










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Portuguesa de Nutrição
versão On-line ISSN 2183-5985
Acta Port Nutr no.7 Porto dez. 2016
https://doi.org/10.21011/apn.2016.0702
ARTIGO ORIGINAL
Prevalence of Overweight and Obesity in 2-6 Years Old Children from a Kindergarten
Prevalência de Excesso de Peso e Obesidade em Crianças dos 2 aos 6 Anos Frequentadoras de um Jardim de Infância
Alex Pinto1,2; Henrique Figueiredo1; Maria J Ramos1; Jorge Ferreira1,3; Júlio C Rocha1,2,4,5*
1Centro de Apoio Social de Mozelos, Alameda Alfredo Henriques, n.º 89, 4535-159 Mozelos, Portugal
2Centro de Genética Médica, Centro Hospitalar do Porto,nPraça Pedro Nunes, n.º 88, 4099-028 Porto, Portugal
3Unidade de Cuidados de Saúde Personalizados de Mozelos, ACES Feira/Arouca, Alameda Alfredo Henriques, n.º 107, 4535-159 Mozelos, Portugal
4Faculdade de Ciências da Saúde, Universidade Fernando Pessoa, Rua Carlos da Maia, n.º 296, 4200-150 Porto, Portugal
5Center for Health Technology and Services Research (CINTESIS), Rua Dr. Plácido da Costa, s/n, 4200-450 Porto, Portugal
ABSTRACT
Introduction: Childhood overweight and obesity is a worldwide concern. Physical activity and food patterns are main factors associated with overweight at preschool age. Centro de Apoio Social de Mozelos is a kindergarten where food habits have been supervised by a nutritionist and where physical activity is freely offered to all children aged 2 to 6 years old. Objectives: This study aimed to investigate the prevalence of overweight and obesity in children aged 2 to 6 years old. Methodology: A sample of 129 children from Centro de Apoio Social de Mozelos (3.7±1.2 years old) was studied. Anthropometric measurements were performed in children and parents. A questionnaire for sample characterization was answered by parents. Overweight and obesity were defined using World Health Organization criteria. Results: The global prevalence of overweight and obesity in children was 11.7% (7.8% of overweight; 3.9% of obesity). Overweight and obesity prevalence in parents was 57.8% (40.5% of overweight; 17.3% of obesity). Conclusions: The prevalence of overweight and obesity in parents seems to follow the general Portuguese population. However, results found in children are below our expectations comparing to similar studies. Further longitudinal studies are needed to clearly demonstrate the benefits of a combined nutritional and physical activity management approach in kindergartens like Centro de Apoio Social de Mozelos in the prevention/reduction of overweight and obesity in preschool aged children.
Keywords
Children, Food habits, Obesity, Overweight, Physical activity, Prevalence
RESUMO
Introdução: O excesso de peso e a obesidade infantil são uma preocupação mundial. Os principais fatores associados ao excesso de peso em idade pré-escolar são o padrão alimentar e a atividade física. O Centro de Apoio Social de Mozelos é um jardim de infância onde os hábitos alimentares são supervisionados por um Nutricionista e a atividade física é oferecida gratuitamente a todas as crianças dos 2 aos 6 anos. Objetivos: Este estudo visou investigar a prevalência de excesso de peso e obesidade em crianças com idades compreendidas entre os 2 e os 6 anos. Metodologia: Estudou-se uma amostra de 129 crianças do Centro de Apoio Social de Mozelos (3,7±1,2 anos). Realizaram-se avaliações antropométricas às crianças e aos seus progenitores. Um questionário para caracterização da amostra foi realizado aos pais. Excesso de peso e obesidade foram definidos utilizando os critérios da Organização Mundial da Saúde. Resultados: A prevalência global de excesso de peso e obesidade nas crianças foi de 11,7% (7,8% de excesso de peso e 3,9% de obesidade). A prevalência de excesso de peso e obesidade nos pais foi de 57,8% (40,5% de excesso de peso e 17,3% de obesidade). Conclusões: A prevalência de excesso de peso e obesidade nos pais parece ser similar à população geral portuguesa. No entanto, os resultados encontrados nas crianças parecem estar abaixo do expectável comparando com estudos similares. São necessários mais estudos longitudinais que demonstrem claramente os benefícios da abordagem conjunta da atividade física e do padrão alimentar em jardins de infância como o Centro de Apoio Social de Mozelos na prevenção/redução do excesso de peso e obesidade em crianças com idade pré-escolar.
