancy, complicated by selective intrauterine growth restriction (sIUGR) after the 15th week. Subsequent twin-twin transfusion syndrome (TTTS) was diagnosed by oligohydramnios/hydramnios sequence along with critically abnormal Doppler of the donor twin. She was admitted at 24 weeks and 3 days in order to provide maternal and foetal surveillance. Two days after admission, the patient developed sudden epigastric discomfort along with nausea and vomiting, and sharp, severe and constant chest pain radiating to the right arm. The patient had no cardiovascular risk factors, and no tobacco, alcohol or drug abuse. Physical examination revealed: arterial blood pressure 135/86mmHg on the left and 141/90 mmHg on the right arm, ample and regular pulse (82 beats.min-1) and normal cardiac and pulmonary auscultation. Symptomatic treatment with acetaminophen, diazepam and metoclopramide was administered. An electrocardiogram (ECG) showed nonspecific repolarization changes and obstetric ultrasound revealed donor foetal demise. Laboratory assessment demonstrated normal blood count and coagulation, lactate dehydrogenase (LDH) 850 U/L, aspartate aminotransferase (AST) 506 U/L, alanine transaminase (ALT) 685 U/L, gamma glutamyl transferase (ϒ-GT) 166 U/L and normal creatine kinase (CK), creatine kinase muscle/brain (CK-MB) and myoglobin. First troponin I test was slightly elevated - 0.065 ng/mL [normal <0.057 ng/mL].
She underwent an emergency caesarean section for atypical preeclampsia, with birth of a 580g girl (5/5/8 Apgar score) and a 425g stillbirth. Surgical inspection showed no hemoperitoneum and a normal hepatic examination and ECG monitoring revealed no ST segment/T wave changes.
She remained drowsy during the postoperative period. Analytical control at 8 hours postpartum showed a troponin I level of 187.9 ng/mL, along with ECG T wave inversion in anterolateral leads. In the Emergency Room, handheld echocardiography revealed apical, anterior and lateral wall hypokinesia, with a mildly depressed left ventricular systolic function, (left ventricular ejection fraction of 43%). A high-risk non-ST elevation ACS (NSTEACS) was suspected and the patient underwent emergent transradial coronary angiography for risk stratification. Angiography revealed a mid-left anterior descending (LAD) artery type I dissection (Figure 1). Due to haemodynamic stability and patent artery flow, a conservative strategy without percutaneous coronary intervention (PCI) was adopted.
The patient was admitted to the Coronary Care Unit asymptomatic and with normal hemodynamic parameters (arterial blood pressure 135/70mmHg, resting heart rate 75beats.min-1). She was given dual antiplatelet therapy (aspirin 100mg qd and clopidogrel 75mg qd), low molecular weight heparin 1mg.kg-1 bid, carvedilol 6.25mg bid and atorvastatin 40mg qd, and was discharged 8 days later without events. The discharge echocardiogram revealed a mildly depressed LVEF (45%).
Neonatal death of the second twin occurred at day 4 of life due to septic shock. Five months after the event, the patient remained asymptomatic and progestin-based contraception was initiated. Screening for an underlying autoimmune disorder with antinuclear antibodies (ANA), anti-neutrophil cytoplasmic antibodies (ANCAs), rheumatoid factor (RF) and antiphospholipid (APL) antibodies was negative.
Discussion
SCAD is an under-diagnosed cause of AMI during pregnancy, with a incidence for 1.81 in 100000 pregnancies4. Current use of high sensitivity troponin assays, early angiography in ACS and widespread availability of intracoronary imaging has led to a greater awareness of this clinical entity, with incidences of 0.07 to 0.2% of all angiograms and 2 to 4% of ACS-driven angiograms1,8-10.
SCAD has been associated with fibromuscular dysplasia, connective tissue disorders and autoimmune diseases3,5,11. The predilection for female patients and the association with pregnancy suggests an etiological role for sex hormones1. Increased cardiac output during pregnancy had also been implicated as an etiological factor5. Additionally, emotional stressors have been reported in a high proportion of SCAD cases1. In our case, as the postpartum screening for an underlying cause was negative, we might speculate that the pregnancy-related emotional stress associated with severe TTTS at the fetal viability threshold, along with a particularly exacerbated cardiac output in a twin pregnancy, could all contribute to this outcome.
Chest pain is reported in 60-90% of cases1,3,7,12, as presented in this case. However as ECG and troponin results were initially non diagnostic, and in the presence of significant elevated liver function tests (LFTs), an emergency caesarean section was performed bearing in mind the diagnosis of atypical preeclampsia and eventual subcapsular liver hematoma. That diagnosis was not verified under surgical exploration. In this case, the elevation of LFTs was due to myocardial necrosis13,14. Our case poses an additional diagnostic challenge, as it presented early in pregnancy. Although described from as early as 5 weeks3,5, most cases occur late in the third trimester or in the periand postpartum period, with report rates ranging from 26 to 72.5%7,9,11.
Due to the haemodynamic stability and patent artery flow, medical management was adopted in our case. This strategy is supported by multiple reports, advising a conservative management whenever feasible5,15. Given the high complication rates associated with PCI and the spontaneous healing of most dissected segments presenting in pregnancy3,5, revascularization procedures are limited to patients with left main dissection, ongoing ischemia, ventricular arrthymias or haemodynamic instability3,5.
