










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.11 no.1 Lisboa mar. 2015
ORIGINAL ARTICLE
Groin wound infection in vascular surgery. A one year institutional incidence
Infeção da ferida cirúrgica inguinal na cirurgia vascular. Incidência de um ano de uma instituição
Gabriela Teixeiraa,*, LuÃs Loureiroa, Rui Machadoa, Arlindo Matosa, Rui Almeidaa
aServiço de Angiologia e Cirurgia Vascular do Hospital de Santo António, Centro Hospitalar do Porto, Porto, Portugal
ABSTRACT
Introduction/Objectives: Surgical site infection (SSI) in vascular surgery is a complication that may lead not only to healing problems, but also limb loss and risk of death. The incidence of surgical site infection at the groin after vascular procedures ranges among 3% to 44%. The aim of this study is to review the incidence of groin infection in our department and the degree of correlation between infection, known risk factors and preventing measures.
Methods: Retrospective review of consecutive arterial vascular surgeries in a university central hospital during one year. Patients undergoing groin incisions were studied according to baseline demographics, clinical characteristics, active infection, previous inguinal access, antithrombotic therapy, indication for intervention, prophylactic antibiotic use, type of intervention and type of graft used. Wound site infections over a 30-day period were registered and graded based on Szilagyi classiï¬cation. On patients with documented groin infection, the presentation timing, modality of treatment (surgical and non-surgical) and time of healing were recorded. Data were analyzed by using SPSS 18.0 version software.
Results: From January to December 2013, 1266 vascular surgeries were performed. Of these, 782 were arterial vascular procedures, 279 by inguinal approach, with a total of 358 groin incisions. Our base population included 241 patients (31 patients with more than one procedure in a year). Total infection rate was 4.7% (17/358 groin incisions). All Szilagyi I (n = 4) resolved with antibiotic only; three of the ten Szilagyi II infections needed drainage/debridement at operation room; the other Szilagyi II resolved with antibiotic and wound care. All Szilagyi III infections (n = 3) were treated with bypass removal, and in two patients an in situ revascularization was performed. These two patients died from sepsis. Identiï¬cation of the infecting agent was possible in 9 patients, with the most common isolated agent being Pseudomonas. Hypertension was signiï¬cantly associated with a higher risk of SSI (p = 0.033).
Discussion/Conclusions: In our department, the infection rate of the inguinal approach equals the best international standards described. These results may be the outcome of a carefully planned strategy of infection control. Arising from the fact that groin SSI is a low incidence event, correlations between suspected risk factors and this infection are hard to establish. Longer follow-ups would be useful for identiï¬cation of all groin infections.
Keywords: Vascular surgical site infection; Groin infection; Vascular synthetic graft infection
RESUMO
Introdução/Objetivos: A infeção do local cirúrgico na cirurgia vascular é uma complicação que não só implica atrasos na cicatrização, mas que pode levar a perda de membro e a risco de vida para o paciente. A incidência descrita de infeção da ferida cirúrgica inguinal após procedimentos vasculares varia de 3 a 44%. Este estudo tem como objetivo quantiï¬car a incidência de infeção inguinal no nosso serviço e estabelecer nÃveis de correlação com fatores de risco e medidas preventivas.
Métodos: Estudo retrospetivo das cirurgias vasculares arteriais realizadas num hospital universitário durante um ano. Pacientes com abordagem inguinal foram estudados segundo caracterÃsticas clÃnicas e demográï¬cas, infeção ativa, acesso inguinal prévio, terapia antitrombótica, indicação cirúrgica, antibioterapia proï¬lática, tipo de intervenção e tipo de enxerto. Foram registadas as infeções do local cirúrgico e classiï¬cadas segundo Szilagyi. Nos pacientes com infeção, documentamos o tempo de apresentação, tratamento e tempo de cicatrização. Os dados foram analisados no SPSS 18.0.