Palavras-chave
Crianças, Hábitos alimentares, Obesidade, Excesso de peso, Atividade física, Prevalência
INTRODUCTION
Childhood overweight (OW) and obesity (OB) is a major worldwide problem and Portugal is one of the most affected countries in Europe (1, 2). OW and OB are associated with genotypic and environmental factors (3) and it can lead to several comorbidities such as metabolic, cardiovascular and psychological disorders (4). Particularly at preschool age, OW and OB constitute a serious concern considering the higher risk of tracking until adulthood (5). Although genetic factors have been linked with excessive weight gain (6), in the great majority of OW and obese individuals, the condition is lifestyle associated (7). Several factors have been associated with OW at preschool age including prematurity, parental OB, lack of physical activity and inadequate food patterns (8). Moreover, familiar obesogenic environment has also been described as an important modulator of weight gain in children (9). The age of 3-6 years is considered a crucial moment for acquiring healthy food habits to prevent later OB (10, 11), which underlines the importance of preschool in the adoption of an healthy food pattern together with a non sedentary life-style (12). Centro de Apoio Social de Mozelos (CASM) is a kindergarten with a food pattern implemented and monitored by a nutritionist since the last 12 years. In addition, physical activity is freely offered to children at 2-6 years, twice a week and supervised by a physical education teacher.
OBJECTIVES
Our work aimed to study the prevalence of OW and OB in preschool children aged 2 to 6 years from CASM.
METHODOLOGY
Participants and data collection procedures
A cross-sectional study was developed in children from CASM, aged 2 to 6 years, during 2015 (from April until June). The initial sample included all the 167 children at this age range registered in the institution. Everyone was invited to participate in the study. Out of the 167 children, one was excluded because he was away during the study period, five did not reply and 32 refused to participate. The final sample was composed by 129 children (65 females; 50.4%) with a mean age of 3.7±1.2 years. Both parents of all children were also invited to participate. Since we aimed to use only simultaneous data of both parents, the final sample of parents was composed by 168 progenitors: 84 males (37.8±6.0 years) and 84 females (34.9±4.4 years). In children, general information was collected from CASM database, namely gender, birth date, admission date in the institution and single parenthood. Each child received a code in order to guarantee anonymity. Parents who accepted to participate were asked to bring their child’s official medical record (BSI - Boletim de Saúde Infantil) on the day they were evaluated. From the BSI, data on gestational age, weight, length and head circumference at birth was recorded. Parents that refused to participate were asked to send their child’s BSI in order to collect the referred data. Anyway, out of the 129 children, the information was only possible to be obtained in 118. Data on clinical history, follow-up by nutritionist and physical activity practiced out of CASM were also obtained from parents.
Anthropometric measurements and overweight, obesity and abdominal obesity definitions
Anthropometric measurements of children were performed by classroom, always in the morning and before lunch. Weight and height were measured wearing light-weight clothes and without shoes or adornments, using a Seca® mechanic weight scale (measured to the nearest 100 g), including a stadiometer (height measured to the nearest mm), respectively. The same anthropometric measurements were done in parents according to their availability and using the same methodology described for children’s evaluation. On these, it was also assessed waist circumference (WC), performed in standing position, midway between the lower rib margin and the iliac crest, at the end of a normal exhalation, to the nearest mm and using a non-extensive metric tape. All the instruments were frequently calibrated and cleaned throughout the study period. In children, weight, height and body mass index [BMI=weight (Kg) / height (m)2] were interpreted according with World Health Organization (WHO) growth charts. The WHO Anthro® and WHO AnthroPlus®softwares were used to calculate BMI z-scores. OW was defined when BMI z-score was between 2 and 3 SD or between 1 and 2 SD, in children aged below or above 5 years, respectively. OB was identified when BMI z-score was above 3 SD or above 2 SD, in children aged below or above 5 years, respectively (13, 14). In parents, BMI was classified according to the WHO categories: OW (≥ 25.0 – 29.9 kg/m2) and OB (≥ 30.0 Kg/m2) (15). WC cut-offs from the International Diabetes Federation were used for abdominal OB (94 cm in males and 80 cm in females) (16).
