Clinical Case
Renal autotransplantation: a solution for different complex situations
Autotransplante renal: uma solução para situações complexas diversas
Pedro Pinto Sousa1
Pedro Sá Pinto1
Rui Machado2
Rui Almeida2
1. Serviço de Angiologia e Cirurgia Vascular; Centro Hospitalar de Vila Nova de Gaia/Espinho; Vila Nova de Gaia; Portugal
2. Serviço de Angiologia e Cirurgia Vascular; Centro Hospitalar do Porto; Porto; Portugal
Abstract
Introduction:
Renal autotransplantation (RA) is a safe and effective procedure to reconstruct the urinary tract which first successful surgery was performed by Hardy in 1963. The main indications reported to perform a RA generally include renovascular disease, ureteral pathologies and neoplastic disease. Furthermore, RA may be useful as an ultimate recourse in preventing kidney loss in highly selected patients, especially when conventional methods have failed.
Materials and Methods:
The authors describe four total different situations where the RA was the key solution for the pathology initially presented.
Clinical case I - A 52 years old male with a previous history of left nephrectomy due to a preceding exacerbation of his basal Crohn's disease and also a right ureter cutaneostomie, presented now with repetitive urinary tract infections that led to renal function impairment;
Clinical case II - A 57 years old female with the diagnosis of renal artery aneurysm while being studied as a potential kidney donor;
Clinical case III - A 49 years old male admitted in the emergency room after a penetrating trauma which conditioned bowel and ureteral lesions with postoperative consecutive and recurrent peritoneal infections that compounded a necessity for a left ureterostomy, that the patient vehemently refused;
Clinical case IV - A 24 years old female with the diagnosis of Nutcracker syndrome identified after being studied regarding repetitive urgency admissions with frank haematuria.
Results:
Every patient was submitted to laparoscopic nephrectomy, ex-vivo reconstruction, if necessary, and kidney transplantation to the iliac fossa. The interventions were uneventful and only one patient faced a minor post-operative complication (surgical wound dehiscende). We performed an ultrasound and renal scintigraphy evaluation on following days after each procedure to attest normal renal perfusion.
Discussion:
The RA were conducted in two patients with ureteral cutaneostomie because there was no viable alternative but kidney loss. The other two clinical cases were treated with RA because they concerned a complex renovascular disease (one arterial and the other venous). Despite the existence of an endovascular option for these patients, long term follow-up studies are still lacking.
Conclusion:
The RA is a viable option in specific situations for kidney salvage. The recent development of laparoscopic nephrectomy significantly decreased the surgical hostility to the patient and promoted the RA as a value option for the treatment of complex vascular pathologies, traumatic disease and specific medical situations. It represents a credible alternative with attested results already described in the literature thus requiring a vast Institutional experience with conventional renal transplantation.
Keywords: Renal auto-transplant; laparoscopy; Nutcracker syndrome; Renal artery aneurysm; Ex-vivo repair
Resumo
Introdução:
O autotransplante renal (RA) é um procedimento seguro e eficaz, utilizado em patologias que requeiram reconstrução do trato urinário, cujo primeira intervenção foi descrita por Hardy em 1963. As principais indicações são doença renovascular, patologias ureterais e doença neoplásica. O RA poderá ainda ser útil em casos selecionados, como último recurso na prevenção de perda renal, especialmente quando os métodos convencionais não tiveram sucesso.
Materiais e métodos:
Os autores pretendem descrever quatro diferentes situações em que o RA foi a melhor solução para a patologia apresentada pelos doentes.
Caso clínico I - Doente do sexo masculino, 52 anos de idade, com história de nefrectomia esquerda prévia e ureterostomia direita, no contexto de exacerbação da sua doença de Crohn. Apresentava-se agora, recentemente, com infeções urinárias de repetição e consequente disfunção renal;
Caso clínico II - Doente do sexo feminino, 57 anos de idade, a quem foi diagnosticado um aneurisma da artéria renal enquanto era estudada como potencial dadora para transplante renal;
Caso clínico III - Doente do sexo masculino, 49 anos de idade, admitido no Serviço de urgência vítima de trauma penetrante com atingimento abdominal e consequentes lesões ureterais e do trato intestinal. Submetido a laparotomia com reconstrução das mesmas, mas posteriores peritonites de repetição que condicionaram necessidade de ureterostomia que o doente recusava;
Caso clínico IV - Doente do sexo feminino, 24 anos de idade, com o diagnóstico de Síndrome de Nutcraker após estudo realizado na sequência de admissão no Serviço de urgência com hematúria franca.