Resultados: De janeiro a dezembro de 2013, foram realizadas 1266 cirurgias vasculares, das quais 782 arteriais. Destas, 279 tiveram abordagem inguinal, com um total de 358 incisões inguinais e uma amostra populacional de 241 pacientes (31 reintervencionados). A taxa de infeção foi de 4,7% (17/348 incisões). Todas as infeções Szilagyi I (n = 4) resolveram com uso exclusivo de antibiótico. Três das dez infeções Szilagyi II necessitaram de drenagem/desbridamento no bloco; as restantes Szilagy II resolveram com antibiótico e cuidados de penso. Nas infeções Szilagyi III (n = 3) foi retirada a pontagem, e em dois doentes foi tentada a revascularização in situ. Esses dois pacientes morreram. A identiï¬cação do agente infecioso foi possÃvel em 9 pacientes, sendo a Pseudomonas o agente mais comum. A hipertensão esteve signiï¬cativamente associada a maior risco de infeção (p = 0,033).
Discussão/Conclusões: A baixa taxa de infeção descrita é comparável aos melhores resultados publicados sobre este tema. Estratégias de controlo de infeção reï¬nadas ao longo de anos podem contribuir para estes resultados. Contudo, sendo um evento de baixa incidência, correlações entre infeção da ferida inguinal e fatores de risco são difÃceis de estabelecer. PerÃodos de seguimento mais longos são necessários para a identiï¬cação de todas infeções a este nÃvel.
Palavras-chave: Infeção ferida cirúrgica vascular; Infeção ferida cirúrgica inguinal; Infeção prótese vascular
Introduction
Surgical site infection (SSI) in vascular surgery is a complication that may lead not only to healing problems, but also limb loss and risk of death. It always implies increased hospital stay, hospital costs and morbidity for the patient.1
Groin incisions play a central role in various vascular surgical procedures. In addition to their traditional use in bypass procedures, endarterectomies and thromboembolectomies, more than 95% of all percutaneous interventions are performed by femoral access.2
The incidence of surgical site infection at the groin after vascular procedures ranges from 3% to 44%.3 Factors contributing to the increased incidence of SSI in this subset of patients include disruption of lymphatics, proximity to the perineum and prosthetic graft placement. The increasing prevalence infection by multiresistant bacteria has been associated with worsened outcomes.4
Although the management of groin SSI is well documented, there is little published about the incidence and classiï¬cation of these infections. Szilagyi et al said that diabetes, as well as obesity, had a relatively small role in initiating groin wound infection.5 A recent study showed that redo bypass, female gender, diabetes and active infection were associated with a risk of graft infection involving the femoral artery.6
Besides the general aseptic measures, the only strategy that signiï¬cantly reduces the incidence of SSI is prophylactic systemic antibiotics administered only preoperatively.4
There is no ââgold standardââ for treatment of these infections. The initial treatment generally includes surgical debridement and antibiotics. Secondary interventions have been attempted with limited success, including rotational ï¬aps, wound vacuum-assisted closure, alginate dressing, graft excision and extra-anatomic or in situ bypass or patch replacement using autologous, rifampin-soaked or silver-impregnated materials.7--10The aim of this study is to describe the incidence of groin infection in our vascular department and the degree of correlation between infection/known risk factors and infection/preventing measures.
Methods
Retrospective review of consecutive arterial vascular surgeries in a central operating room during one year. Patients undergoing groin incisions for arterial vascular procedures were studied according to baseline demographics, clinical characteristics, active infection (ipsilateral lower extremity infection occurring before vascular surgery), previous inguinal access (including arterial puncture), antithrombotic therapeutic in use, initial indication for intervention, type of intervention and type of graft used.
We reported the universal good care practice that every patient was subjected to before going to the operating room.
We deï¬ned patients under prophylactic antibiotic those who received intraoperative antibiotic or patients who were under antibiotic therapy at the time of surgery.
All patients underwent longitudinal incision for femoral cutdown.
