











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Primary ciliary dyskinesia PCD is an inherited disease characterized by anomalies in the ciliary structure or function causing congenital impairment of mucociliary clearance1. Normal ciliary function is critical for respiratory tract, sperm mobility and normal visceral orientation during embryogenesis. Kartagener syndrome KS is a rare subtype of PCD defined by the clinical triad: bronchiectasis, chronic sinusitis and situs inversus1-3. KS has an estimated prevalence of 1 in 20.000-40.000 and inheritance is usually autosomal recessive3,4. Couples in which the male partner has KS have almost zero spontaneous pregnancy rates due to complete immotility of their spermatozoa and assisted reproduction techniques are indicated3,5-7. Intracytoplasmic sperm injection ICSI provides an effective treatment modality for patients with severe forms of male factor infertility and it is considered the treatment of choice in males with KS3,5,8. Pregnancies and healthy births in these patients using ICSI have been reported7. Different tests for assortment and selection of viable immotile spermatozoa are described. However, the outcome of ICSI using immotile spermatozoa is poor and most reports show low fertilization rates in these patients5,6. In this report, we present two cases of infertility due to KS where pregnancy was achieved with ICSI using two different methods of spermatozoa selection.
Informed written consent has been obtained and all identifying information is omitted.
Case report
Case 1
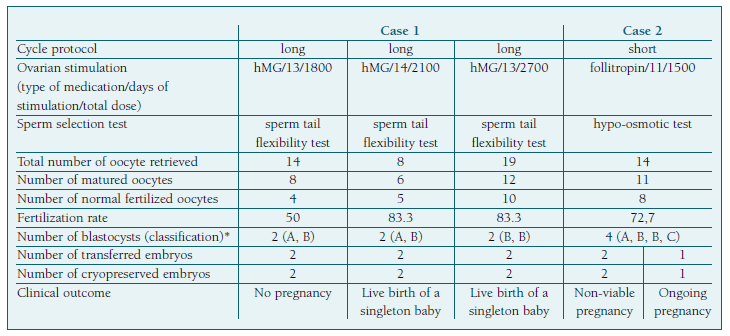
A 32-year-old woman and her 36-year-old husband were referred to our infertility center with a history of primary infertility for 3 years. Her medical history was uneventful. Her cycles were regular and transvaginal ultrasound examination was normal. The male partner had a history of chronic bronchitis, bronchietasis and situs inversus, the classic triad disorders of KS. A semen sample was collected by masturbation into a sterile cup. Initial evaluation revealed a sperm concentration of 102x106/ml and all spermatozoa were immotile. Eight percent of spermatozoa were morphologically normal using Kruger criteria9. Sperm analysis was repeated three months later with the same result regarding motility. His karyotype was normal, 46,XY. The couple was advised to perform ICSI. Controlled ovarian hyperstimulation was performed by a long standard protocol with human menopausal gonadotropin hMG after down-regulation with leuprorelin acetate as a GnRH agonist. Follicular development was assessed by transvaginal ultrasonography. When at least two dominant follicules were ≥ 18 mm, ovulation was induced with human chorionic gonadotropin hCG. Oocyte retrieval by transvaginal ultrasonography was performed approximately 36 h after the hCG administration. Fourteen oocytes were retrieved. Before ICSI, a sample of ejaculated sperm was collected and analyzed. Spermatozoa selection was performed using the sperm tail flexibility test and was based on spermatozoa structure and tail movement. Eight oocytes were microinjected resulting a 50% fertilization rate. Two quality blastocysts were obtained and transferred on the fifth day after oocyte retrieval. β-hCG was negative two weeks after embryo transfer. Later the couple did two more ICSI cycles using a similar protocol and method of spermatozoa selection as the first cycle. Fertilization rates were 83.3% in both cycles. Data of each cycle are presented in table I. In each cycle, two quality embryos were obtained and transferred on the fifth day after oocyte retrieval. β-hCG was positive and a singleton intrauterine pregnancy was confirmed by transvaginal ultrasound posteriorly in both of them, resulting in the birth of two healthy infants at 37 and 39 gestational weeks, respectively.