Resultados:
Todos os doentes foram submetidos a RA. As intervenções cirúrgicas decorreram sem intercorrências com apenas um doente a ter desenvolvido uma complicação (deiscência de ferida cirúrgica) no período pós-operatório. Foi realizado ecoDoppler e cintigrafia renal nos dias subsequentes ao procedimento que atestou a normal perfusão dos rins transplantados.
Discussão:
O RA foi realizado em dois doentes no contexto de lesões ureterais e perante a ausência de tratamento viável alternativo que não a perda do rim. Os outros dois casos ocorreram no contexto de patologias renovasculares complexas (uma arterial e outra venosa). Apesar da existência de opções endovasculares para estes casos, a publicação de resultados de seguimento a longo prazo ainda é escassa.
Conclusão:
O RA é uma opção viável em situações específicas em que é imperial a salvação do rim. Os avanços recentes com nefrectomia laparoscópica vieram reduzir de forma significativa a agressividade do procedimento cirúrgico, promovendo o RA como uma arma de tratamento de real valor no tratamento de patologias vasculares complexas, doença renovascular e ureteral traumática bem como situações médicas específicas. O RA representa assim, uma alternativa credível com resultados demonstrados e publicados, exigindo, contudo, ser realizado num Centro com elevada experiência institucional.
Palavras-chave: Autotransplante renal; laparoscopia; Síndrome de nutcracker; Aneurisma da artéria renal; Reparo ex vivo
Introduction
Hardy firstly described the renal auto-transplant in 19631. The procedure was performed to repair a high ureteral injury sustained during aortic surgery, where there was a re-implantation of the kidney into the ipsilateral iliac fossa. Since then, indications for auto-transplant were extended.
In addition to complex ureteral reconstruction, renal auto-transplant has been performed for renovascular diseases such as renal artery aneurysms and nutcracker syndrome and may be also suitable for treating neoplastic disease and other specifi medical kidney diseases.
The renal auto-transplant is, nowadays, at our Department a frequent performed procedure.
The institutional experienced associated with the recent further technical developments, such as the advent of laparoscopic nephrectomy combined with extracorporeal repair of the ureteral or vascular anomalies, has induced less morbidity and hostility with the intervention.
Materials and methods
The authors collected the data, medical and surgical registries of four patients with complex pathologies requiring RA. Intervention outcomes and follow-up was analysed and hereafter described.
Clinical case I - A 52 years old female with a personal history of Crohn's disease that had been, previously, submitted to left nephrectomy and right ureterostomy, both in the setting of disease exacerbations. Recently, she developed repetitive urinary infections that caused significant and progressive renal function impairment (Fi. 1 and 2).
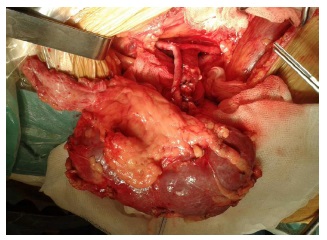
Clinical case II - A 57 years old female, to whom a renal artery aneurysm, localized on the renal artery bifurcation, was diagnosed, while she was being studied for a potential kidney donor (Fig. 3).
Clinical case III - A 49 years old male that experienced an abdominal penetrating trauma with bowel and ureteral lesions submitted to open laparotomy for urinary and intestinal tract reconstruction but required a permanent right ureterostomy that the patient refused.
Clinical case IV - A 24 years old female with multiple urgency admissions with frank hematuria requiring long-term blood product transfusion support. Following imagiological study, a nutcracker syndrome was diagnosed (Fig. 4 and 5).
Results
All the four patients were submitted to laparoscopic nephrectomy, kidney cooling with Celsius solution, ex-vivo reconstruction whenever necessary, kidney implantation in the iliac fossa with vascular anastomosis to the external iliac vessels and ureterocistostomy following the Paquin technique. In the third clinical case, we complemented the procedure with ex-vivo reconstruction ensuing a total aneurismectomy and end to end anastomosis.