Past medical history of diabetes mellitus, hypertension, cerebrovascular disease, coronary artery disease, smoking including both current and former smokers (>6 months), end-stage renal disease on hemodyalisis and history of kidney transplant, were recorded.
The diagnostic criteria for SSI included signs/symptoms of infection (pain, tenderness, erythema and/or swelling), purulent drainage from the wound and organisms isolated from aseptically smears cultures of ï¬uid or tissue.
Wound site infections over a 30-day period were registered and graded based on Szilagyi classiï¬cation.5 Grade I infections had only dermal involvement. Grade II infections extended to the subcutaneous region and included dehiscence of wound. Infections involving arterial graft were grade III. Patients with hematomas and noninfected lymphoceles were also accounted.
On patients with documented groin infection it was registered the presentation timing, modality of treatment (surgical and non-surgical) and time of healing.
Data were entered in Microsoft Excel 2010 and analyzed by using SPSS 18.0 version software.
Results
From January to December 2013, 1266 vascular surgeries were performed at our central operating rooms. Of these, 782 were arterial vascular procedures, 279 by inguinal approach, with a total of 358 groin incisions. Our base population had 241 patients (31 patients with more than one procedure in a year). Demographics and clinical characteristics of our population are presented in Table 1.
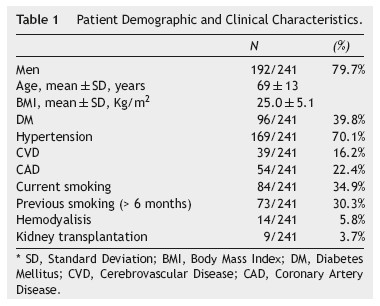
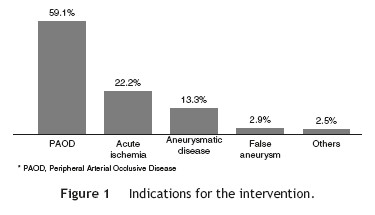
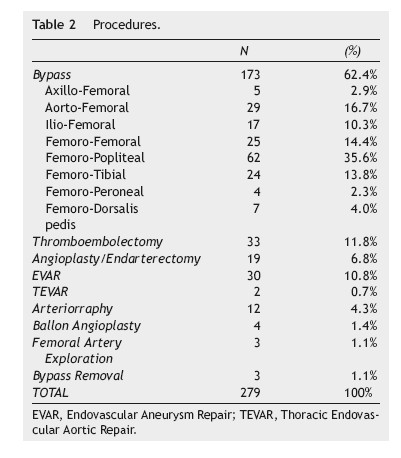
In Figure 1, we illustrated the indications for the 279 interventions, and in Table 2 we listed the procedures performed. A graft prosthesis was used in 114 of the 173 bypass surgeries (65.9%). Once the patient was considered infected, no more procedures were included in our series. The perioperative characteristics are described in Table 3.
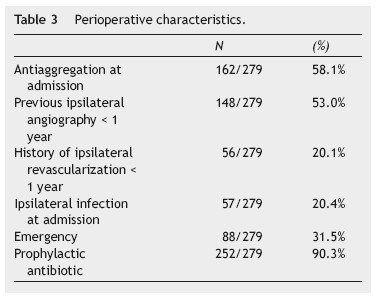
All patients received the universal good care practice before surgery: previous bath with clorohexidine, trichotomy immediately before surgery, skin antisepsis with alcoholic solution, intraoperative glove change, closed suction drain placement, careful haemostasis and layered closure. Prophylactic antibiotic was administered to 90.3% of the patients.
Total infection rate was 4.7% (17/358 groins incisions), representing complication in 16 out of the 279 procedures (5.7%). One patient had bilateral groin involvement. There were 4 patients (4 groins) who had Szilagyi I infection, 9 patients (10 groins) with Szilagyi II and 3 patients (3 groins) with Szilagyi III infection.