Ethical Statement
The study protocol, information letter, data collection table, and informed consent form were approved by the Ethical Committee of the Universidade Fernando Pessoa according with the report of 24th of March 2015. All parents and/or guardians gave their written informed consent.
Statistical analysis
Statistical analysis was performed using the software SPSS version 22 for Mac. Normal distribution of variables was analyzed with the Kolmogorov-Smirnov test. Categorical variables were presented as percentage and continuous variables as mean ± standard deviation (±SD). Differences between percentages were analyzed with Chi-square test. Statistical significance was set when p<0.05.
RESULTS
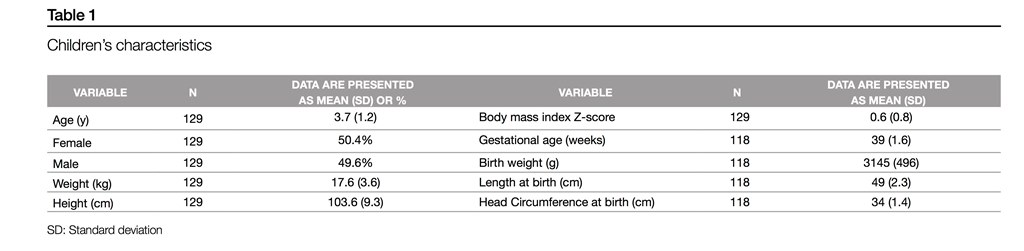
Data on age, gender and anthropometry is presented on (Table 1), together with all the data obtained from BSI. Children enrolled in the study were equally distributed across different age groups, with the exception of sub-group with 6 years of age (Figure 1).
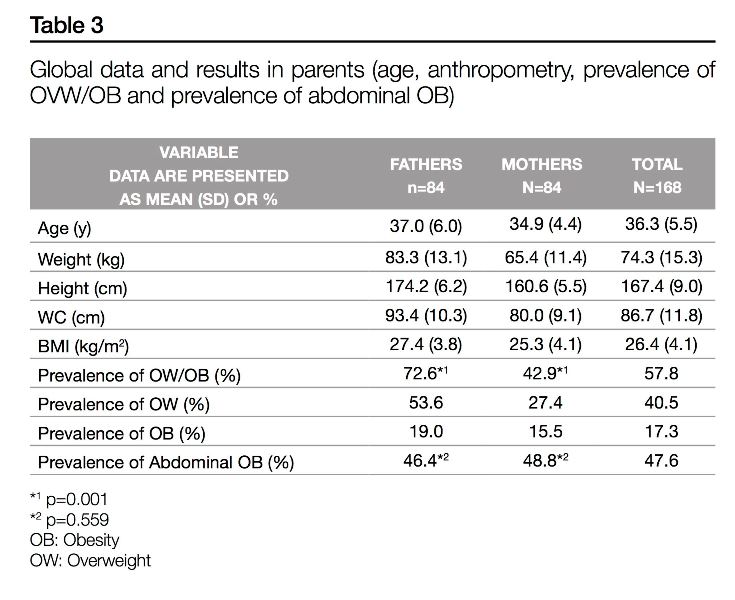
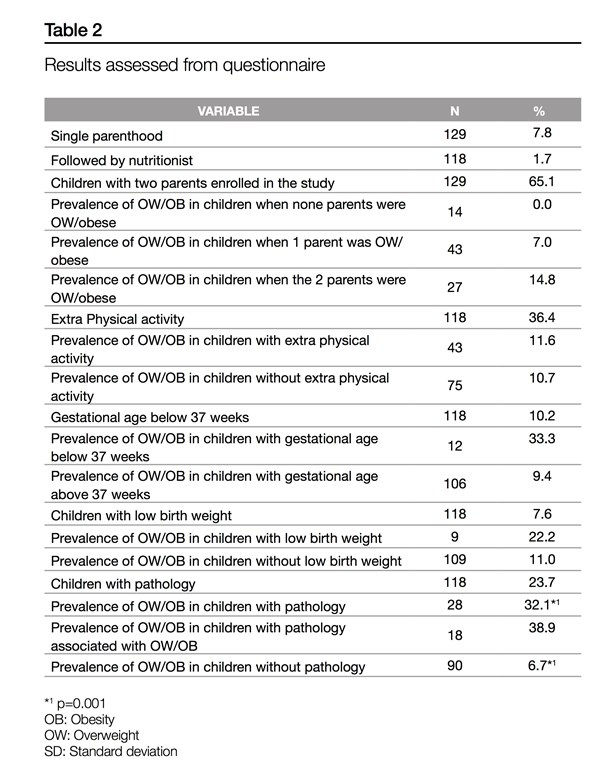
In children, global prevalence of OW and OB was 11.7%, (7.8% of OW and 3.9% of OB) without statistical differences between genders (p=0.584) (Figure 1). The age group of 5 years contributed the most (6.2%) to total prevalence of OW and OB, with 4.65% in girls and 1.55% in boys. OB was not identified in children aged 2 to 3 years (Figure 1). There was a significantly higher prevalence of OW and OB in children with any disease diagnosis comparing to those referred to be healthy (32.1% vs. 6.7%) (p=0.001) Table 3. Enrolment of both parents was only possible in 84 children (65.1%). When none, one or both parents were OW or obese, the prevalence of OW and OB in children was 0.0%, 7.0% and 14.8%, respectively (Table 2). In parents, the overall prevalence of OW and OB was 57.8% (40.5% of OW and 17.3% of OB), higher in fathers (72.6%) than in mothers (42.9%) (p=0.001) (Table 3). The global prevalence of abdominal OB in progenitors was 47.6%, with similar rates in both genders (p=0.559) (Table 3).
DISCUSSION
The main result of this study is that OW and OB prevalence in children was lower than expected. Parental OW/OB was comparable to general adult Portuguese population. When both progenitors had OW or OB, prevalence of OW and OB in children doubled, comparing with children’s prevalence when only one progenitor had OW/OB. Some factors like low birth weight and prematurity are recognized as important modulators of OW and OB (17). However, the sample size does not allow us to take firm conclusions. Considering the diagnosis of any disease, prevalence of OW and OB was 32.1% in this sub-group of children, compared with 6.7% in healthy children. Although in general some diseases are clearly associated with OW and OB, others may not. In this particularly case, we cannot exclude the possibility of a higher parental protection, ultimately limiting more intense physical exercise in these children. Studies