Finally, our case rises an additional point of discussion regarding the patient's reproductive future.
Given its potential for major complications, such as 10-year major adverse cardiac events and recurrence rates of 47.4%15 and 29%1,3 respectively, pregnancy after a SCAD-event is not currently recommended1,3,7. However, since it was a primigesta, a subsequent high-risk pregnancy is very likely; deferring it for at least 1 year is recommended7.
This case deserves to be highlighted by its rare presentation in a primigesta with a twin pregnancy complicated by the death of both foetuses. In the absence of reliable prevention strategies, it is necessary to establish guidelines for the surveillance of high-risk pregnancies after a PSCAD episode.
REFERENCES
1. Adlam D, Alfonso F, Maas A, et al. European Society of Cardiology, acute cardiovascular care association, SCAD study group: a position paper on spontaneous coronary artery dissection. Eur Heart J. 2018;(February):1-21. DOI: 10.1093/eurheartj/ehy080. [ Links ]
2. James AH, Jamison MG, Biswas MS, Brancazio LR, Swamy GK, Myers ER. Acute myocardial infarction in pregnancy: A United States population-based study. Circulation. 2006;113(12):1564-1571. DOI: 10.1161/CIRCULATIONAHA.105.576751. [ Links ]
3. Codsi E, Tweet MS, Rose CH, Arendt KW, Best PJM, Hayes SN. Spontaneous Coronary Artery Dissection in Pregnancy. Obstet Gynecol. 2016;128(4):731-738. DOI: 10.1097/AOG.0000000000001630. [ Links ]
4. Faden MS, Bottega N, Benjamin A, Brown RN. A nationwide evaluation of spontaneous coronary artery dissection in pregnancy and the puerperium. Heart. 2016;102(24):1974 LP - 1979. http://heart.bmj.com/content/102/24/1974.abstract.
5. Vijayaraghavan R, Verma S, Gupta N, Saw J. Pregnancy-related spontaneous coronary artery dissection. Circulation. 2014;130(21): 1915-1920. DOI: 10.1161/CIRCULATIONAHA.114.011422. [ Links ]
6. Paratz ED, Kao C, MacIsaac AI, Somaratne J, Whitbourn R. Evolving management and improving outcomes of pregnancy-associated spontaneous coronary artery dissection (P-SCAD): a systematic review. IJC Hear Vasc. 2018;18:1-6. DOI: 10.1016/j.ijcha.2017.12.001. [ Links ]
7. Naderi S. Spontaneous Coronary Artery Dissection and Pregnancy. Curr Treat Options Cardiovasc Med. 2017;19(9). DOI: 10.1007/s11936-017-0567-x.
8. Ferro J, Tortorella G, Pantaleoni M, Guiducci V. An unusual case of spontaneous left main coronary dissection in a young pregnant woman treated with percutaneous intervention. Int Cardiovasc Res J. 2017;11(4).
9. Havakuk O, Goland S, Mehra A, Elkayam U. Pregnancy and the Risk of Spontaneous Coronary Artery Dissection. Circ Cardiovasc Interv. 2017;10(3):e004941. DOI: 10.1161/CIRCINTERVENTIONS.117.004941. [ Links ]
10. Sabatine MS, Jaffer F a, Staats PN, Stone JR. Case records of the Massachusetts General Hospital. Case 28-2010. A 32-year-old woman, 3 weeks post partum, with substernal chest pain. N Engl J Med. 2010;363(12):1164-1173. DOI: 10.1056/NEJMcpc1000966. [ Links ]
11. Magarkar V, Lathi P. A case of spontaneous coronary artery dissection in early pregnancy managed by PCI. Indian Heart J. 2016;68:S25-S27. DOI: 10.1016/j.ihj.2016.04.021. [ Links ]
12. Roth A, Elkayam U. Acute Myocardial Infarction Associated With Pregnancy. J Am Coll Cardiol. 2008;52(3):171-180. DOI: 10.1016/j.jacc.2008.03.049. [ Links ]
13. Jang HJ, Oh PC, Moon J, et al. Prognostic Impact of Combined Dysglycemia and Hypoxic Liver Injury on Admission in Patients With ST-Segment Elevation Myocardial Infarction Who Underwent Primary Percutaneous Coronary Intervention (from the INTERSTELLAR Cohort). Am J Cardiol. 2017;119(8):1179-1185. DOI: 10.1016/j.amjcard.2017.01.006. [ Links ]
14. Gao M, Cheng Y, Zheng Y, Zhang W, Wang L, Qin L. Association of serum transaminases with shortand long-term outcomes in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. BMC Cardiovasc Disord. 2017;17(1). DOI: 10.1186/s12872-017-0485-6.
15. Tweet MS, Hayes SN, Pitta SR, et al. Clinical features, management, and prognosis of spontaneous coronary artery dissection. Circulation. 2012;126(5):579-588. DOI: 10.1161/CIRCULATIONAHA.112.105718. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Inês Coutinho
E-Mail: ines.mcoutinho@gmail.com
Conflict of Interest
The authors declare that they have no conflict of interests.
Acknowledgements
Not applicable.
Recebido em: 14/01/2019
Aceite para publicação: 02/09/2019