The demographics, clinical and preoperative characteristics of both infection and control group were compared and listed in Table 4. Hypertension was signiï¬cantly associated with a higher risk of SSI (p = 0.033).
The time to presentation with infection ranged from 2 to 25 days (mean, 13 ± 8). Incidence of infection by type of procedure was described in Table 5.
Previous revascularization with open surgery involved the ipsilateral inguinal area in 18.8% of the infected patients (3/16) and 56.3% had a history of previous femoral artery puncture (9/16).
Identiï¬cation of the infecting agent was possible only in 9/16 patients. The most common isolated agent was Pseudomonas aeruginosa (3/16).
All infections were described in Table 6. Empiric antibiotic treatment was instituted after clinical diagnosis of wound infection. All Szilagyi I resolved with antibiotic only; Three patients with Szilagyi II infections needed drainage/debridement on operation room the others Szilagyi II resolved with antibiotic and wound care. All Szilagyi III were treated with bypass removal, and in two patients, an in situ revascularization was performed. These two patients died from sepsis.
Other wound complications were registered and mentioned in Table 7.
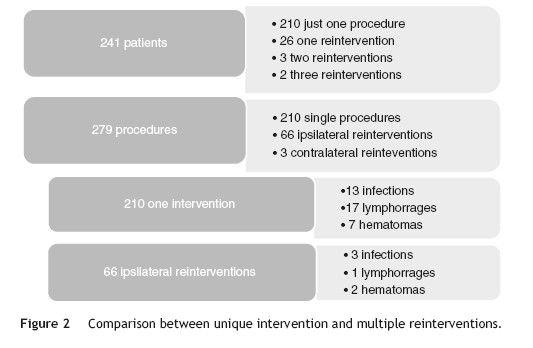
As redo operations are a consistent risk factor for surgical site infections, we compared the infection rates according to the number of reinterventions (Figure 2). Three out of 31 reoperated patients were subjected to contralateral procedures, so they were not truly redo operations and were excluded, leaving 28 redo patients to compare with 210 patients treated with just one procedure during 2013. Subgroup analysis showed that hemodialysis was a risk factor for reintervention (5/28 vs 8/210, p = 0.002). As for complications after reintervention, we had 3/66 infections, 1/66 lymphorrage and 2/66 hematomas. No statistically signiï¬cant difference was found in the outcomes between re-operated patients and one-time operated patients.
Discussion
Most wound complications (hematoma, seroma and dehiscence) and superï¬cial infections of surgical site are easily treated, but frequently neglected by the vascular surgeon.
However, they are assumed risk factors for deeper infections extending to the graft, which are associated with catastrophic consequences: death rate between 15 to 75% and major amputations rate up to 70%.11 Even when the treatment is successful, the morbidity associated with vascular graft infection is considerable, the outcomes often being worse than the natural history of the vascular condition that led to graft implantation.2 Vascular surgeons should maintain a low threshold for proceeding with additional diagnostic testing when any symptom or sign suggests graft infection.
In a case-controlled study reported by Antonios et al., multivariate analysis identiï¬ed only groin incision and wound infection as factors increasing the risk of subsequent vascular graft infection.12 Dennis F Bandyk added that, for the vascular patient, obesity, advanced age, smoking and diabetes were characteristics that potentiate SSI.1 In our study we found that hypertension rate was higher in patients that got infection (p = 0.03), but no other study found this correlation.
We had an incidence of SSI at the groin after vascular procedures of 4.7%: a good mark comparing with an overall incidence described in the range of 3 to 44%.3 However, a possible explanation for the differences in the reported incidence could be the deï¬nition of SSI used.