have shown an inverse relation between physical activity and OW and OB (18). However, in our study the prevalence of OW and OB in children who practiced extra organized physical activity out of CASM (11.6%) was similar compared to the prevalence of those practicing exclusively in CASM (10.6%). In contrast, it has been stated that parental OW and OB is a risk factor for its occurrence in children (19, 20) and our study confirmed the same trend. When both parents had a normal BMI, the prevalence of OW and OB in their children was null. However, the prevalence of OW and OB in children increased from 7.0% to 14.8% when one or both parents had OW or OB, respectively. This is similar to what is described in the literature showing the influence of obesogenic environment in OW/OB in children (9). Furthermore, prevalence of OW and OB in parents seemed to follow the trend of general Portuguese population 57.8% vs. 51.4% (21, 22). Regarding abdominal OB, parents in our study seemed to have a higher prevalence then Portuguese population (47.6% and 29.6% respectively) (21, 22). Taking that adult OW and OB rates in our study follow the adult Portuguese trends and abdominal OB seems even higher, we here speculate whether a higher prevalence of OW and OB in children could be found. The majority of children were admitted in CASM before 1 year of age, in a stage of food diversification and acquisition of food habits. Our results support the hypothesis whether this relatively low prevalence of OW and OB in children may be reflecting the beneficial impact of food and physical activity habits implemented in CASM, as previously suggested (23). Intervention programs towards OW prevention in children should start as soon as possible and parents should be part of this process (24). At CASM, the food patterns are carefully adjusted since weaning age in order to prevent OW and OB. Again, the focus at the preschool age is crucial considering the higher remission rates at this age comparing to primary school age (25). From our knowledge, limited studies analyzed the prevalence of OW/OB in preschool age and particularly in Portugal there are no reports using the WHO criteria (26). Analyzing the prevalence of OW and OB in other countries, our study showed a lower prevalence compared to a Greek study that showed a total prevalence of 32.6% in the same age group (2-6 years) (27). This result is according to the literature that already classified the southern Europe as a region of particularly high prevalence of OW and OB in pediatrics (2). Comparing WHO definition with other criteria, usually the former identifies the highest prevalence of OW and OB (28, 29). Even though, in comparison to other Portuguese studies, our results seem optimist (26). This study has several limitations like a little sample size and a cross-sectional design that does not allow us to establish a correlation between the nutritional and physical activity pattern established and the low prevalence of OW and OB found.