Case 2
A 27-year-old woman presented to our department with primary infertility of 3.5 years. Her diagnostic work-up was normal. She had regular cycles and transvaginal ultrasound was normal. Her husband was 36 years old. He was a smoker and had chronic sinusitis. Due to his respiratory background, a CT scan performed years before the consultation described bronchiectasis and situs inversus. Ejaculated semen analysis revealed a sperm concentration of 12x106/ml and no evidence of sperm mobility; morphological analysis showed 15% normal spermatozoa using Kruger criteria.9 His semen analysis repeatedly showed totally immotile spermatozoa. The man attended clinical genetics appointment and the diagnosis of KS was made. His karyotype was normal, 46,XY. Given that the couple had close geographical origins, NGS-based panel for PCD in his partner was also recommended and it came back negative. Afterwards the couple was informed of the treatment options and proposed for ICSI using ejaculated sperm. Controlled ovarian hyperstimulation was achieved using an antagonist GnRH cycle protocol with follitropin. hCG was given to induce ovulation when at least two dominant follicules were ≥ 18 mm and oocyte retrieval by transvaginal ultrasonography was performed approximately 36 h after the hCG administration. Fourteen oocytes were retrieved. Prior to ICSI, sperm analysis showed a concentration of 4x106/ml; all spermatozoa were immotile. Selection of spermatozoa was carried out using the hypo-osmotic test and individual morphologically normal spermatozoa were selected and placed in the hypo-osmotic solution for viability selection. In this cycle, eleven oocytes were microinjected resulting a 72.7% fertilization rate. Of four quality blastocysts obtained, two blastocysts were transferred on the fifth day and two were cryopreserved Table I. β-hCG was positive but a non-viable pregnancy was diagnosed at 7 gestational weeks. A few months later, a frozen-thawed embryo transfer cycle was performed and β-hCG was positive. This time an ongoing pregnancy of 8 gestational weeks was confirmed.
Discussion
Primary Ciliary Dyskinesia PCD is believed to be caused by ultrastructural defects in the dynein arms connecting the microtubules which leads to ciliary epithelial disfunction and sperm mobility8,11. In patients with PCD clinical manifestations include recurrent infections of the upper and lower respiratory tract, chronic pansinusitis, bronchiectasias and male infertility1,2,5,11,12. KS is an autosomal recessive genetic disease accounting for approximately 50% of the cases of PCD. It is one of the most serious subtypes of PCD as it is characterized by simultaneous abnormal ciliary function in several parts of the organism. The syndrome is caused by mutation of DNAH5, DNAI2, DNAH9 and other genes that are involved in the formation of several kinds of proteins composed of a ciliary microstructure1,2,4,12. As sperm flagellum is also a type of cilia, male patients with KS are invariably thought to be infertile presenting with totally immotile spermatozoa. 8 A few male patients with KS who were fertile have been reported, however, in most cases male patients with KS need assisted reproduction techniques to achieve pregnancy. 8,13,14 ICSI is currently the only treatment option for most KS patients and shows promising results in these patients.
Regarding sperm sample selection, we used ejaculated spermatozoa rather than testicular spermatozoa in both cases, although some reports suggest slightly higher fertilization and pregnancy rates with testicular spermatozoa. 2,3,11 Vital spermatozoa are a prerequisite for successful ICSI and motility is the unique marker for viability in sperm selection. In KS it is more challenging for an embryologist to select which spermatozoa to use, however different techniques for selection of viable immotile spermatozoa are described. The most commonly techniques for immotile sperm assortment are the hypo-osmotic swelling HOS test, chemical substances for induction of tail movements, the sperm tail flexibility test STFT and LASER assisted immotile sperm selection. Each technique has their own benefits and drawbacks, with variable fertilization rates. The choice of the test depends upon the type of procedure undertaken, available equipment and, most important of all, experience of the embryologist. 15,16 In case 1 spermatozoa selection was carried out using STFT, which is completely based on the examination of the selected spermatozoa. In this technique, the spermatozoa were considered motile if the tip of the sperm tail showed a slight movement irrespective of head movement after being touched by the ICSI injecting pipette. It is a fast technique that doesn’t need extra equipment or additional substances but requires a high level of experience by the embryologist as it is extremely influenced by personal observation. On the other hand, in case 2 spermatozoa selection was performed using the HOS test. Here the spermatozoa were exposed to a hypo-osmotic medium. The HOS test caused the tails with intact membranes to swell. Once identified these spermatozoa, they were placed in a normo-osmotic fluid where they regained normal shape prior to injection. In the two cases presented sperm selection was performed using different techniques mainly due to availability of tests at the time in our department, however high fertilization rates were obtained using both techniques. Currently, the HOS test is the recommended and most used test for selection of spermatozoa in KS7,15,16. Our report highlights the importance of evaluation of spermatozoa by an experienced embryologist as one of the crucial steps in the management of these couples. At the time these couples were referred to our institution, decision between single or double embryo transfer depended mainly on couple’s wishes, if there were no clinical contraindications for multiple pregnancy.
Regarding inheritance of PCD/KS, in order to assess the risk of these couples’ offspring, a sequencing PCD gene panel although not performed routinely may be offered to enable a molecular diagnosis, which may technically be used for preimplantation genetic diagnosis PGD or prenatal diagnosis3,4,12. In case 2 it was recommended to study the partner due to the couples’ close geographical origins, however as the test was negative, PGD was not discussed.
Authors’ contributions
Cláudia Miranda: Contributed to the analysis and interpretation of data, reviewing the literature and drafting the article.
Sofia Costa: Contributed to the diagnosis of the clinical case, interpretation of data, critical review and final approval of the submitted version.
Diana Coelho: Contributed to the critical review of the article.
Sofia Dantas: Contributed to the critical review of the article.