Most bacterial infections occur from direct spread of bacteria from the wound surface.4 Therefore, our focus must be in the prevention of surgical site infection. In our center antibiotic prophylaxis was administered to 90.3% of the patients. There is clear evidence that this is effective for SSI prevention in vascular surgery. Other protocol prophylactic measures used (previous bath with chlorhexidine, trichotomy immediatly before surgery, skin antisepsis with alcoholic solution, intraoperative glove change, closed suction drain placement, careful hemostasis and layered closure) are recommended but do not have the same level of evidence.4
The prophylactic antibiotic of choice in our department is cefazolin.13,14 Cefazolin is a ï¬rst-generation, low cost, low toxicity cephalosporin, active against methicillin-sensitive Staphylococcus aureus, coagulase negative Staphylococcus and some Gram-negative bacilli. The initial dose is twice the usual (usually 1-2 g EV) and, in longer surgeries, booster doses are administered every 4 hours. Cefazolin is administered 60 minutes before surgery and administration is completed before incision. In patients already under antimicrobial treatment an extra dose 60 minutes before the surgical incision is administered.
We signalized a history of arterial puncture at the site of infection in 56.3% of the patients that develop SSI. The signiï¬cant association described elsewhere between preoperative inguinal arteriography and groin infection conï¬rms the necessity of adopting speciï¬c preventive measures to avoid the high morbidity and mortality inherent to this vascular surgery complication.15
Recently, negative pressure dressing combined with standard perioperative infection prevention has shown to signiï¬cantly decrease the incidence of groin SSIs in patients undergoing vascular procedures in one single center.3
Although virtually any microorganism can infect a vascular prosthesis, S. aureus is the most prevalent pathogen and accounts for one fourth to one half of the infections depending on the implant site. Early infections are caused by virulent hospital-acquired bacteria and frequently associated with sepsis, as evidenced by fever, leukocytosis, bacteremia and an advanced wound infection. Late infections result from graft colonization by low-virulence organisms such as Staphylococcus epidermiditis. The low titer of microorganisms on graft surfaces produces an indolent infection without signs of sepsis, and cultures of perigraft ï¬uid or tissue may yield no growth. Although typically less virulent, these infections are more established and difï¬cult to eradicate locally.2 In our study, the highest incidence of infection with more aggressive pathogens was coincident with the characteristics of early infections and may support that prevention measures applied were effective in preventing wound infection by commensal bacteria of the skin ï¬ora.
The empirical antibiotic therapy should cover methiclinresistant S. aureus and gram negative bacilli. Associations with beta lactams, daptomycin or vancomycin and aminoglycosides seems the best option.17 Among the anti-staphylococcal drugs available, the preference for daptomycin, rather than vancomycin, has been growing due to its bactericidal activity, ability to prevent bacterial adhesion, capacity to penetrate into bioï¬lm and to prevent the formation of bioï¬lm itself.16 A synergistic effect when used with rifampin has been described.17
Multiple surgical treatment modalities have been attempted with limited success and increased health care costs, including rotational ï¬aps, wound vacuum-assisted closure and excision of prostheses with extra-anatomic bypass. In femorodistal bypass, in the absence of bleeding or severe sepsis, aggressive local treatment with debridement and drainage of localized collections, bactericidal broad-spectrum antibiotics and use of muscle ï¬aps, was associated with lower rates of limb amputation and with reinfection and mortality rates similar to conventional therapy which involves the excision of the graft, with or without arterial reconstruction.6,18,19 In our study, the two patients with graft infection and in whom revascularization was tried, did not survive. These two fatal results are a red ï¬ag for the devastating consequences that may arise from surgical site infection, and may be a stop to endless revascularization attempts.
