










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versión impresa ISSN 1646-706X
Angiol Cir Vasc vol.15 no.4 Lisboa dic. 2019
CASOS CLÍNICOS
Coil embolisation of ruptured left gastric artery aneurysm
Embolização de aneurisma em rotura da artéria gástrica esquerda
Mário Moreira1, Alfredo Gil Agostinho2, Joana Moreira1, Luís Antunes1, Manuel Fonseca1
1 Angiology and Vascular Surgery Department, Centro Hospitalar e Universitário de Coimbra
2 Radiology Department, Centro Hospitalar e Universitário de Coimbra
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Visceral artery aneurysms are rare, with an estimated incidence of less than 2% in the general population. Left gastric artery aneurysm are particularly uncommon, accounting for 4% of all visceral aneurysms. Usually an incidental finding, they can manifest with rupture and be life threatening. The authors present a case of an 83 year-old male with haemorrhagic shock caused by a ruptured left gastric artery aneurysm. Coil embolization of afferent and efferent arteries was performed with good morphologic results. Management of a ruptured visceral aneurysm is aimed at controlling life-threatening bleeding usually by embolisation in the emergency setting.
Keywords: Left gastric artery; Aneurysm; Rupture
RESUMO
Os aneurismas das artérias viscerais são raros, com uma incidência inferior a 2% na população geral. O aneurisma da artéria gástrica esquerda é particularmente incomum, representando menos de 4% dos aneurismas viscerais. Apesar de geralmente serem descobertos incidentalmente, podem apresentar-se em rotura e com risco vital associado. Os autores apresentam o caso de um indivíduo do sexo masculino, 83 anos, em choque hemorrágico secundário a aneurisma em rotura da artéria gástrica esquerda. Foi realizada embolização das artérias eferente e aferente. O tratamento de aneurismas viscerais em rotura tem como objectivo o controlo emergente da hemorragia, geralmente através de embolização.
Palavras-chave: Artéria gástrica esquerda; Aneurisma; Rotura
Introduction
Visceral artery aneurysms are exceedingly rare, with an estimated incidence of less than 2% in the general population. Within visceral artery aneurysms, left gastric artery aneurysm are particularly uncommon(1,2). Most visceral artery aneurysms are atherosclerotic. Other pathologies implicated in the etiology are medial wall degeneration and vasculitis as well as a variety of conditions including Marfan's, Ehlers-Danlos and Osler-Weber-Rendu syndromes, fibromuscular dysplasia, Kawasaki disease and hyperflow conditions such as portal hypertension and pregnancy. Surrounding inflammation secondary to prior pancreatitis, peptic ulcer disease or hepatitis has been considered an additional possible contributing factor to left gastric artery aneurysm in particular. Usually an incidental finding, they can manifest with rupture (around 1 out of 4) which be life threatening. Current treatment options include open and endovascular techniques; considering the very low prevalence, there are no guidelines for management. The authors present a case of this rare and serious condition.
Case report
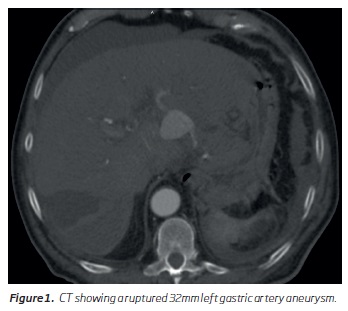
Male, 83 year-old, admitted at another institution, complaining of fever and diffuse upper abdominal pain. His past medical history included hypertension. He was diagnosed acute calculous cholecystitis after blood sample analysis and abdominal ultrasound and admitted under antibiotics. On sixth hospital day, the patient complained of intense and sudden pain in the upper abdomen and manifested signs of hypovolemic shock (blood pressure of 40mmHg, heart rate 122). Computerized tomography showed a ruptured 32mm left gastric artery pseudoaneurysm (Figure 1).
The patient was transferred with haemorrhagic shock to our institution and taken to the angiosuite. Percutaneous right femoral access was obtained (5F). Catheterisation of left gastric artery (Figure 2) was performed using a 0.018 inch guidewire (Terumo®) supported by a 4F 100cm Simmons-1® catheter (Merit Medical®).

Then a 2.7F microcatheter (Progreat®) was placed in the distal left gastric artery and microcoils (Tornado®) were gradually deployed in the outflow and inflow vessels of the aneurysm (Figure 3).

Catheterization of pseudoaneurysm was unsuccessfully attempted. The procedure was uneventful. Good morphological results were achieved, with aneurysm exclusion and no antegrade or retrograde flow into aneurysm sac. Computerized tomography was performed on postoperative day 2 and aneurysm exclusion was confirmed. The patient improved gradually and was discharged to his local hospital on postoperative day 4. Patient remains asymptomatic at 12 months.
Discussion
Aneurysmal degeneration of visceral arteries is uncommon and rarely involve gastric arteries. However, rupture of left gastric aneurysm is a serious condition. Approach to a ruptured visceral aneurysm encompass life-threatening bleeding control with vigorous resuscitation and effective aneurysm exclusion. Intervention mainly consists of minimally invasive endovascular techniques, usually by transarterial coil embolisation in the emergency setting. The procedure should address embolisation of both the efferent and afferent vessels along with coil deployment inside the sac when possible. Proximal embolisation alone is not recommended neither in elective nor in emergent cases; in rupture aneurysms, proximal embolisation do not stop bleeding; in asymptomatic ones, robust retrograde vascular supply may occur, with aneurysm growth and no possibility of antegrade vascular access to the aneurysm. Transcutaneous CT guided aneurysm exclusion has also been described(3).
Regarding the etiology of the aneurysm, the case we report is quite intriguing. Taking in account blood analysis and ultrasound findings, cholecystitis as initial diagnosis seems unquestionable. Left gastric artery pseudoaneurysms are usually associated with surrounding inflammation secondary to pancreatitis or peptic ulcer disease; coincidental cholecystitis has been reported(4) but with concurrent pancreatitis which is not observed in our case. Isolated cholecystitis and visceral pseudoaneurysms was previous reported(5) but cystic artery was the affected vessel.
Conclusion
Despite its rarity, visceral aneurysm rupture should be considered in the differential diagnosis of unexplained hemorrhagic shock particularly when intrabdominal inflammatory process is present.
REFERENCES
1. Barrionuevo P, Malas MB, Nejim B, Haddad A, Morrow A, Ponce O, et al. A systematic review and meta-analysis of the management of visceral artery aneurysms. J Vasc Surg. 2019 May 21. (Epub ahead of print; doi: 10.1016/j.jvs.2019.02.024 ). [ Links ]
2. Nishimura T, Sakata H, Yamada T, Osako T, Kohama K, Kako Y, et al. Hemorrhagic shock due to ruptured left and right gastric artery aneurysm. Acute Medicine & Surgery. 2016;3: 39-42. (doi: 10.1002/ams2.115 ). [ Links ]
3. Chandran S, Parvaiz A, Karim A, Ghafoor I, Steadman B, Pearce NW, et al. Ruptured Left Gastric Artery Aneurysm Successfully Treated by Thrombin Injection: Case Report and Literature Review. Sci World J. 5(2005):20-23. (doi: 10.1100/tsw.2005.8 ). [ Links ]
4. Valluru B, Yang B, Sharma K, Adam AA, Wei D, Zhou Z, et al. Significance of radiology in the diagnosis and management of ruptured left gastric artery aneurysm associated with acute pancreatitis. Medicine. 2019 Mar. 98(10): e14824. (doi: 10.1097/MD.0000000000014824 ). [ Links ]
5. Saluja SS, Ray S, Gulati MS, Pal S, Sahni P, Chattopadhyay TK. Acute cholecystitis with massive upper gastrointestinal bleed: A case report and review of the literature. BMC Gastroenterol. 2007 Mar; 7:12. (doi: 10.1186/1471-230X-7-12 ). [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Correio eletrónico: mariodpmoreira@gmail.com (M. Moreira).
Recebido a 09 de outubro de 2019
Aceite a 03 de dezembro de 2019