In all four cases, a 3-port trans-peritoneal approach was used with a muscle splitting Gibson incision for renal extraction and then we implanted the auto-transplant on the iliac fossa, according to the technique above described. No technical or surgical complications were reported. Total mean operative time was five hours and 52 minutes, and average laparoscopic donor nephrectomy time was one hour and 48 minutes. Mean renal warm ischemia time (from endoscopic clamping of the renal artery to ex vivo cold perfusion) was 4 minutes. Mean hospital stay was 11.5 days. No significant difference was found between preoperative and postoperative plasma creatinine levels (p=0.78). Inclusively, the first clinical case presented a renal function recovery after the procedure. Postoperative imaging study indicated good perfusion to the transplanted kidneys.
Concerning the post-operative period, we registered, in the third clinical case, a minor complication with wound infection and dehiscence that was handled with surgical revision and antibiotic treatment.
The post-operative period on the other three patients was uneventful. Patients have now a mean 4,3 years of follow up with a well-functioning kidney and normal renal function.
Discussion
Literature has already attested RA as an effective and safe procedure, for specific and complex situations like the ones above described. Advancements in laparoscopic techniques have yet improved this procedure once it brought even less morbidity to the patient.
The authors report the use of laparoscopy as an adjunctive to the auto-transplant procedure by combining laparoscopic nephrectomy with ex-vivo repair of the vascular and ureteral lesions presented by the patients, followed by renal auto-transplant into the iliac fossa and anastomosis to the external iliac vessels.
Gil Inderbir et all and Bluebond et all have one of the largest series published for renal auto-transplantation with hand assisted nephrectomy, with both four cases presented2,3.
Addressing only to the cases exposed, ureteral injuries are rare but sometimes present with some complexity and high failure rates after conventional repair4-8. They normally occur in conjunction with preserved renal parenchyma, therefore, their repair and kidney salvage is desirable. Conventional techniques include ureteroureterostomy, psoas hitch procedure, Boari flap, transureteroureterostomy, or transureteropyelostomy reconstruction. Nevertheless, these techniques cannot be used in severe ureteral loss or high ureteral injury. Bodie et al9 already reported 23 patients receiving auto-transplant for substantial ureteral loss. On his study, he demonstrated excellent long-term results with renal function preserved in 93% patients during 14-year follow-up. Despite some others reports indicating a high rate of perioperative renal loss, when done by a skilled team, excellent results may be obtained.
On the other hand, the topic renovacular disease, is still leading the vast majority of indications for these procedure accounting for 60-80% of the treated cases10-11. Most of the published literature represents only case reports with treatment modalities for renal artery aneurysms including surgical and endovascular techniques. The choice, between them, in our experience, is essentially determined by the anatomical site and aneurysm morphology. Ex-vivo surgery allows for adequate exposure and repair of the aneurysm with clear long-term results already published in the literature. Brekke reported 21 cases of renal auto-transplant for RAA. They had no organ loss after an average 4.3 years' follow-up12. Mahmoud Alameddine et al13 also described four patients diagnosed with renal artery aneurysms who underwent reconstruction of the allograft before serving as kidney donors with excelente results. In clinical case III, we present a Poutasse Type I and Rundback Type II renal artery aneurysm that, according to the literature, is best treated with renal auto-transplant and aneurysm repair, that is why we believe a good treatment option was made.
Concerning the Nutcracker Syndrome, also various surgical and endovascular options exist14-15. In our case, auto-transplantation was considered a more complete procedure as it also corrected the concomitant posterior ptosis, which is frequent, as already described in the literature. Waqas Javed Siddiqui et al published an article where he presented three cases and did a literature revision. We agree with that data when arguing that treatment options diverge from simple close observation, intervention with open or endovascular procedures till nephrectomy. But we believe that surgery with renal auto-transplant is the only definite option with already attested results on long term follow-up.
Following everything above displayed, the authors believe that, since we have an extended experience in conventional renal transplantation with cadaveric and live donor, and also with already attested results with auto-transplant, the cases presented, despite challenging, were feasible, showing renal auto-transplant as a viable option. We publish this article based on our vast Institutional experience with more than 2.000 kidney transplants accomplished.
References
1. HARDY, J.D.: "High ureteral injuries. Management by autotrasplantation of the kidney". JAMA, 84: 97, 1963
[ Links ]
2. GILL INDERBIR, S.; UZZO, R.G.; HOBART, M.G. y cols.: "Laparoscopic retroperitoneal live donor right nephrectomy for purposes of allotransplantation and autotransplantation". J. Urol., 164: 1500, 2000.