Conclusions
In addition to showing our low incidence rate of groin SSI, this study offers the opportunity to review risk factors, preventive measures and therapeutic modalities in vascular infections. Our rate of groin infection is consistent with the best international reports. Strategies for infection control reï¬ned over years may contribute to these excellent results. The difï¬culty in establishing a correlation between infection/risk factors and infection/preventing measures results from the low incidence of groin infection and the necessity for longer follow-up periods
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Conï¬dentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
References
1. Bandyk DF. Vascular surgical site infection: risk factors and preventive measures. Semin Vasc Surg. 2008;21(3):119-23. [ Links ]
2. Cronenwett JL, Johnston WK. Rutherfordâs Vascular Surgery. Philadelphia: Elsevier. 2014:654-72. [ Links ]
3. Matatov T, Reddy KN, Doucet LD, et al. Experience with a new negative pressure incision management system in prevention of groin wound infection in vascular surgery patients. J Vasc Surg. 2013;57(3):791-5. [ Links ]
4. Stewart AH, Eyers PS, Earnshaw JJ. Prevention of infection on peripheral arterial reconstruction: a systematic review and meta-analysis. J Vasc Surg. 2007;46(1):148-55. [ Links ]
5. Szilagyi DE, Smith RF, Elliott JP, et al. Infection in Arterial Reconstruction with Synthetic Grafts. Ann Surg. 1972;176(3): 321-33. [ Links ]
6. Siracuse JJ, Nandivada P, Giles KA, et al. Prosthetic graft infections involving the femoral artery. J Vasc Surg. 2013;57(3):700-5. [ Links ]
7. Engin C1, Posacioglu H, Ayik F, et al. Management of vascular infection in the groin. Tex Heart Inst J. 2005;32(4): 529-34. [ Links ]
8. Dosluoglu HH, Loghmanee C, Lall P, et al. Management of early (<30 day) vascular groin infections using vacuum-assisted closure alone without muscle ï¬ap coverage in a consecutive patient series. J Vasc Surg. 2010;51(5):1317. [ Links ]
9. Mohammed S, Pisimisis GT, Daram SP, et al. Impact of intraoperative administration of local vancomycin on inguinal wound complications. J Vasc Surg. 2013;57(4):1079-83. [ Links ]
10. Monsen C, Wann-Hansson C, Wictorsson C, et al. Vacuum-assisted wound closure versus alginate for the treatment of deep perivascular wound infections in the groin after vascular surgery. J Vasc Surg. 2014;59(1):145-51. [ Links ]
11. Legout L, DâElia PV, Sarraz-Bournet B, et al. Diagnosis and management of prosthetic vascular graft infections. Med Mal Infect. 2012;42(3):102-9. [ Links ]
12. Antonios VS, Noel AA, Steckelberg JM, et al. Prosthetic vascular graft infection: a risk factor analysis using a case-control study. J Infect. 2006;53(1):49-55. [ Links ]
13. Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health-Syst Pharm. 2013;70:195-283. [ Links ]
14. European Centre for Disease Prevention and Control. Systematic review and evidence-based guidance on perioperative antibiotic prophylaxis. doi 10.2900/85936. June 2013. [ Links ]
15. Cano E, Baquer M, Carnicero JÃ, et al. Relationship Between Preoperative Inguinal Arteriography and Groin Infection after Arterial Surgery. CirugÃa EspaËnola. 2001;69(6):557-9.
16. Edmiston CE Jr, Goheen MP, Seabrook GR, et al. Impact of selective antimicrobial agents on staphylococcal adherence to biomedical devices. Am J Surg. 2006;192(3):344-54. [ Links ]
17. Cirioni O, Mocchegiani F, Ghiselli R, et al. Daptomycin and rifampin alone and in combination prevent vascular graft bioï¬lm formation and emergence of antibiotic resistance in a subcutaneous rat pouch modelo of Staphylococcal infection. Eur J Vasc Endovasc Surg. 2010;40:817-22. [ Links ]
18. Cherry KJ, Roland CF, Pairolero PC, et al. Infected femorodistal bypass: is graft removal mandatory? J Vasc Surg Feb. 1992;15(2):295-305. [ Links ]
19. Ministro A, Evangelista A, Damião A, et al. Infeção protésica infra-inguinal em cirurgia vascular. A propósito de um caso clÃnico. Rev Port Cir Cardiotorac Vasc. 2011;18(4):243-8. [ Links ]
Correio eletrónico: tgabrielateixeira@gmail.com (G. Teixeira).
Received 30 October 2014;
Accepted 3 December 2014
Available online 11 March 2015