CONCLUSIONS
Our study found a relatively low prevalence of OW and OB in children from CASM (11.7%) comparing to similar studies. Moreover, parents manifested a similar OW and OB prevalence compared to the Portuguese adult population, so we would expect to find a higher prevalence of this condition in children. In that way, longitudinal studies are needed to clearly demonstrate the benefits of both nutritionist supervision and free access to physical exercise programs on the prevention/reduction of OW and OB in kindergartens like CASM.
ACKNOWLEDGMENTS
We would like to thank Ana Fontes, Ana Neiva, Arminda Oliveira, Carla Dias, Carla Rodrigues, Célia Alvim, Clara Santos, Cláudia Costa, Cristina Ferradaz, Elsa Sá, Fátima Baptista, Margarida Serralva, Maria José Coelho, Mariana Oliveira, Mónica Silva, Paula Alves, Paula Matos, Paula Oliveira, Rosa Oliveira, Sónia Tavares and Vânia Dias for their assistance in data collection.
We also thank all the children and parents that participated in this study.
REFERENCES
1. Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. International journal of pediatric obesity : IJPO : an official journal of the International Association for the Study of Obesity. 2006;1(1):11-25. [ Links ]
2. Cattaneo A, Monasta L, Stamatakis E, broret S, Castetbon K, Frenken F, et al. Overweight and obesity in infants and pre-school children in the European Union: a review of existing data. Obesity reviews : an official journal of the International Association for the Study of Obesity. 2010;11(5):389-98. [ Links ]
3. Monasta L, Batty GD, Cattaneo A, Lutje V, Ronfani L, Van Lenthe FJ, et al. Early-brfe determinants of overweight and obesity: a review of systematic reviews. Obesity Reviews. 2010;11(10):695-708. [ Links ]
4. Deckelbaum RJ, Williams CL. Childhood obesity: the health issue. Obesity research. 2001;9 Suppl 4:239s-43s. [ Links ]
5. Singh AS, Mulder C, Twisk JW, van Mechelen W, Chinapaw MJ. Tracking of childhood overweight into adulthood: a systematic review of the literature. Obesity reviews : an official journal of the International Association for the Study of Obesity. 2008;9(5):474-88. [ Links ]
6. Crocker MK, Yanovski JA. Pediatric Obesity: Etiology and Treatment. Endocrinology and metabolism clinics of North America. 2009;38(3):525-48. [ Links ]
7. Gurnani M, Birken C, Hamilton J. Childhood Obesity: Causes, Consequences, and Management. Pediatric Clinics of North America. 2015;62(4):821-40. [ Links ]
8. Agras WS, Hammer LD, McNicholas F, Kraemer HC. Risk factors for childhood overweight: A prospective study from birth to 9.5 years. The Journal of Pediatrics. 2004;145(1):20-5. [ Links ]
9. Lake A, Townshend T. Obesogenic environments: exploring the built and food environments. The Journal of the Royal Society for the Promotion of Health. 2006;126(6):262-7. [ Links ]
10. Reilly JJ. Physical activity, sedentary behaviour and energy balance in the preschool child: opportunities for early obesity prevention. Proceedings of the Nutrition Society. 2008;67(03):317-25. [ Links ]
11. Dietz WH. Critical periods in childhood for the development of obesity. The American Journal of Clinical Nutrition. 1994;59(5):955-9. [ Links ]
12. Wijnhoven TMA, van Raaij JMA, Sjöberg A, Eldin N, Yngve A, Kunešová M, et al. WHO European Childhood Obesity Surveillance Initiative: School Nutrition Environment and Body Mass Index in Primary Schools. International Journal of Environmental Research and Public Health. 2014;11(11):11261-85.
13. WHO Child Growth Standards based on length/height, weight and age. Acta paediatrica (Oslo, Norway : 1992) Supplement. 2006;450:76-85. [ Links ]
14. de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bulletin of the World Health Organization. 2007;85(9):660-7. [ Links ]
15. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organization technical report series. 1995;854:1-452. [ Links ]
16. Alberti KGMM, Zimmet P, Shaw J. Metabolic syndrome—a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabetic Medicine. 2006;23(5):469-80.
17. Zarrati M, Shidfar F, Razmpoosh E, Nezhad FN, Keivani H, Hemami MR, et al. Does Low Birth Weight Predict Hypertension and Obesity in Schoolchildren? Annals of Nutrition and Metabolism. 2013;63(1-2):69-76. [ Links ]
18. Moore LL, Gao D, Bradlee ML, Cupples LA, Sundarajan-Ramamurti A, Proctor MH, et al. Does early physical activity predict body fat change throughout childhood? Preventive Medicine. 2003;37(1):10-7. [ Links ]
19. Reilly JJ, Armstrong J, Dorosty AR, Emmett PM, Ness A, Rogers I, et al. Early life risk factors for obesity in childhood: cohort study. BMJ (Clinical research ed). 2005;330(7504):1357. [ Links ]
20. Magarey AM, Daniels LA, Boulton TJ, Cockington RA. Predicting obesity in early adulthood from childhood and parental obesity. International journal of obesity and related metabolic disorders : journal of the International Association for the Study of Obesity. 2003;27(4):505-13. [ Links ]
21. Poínhos R CF, Durão C, Franchini B, Rodrigues S, Afonso C, Moreira P, Teixeira VH, Pinho O, Silva D, Lima Reis JP, Veríssimo MT, de Almeida MDV. Determinants of weight and health status perception among portuguese adults. Alimentação Humana. 2011;17(1/2/3):7-14. [ Links ]
22. Poínhos R FB, Afonso C, Correia F, Teixeira VH, Moreira P, Durão C, Pinho O, Silva D, Lima Reis JP, Veríssimo T, de Almeida MDV. Alimentação e estilos de vida da população portuguesa: metodologia e resultados preliminares. Alimentação Humana. 2009;15(3):43-60. [ Links ]
23. De Kroon MLA, Renders CM, Van Wouwe JP, Van Buuren S, Hirasing RA. The Terneuzen Birth Cohort: BMI Changes between 2 and 6 Years Correlate Strongest with Adult Overweight. PLoS ONE. 2010;5(2):e9155. [ Links ]
24. Griffiths LJ, Hawkins SS, Cole TJ, Dezateux C. Risk factors for rapid weight gain in preschool children: findings from a UK-wide prospective study. Int J Obes. 2010;34(4):624-32. [ Links ]
25. von Kries R, Beyerlein A, Muller MJ, Heinrich J, Landsberg B, Bolte G, et al. Different age-specific incidence and remission rates in pre-school and primary school suggest need for targeted obesity prevention in childhood. Int J Obes. 2012;36(4):505-10. [ Links ]
26. Antunes A, Moreira P. [Prevalence of overweight and obesity in Portuguese children and adolescents]. Acta medica portuguesa. 2011;24(2):279-84. [ Links ]
27. Hassapidou M, Daskalou E, Tsofliou F, Tziomalos K, Paschaleri A, Pagkalos I, et al. Prevalence of overweight and obesity in preschool children in Thessaloniki, Greece. Hormones (Athens). 2015; 14(4):615-22. [ Links ]
28. Maalouf-Manasseh Z, Metallinos-Katsaras E, Dewey KG. Obesity in preschool children is more prevalent and identified at a younger age when WHO growth charts are used compared with CDC charts. The Journal of nutrition. 2011;141(6):1154-8. [ Links ]
29. Kovalskys I, Rausch Herscovici C, De Gregorio MJ. Nutritional status of school-aged children of Buenos Aires, Argentina: data using three references. Journal of public health (Oxford, England). 2011;33(3):403-11. [ Links ]
Endereço para correspondência
Júlio C Rocha
Centro de Genética Médica,
Centro Hospitalar do Porto,
Praça Pedro Nunes, n.º 88,
4099-028 Porto, Portugal
julio.rocha@chporto.min-saude.pt
Recebido a 29 de agosto de 2016
Aceite a 12 de dezembro de 2016


{kind=link}
{kind=link}
{kind=link}
{kind=link}