[ Links ]
3. BLUEBOND-LANGNER, R.; RHA, K.H.; PINTO, P.A. y cols.: "Laparoscopic-assisted renal autotransplantation". Urology, 63: 853, 2004
[ Links ]
4. Bleicher J, Kim RD, Hamilton B, Lau G, Campsen J; Backtable ureteroscopy for retrieval of retained stent or stone: A novel technique in renalautotransplant; Urol Case Rep. 2018 Jan 28;17:94-96. DOI: https://doi.org/10.1016/j.eucr.2018.01.010. eCollection 2018
[ Links ]
5. Salamanca-Bustos JJ, Gomez-Gomez E, Campos-Hernández JP, Carrasco-Valiente J, Ruiz-García J , Márquez-López FJ; Initial Experience in the Use of Novel Auto-expandable Metal Ureteral Stent in the Treatment of Ureter Stenosis in Kidney Transplanted Patients; Transplant Proc. 2018 Mar;50(2):587-590. DOI: https://doi.org/10.1016/j.transproceed.2017.09.048
[ Links ]
6. Strategies for open reconstruction of upper ureteral strictures; Knight RB1, Hudak SJ, Morey AF; Urol Clin North Am. 2013 Aug;40(3):351-61. DOI: https://doi.org/10.1016/j.ucl.2013.04.005. Epub 2013
[ Links ]
7. Kidney autotransplantation: long-term outcomes and complications. Experience in a tertiary hospital and literature review; Ruiz M, Hevia V, Fabuel JJ, Fernández AA, Gómez V, Burgos FJ; Int Urol Nephrol. 2017;49(11):1929-1935. DOI: https://doi.org/10.1007/s11255-017-1680-1. Epub 2017
[ Links ]
8. Kamel MH1, Thomas AA, Mohan P, Hickey DP; Renal vessel reconstruction in kidney transplantation using a polytetrafluoroethylene (PTFE) vascular graft; Nephrol Dial Transplant. 2007;22(4):1030-2. Epub 2007 Jan 8
[ Links ]
9. Bodie B, Novick AC, Rose M, Straffon RA; Long-term results with renal autotransplantation for ureteral replacement; J Urol. 1986;136(6):1187-9
[ Links ]
10. Renal autotransplantation: a valid option in the resolution of complex cases; López-Fando Lavalle L, Burgos Revilla J, Sáenz Medina J, Linares Quevedo A, Vallejo Herrador J, De Castro Guerin C, Pascual Santos J, Marcén Letosa R.; Arch Esp Urol. 2007;60(3):255-65
[ Links ]
11. Kim MJ, Lee KW, Park JB, Kim SJ; Hand-Assisted Laparoscopic Nephrectomy and Auto-Transplantation for a Hilar Renal Artery Aneurysm: A Case Report; Vasc Specialist Int. 2017 Jun;33(2):84-87. DOI: https://doi.org/10.5758/vsi.2017.33.2.84. Epub 2017 Jun 30
[ Links ]
12. Brekke IB, Sødal G, Jakobsen A, et al. Fibro-muscular renal artery disease treated by extracorporeal vascular reconstruction and renal autotransplantation: short- and long-term results. Eur J Vasc Surg. 1992;6(5):471-476
[ Links ]
13. Alameddine M, Moghadamyeghaneh Z, Guerra G, Morsi M, Osman M, Chia VJ, Burke GW, Chen L, Vianna R, Zheng I, González J, Ciancio G; Case series: Transplantation of kidneys from donors with renal artery aneurysm; Can Urol Assoc 2017 Jul;11(7):E307-E310. DOI: https://doi.org/10.5489/cuaj.4244. Epub 2017
[ Links ]
14. Siddiqui WJ, Bakar A, Aslam M, Arif H, Bianco BA, Trebelev AE Kelepouris E, Aggarwal S; Left Renal Vein Compression Syndrome: Cracking the Nut of Clinical Dilemmas - Three Cases and Review of Literature; Am J Case Rep. 2017;18:754-75
[ Links ]
15. Waqas Javed Siddiqui; Left Renal Vein Compression Syndrome: Cracking the Nut of Clinical Dilemmas - Three Cases and Review of Literature; Am J Case Rep. 2017; 18: 754-75
[ Links ]












 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink