










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Portuguesa de Nutrição
versão On-line ISSN 2183-5985
Acta Port Nutr no.13 Porto jun. 2018
https://doi.org/10.21011/apn.2018.1304
ARTIGO DE REVISÃO
Gestational Diabetes and Microbiota: role of probiotic intervention
Diabetes Gestacional e o Microbiota: o Papel da Intervenção com Probióticos
Juliana Morais1-3; Manuela Cardoso4; Jorge Branco5; Cláudia Marques1,3; Diana Teixeira1-3; Ana Faria1-3; Conceição Calhau1,3*
1 Nutrição e Metabolismo, NOVA Medical School | Faculdade de Ciências Médicas da Universidade Nova de Lisboa, Campo Mártires da Pátria, n.º 130, 1169-056 Lisboa, Portugal
2 Comprehensive Health Research Center, NOVA Medical School | Faculdade de Ciências Médicas da Universidade Nova de Lisboa, Campo Mártires da Pátria, n.º 130, 1169-056 Lisboa, Portugal
3 CINTESIS, Center for Health Technology and Services Research, Rua Dr. Plácido da Costa, 4200-450 Porto, Portugal
4 Unidade de Nutrição e Dietética da Maternidade Dr. Alfredo da Costa, Rua Viriato, n.º 1, 1050-010 Lisboa, Portugal
5 Obstetrícia e Ginecologia, NOVA Medical School | Faculdade de Ciências Médicas da Universidade Nova de Lisboa, Campo Mártires da Pátria, n.º 130, 1169-056 Lisboa, Portugal
Endereço para correspondência
ABSTRACT
The number of women with Gestational Diabetes is increasing over the years. The microbiota has been related to energy regulation, immune function and metabolic disorders, such as insulin resistance. It is essential to understand the changes in the gut, placental and vaginal microbiota during pregnancy and the impact this may have on mother and fetus health. Supplementation with probiotics appears to be an effective strategy in the prevention and treatment of Gestational Diabetes and weight gain. Studies shown that probiotic intake improves maternal glucose tolerance and insulin sensitivity. This review intends to shed some light on the influence of gut, placental and vaginal microbiota on Gestational Diabetes and the role of probiotics intervention.
KEYWORDS
Gestational Diabetes, Microbiota, Pregnancy, Probiotics
RESUMO
O número de mulheres com Diabetes Gestacional tem vindo a aumentar. A microbiota tem sido associada à regulação energética, função imunológica e doença metabólica, como a resistência à insulina. É essencial compreender quais as mudanças que ocorrem no microbioma do intestino, da placenta e da vagina durante a gravidez e qual o impacto que essas mudanças podem ter sobre a saúde da mãe e do feto. A suplementação com probióticos parece ser uma terapia eficaz na prevenção e tratamento da Diabetes Gestacional e do ganho de peso. Estudos demonstram que a ingestão de alimentos ricos em probióticos melhora a tolerância à glicose e a sensibilidade à insulina das grávidas. Esta revisão apresenta evidência sobre a influência que a microbiota intestinal, placentária e vaginal têm sobre a Diabetes Gestacional e qual o papel da intervenção com probióticos.
PALAVRAS-CHAVE
Diabetes Gestacional, Microbiota, Gravidez, Probióticos
INTRODUCTION
In the gestational period, substantial hormonal, immunological and metabolic changes are observed such as increased absorption of nutrients and increased insulin concentration accompanied by insulin resistance. This metabolic adaptation is essential to promote fetal growth, nevertheless, during the second half of pregnancy, this is potentially a diabetogenic condition (1). Moreover, in some pregnant women these processes are overstated, leading to Gestational Diabetes (GD). GD corresponds to any degree of glucose metabolism anomaly documented, for the first time, during pregnancy (2). The prevalence of GD has rapidly increased in recent years. In 2016, the prevalence in Portugal was 7.5%, increased markedly in women over the age of 40 years and differed by region (2).
Increased maternal glucose levels may result in complications for the newborn, birth trauma and neonatal hypoglycemia (3). Women with a history of GD presents an increased risk of developing type 2 diabetes in later in life. GD is also associated with an increased risk of chronic diseases such as obesity (4), metabolic syndrome, non-alcoholic fatty liver disease (5, 6), glucose metabolism disorders and autism (7) during childhood and adulthood of offspring. The mechanism by which maternal GD portends offspring risk for chronic diseases is not well understood, but it is believed that the effects may be mediated through alterations in the maternal microbiome during pregnancy that are shared with the newborn either during gestation, delivery, or subsequently (8).
Microbiota is determined by many factors such as mode of delivery, feeding type, nutrition, genetics, health status, gestational age, and antibiotics use (4). Initially, these microorganisms were thought to be transmitted between mother and child after birth. In other words, the intrauterine environment during pregnancy has been presumed to be sterile, although recent evidence suggests the presence of bacteria in amniotic fluid, umbilical cord blood, placental and fetal membranes and meconium (4, 9). It is only at 3 years that adult-like composition is established (10), but the primordial transmission of bacteria between mother and child occurs in utero, during delivery and during lactation; thus the occurrence of dysbiosis during this period caused by GD may be a risk factor for the infant (6).
There are several studies that demonstrate the benefits of using probiotics in the prevention of gestational diabetes and also in the control of weight gain throughout pregnancy (11–14). Prenatal maternal probiotic supplementation may provide a novel early tool to combat the major health challenges such as obesity and immune-inflammatory disease faced by the newborn today.
In this review we consider the changes that occur in the maternal gut, placental and vaginal microbiota in a gestational diabetes situation, and the role of probiotics as a key tool in the treatment.
Diabetes in pregnancy and microbiota
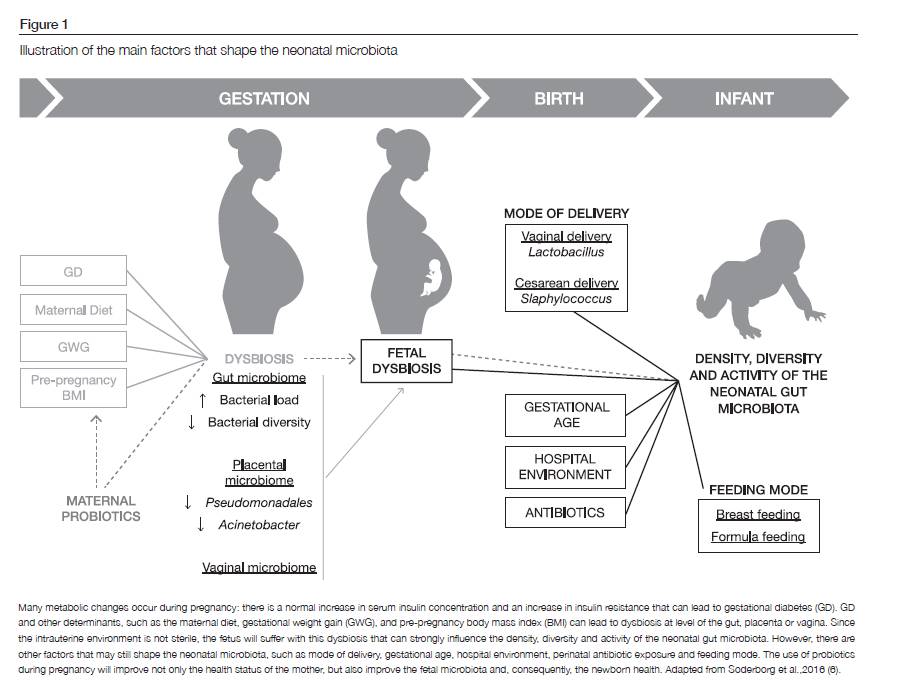
Until now, there is no research that examined directly the association of GD with maternal microbiota during pregnancy. However, it is known that changes in gut, placental and vaginal microbiota occurs over the course of pregnancy (Figure 1). As well as microbiota profiles change, the metabolic hormone levels also change and these changes are correlated (15). Fetus born of an obese mother had higher percentage of body fat and developed insulin resistance already in utero (16). Other study showed that mother’s weight had an effect on infant microbiota development (17), which suggests that the microbiota of mothers is an important factor for baby health.
Gut microbiota
In the gut inhabits the largest microbiota at the human body. The colonization of commensal bacteria is essential to the biosynthesis of vitamins, release of gut hormones, maintenance of the gut barrier function (17), regulation of the immune system (8) and lipid metabolism (18) and control the energy extraction of non-digestible polysaccharides for the production of short chain fatty acids (SCFA), such as acetate, butyrate and propionate (19, 20). Gut microbiota also regulates the intercellular thigh junctions in the intestinal mucosa, in order to inhibit the absorption of endotoxins, like lipopolysaccharide (LPS), which have been positively correlated with obesity, inflammatory markers and abnormal glycemic levels (21). As well as circulating zonulin, a protein that influences intestinal barrier function, whose concentration is influenced by SCFA production, that is determined by gut microbiota composition, even as dietary intake of n-3 polyunsaturated fatty acids (PUFAs), fiber, and certain vitamins and minerals (22).
A b influence between the gut microbiota composition and the pregnancy metabolism has been recently described (15). In fact, over the course of gestation profound changes have been shown (1): bacterial load increase in the gut (1, 23), the relative amount of lactic-acid producing bacteria increases (15) and bacterial diversity decrease with obesity and insulin resistance (24). A systematic review found that the maternal gut microbiota was associated with pre-pregnancy body mass index (BMI), gestational weight gain and GD (8). Insulin, c-peptide, insulin resistance index and fasting glucose were all significantly and positively correlated with increasing BMI and with specific bacteria. Collinsella (family Coriobacteriaceae, phylum Actinobacteria) showed a positive correlation between insulin and pregnancy, as well as maternal triglycerides and VLDL cholesterol. In contrast, Collinsella exhibit a trend for negative correlation with maternal HDL cholesterol. In this study, authors concluded that manipulating the abudance of Collinsella may affect both glucose and lipid metabolism in pregnancy (15). Further, a group of investigators observed a major number of Proteobacteria and Actinobacteria between first to third trimester (1). Then, they inoculated germ free mice with stool collected in the first vs. third trimester. The mice that received the third trimester microbiota gained more weight, become more insulin resistant and had higher levels of inflammatory markers (1). This data confirm the metabolic impact of the gut microbiota. However, other studies found no significant changes in the gut microbiota over the gestational period (25, 26). This divergent results may be attributable to differences in the frequency of sampling and in the methodology used, as well as the population of study. Addictionally, it was found that, regardless of their age, the children’s microbiota were most similar to their mothers’ microbiota in the first trimester (1). Accordingly, presupposing that the infant microbiota is related to the maternal gut microbiota, care should be taken not only during pregnancy but also even before conception. Lastly, significant differences were observed in microbiota composition according to weight status before pregnancy (23). In fact, Bacteroides and S. aureus numbers appear to be significantly higher in overweight and obese pregnant women. These microorganisms may predispose to the enhanced energy storage and the decreased control of systemic low-grade inflammation typical of obesity, such as insulin resistance (23).
Placental microbiota
Since the placenta is a maternal-fetal structure that develops to allow the absorption of nutrients and oxygen uptake to the fetus, its integrity and function are fundamental for fetus development, growth and survival (27). It should be added that placenta is more than an unsterile organ; it has its own microbiota. Taking this into account, a study revealed that term infants of women with GD presented a 7.57 fold increased risk of developing atopic dermatitis and 5.91 fold increased risk of allergen sensitization (28), which could be due to placental immune cell infiltration and inflammation (29). Placental microbiota is mainly formed by Proteobacteria (29), in contrast to the gut microbiota, in which Firmicutes and Bacteroidetes are the most abundant phyla (21). It was described three hypotheses to explain the colonization of the placenta microbiota: translocation of bacteria from the vagina to the placenta; dissemination of oral bacteria via bloodstream; intestinal bacteria transported to the placental via maternal dendritic cells (30). In a recent study, placental microbiota and the expression of anti-inflammatory cytokines from women with GD and from control women were analyzed (29). It was observed that numbers of Pseudomonadales and Acinetobacter genus (both from phylum Proteobacteria) are lower in women with GD. Lower relative abundance of Acinetobacter in GD are associated to more metabolic disorders and inflammatory phenotypes (29).
Vaginal microbiota
It is well known that the vaginal microbiota during pregnancy is distinct from the non-pregnant vaginal microbiota and it can change the course of gestation (31). Here, the microbiota diversity is lower than the gut, being generally dominated by lactobacilli, which produced lactic acid to maintain low vaginal pH and prevent pathogenic bacteria invasion (32). Nonetheless, not all lactobacilli are equal: Lactobacillus crispatus are associated with decrease of vaginal mucosal inflammation and protection from adverse outcomes, while Lactobacillus iners are much more dysbiosis-associated (31), which dominated in premature labor. Further, vaginal microbiota may regulate the hormone secretion, timing parturition and the microbial colonization (8). Vaginal dysbiosis - defined as a microbiota that is not dominated by lactobacilli - has been associated with HIV and other sexually transmitted infections (STIs) and maternal and neonatal infections (31).
The majority of research in pregnant women has focused on rectovaginal Streptococcus agalactiae carriage, because it has an association with pregnancy and neonatal complications (31). More studies are needed on the development of the vaginal microbiota over the gestational period.
Probiotics intervention in pregnancy: the lack of clinical evidence
Usually, GD is a disorder controlled essentially by diet, exercise, insulin treatment or metformin, being the pharmacological treatment of first choice (33). In 2015, the International Federation of Gynecology and Obstetrics affirmed that “metformin is a safe and effective therapy for GD during the second and third trimesters, although metformin crosses the placental barrier” (34). Metformin may have direct microbial effects. A recent study recruited 459 participants to study the influence of metformin on the association of type 2 diabetes and gut dysbiosis (35). In this study, it was found that participants with diabetes but without metformin had more Pretovella and less Enterococcus casseliflavus, while the participants taking this drug had a greater relative abundance of Akkermansia muciniphila – a bacteria that has been associated with weight loss, improved metabolic control and reduced adipose tissue inflammation and SCFA (35). So, metformin could reduce diabetes-associated dysbiosis in pregnancy, as well as reduce the transmission of diabetogenic bacteria to the newborn (8). However, since the number of women with GD continues to increase, it is necessary to think about alternative prevention strategies of this disorder. Thus, a new question arises: can the use of probiotics be a preventive/therapeutic alternative for women with GD?
Probiotics are live microorganisms consumed as supplements or beverage/food in adequate quantities that may confer a health benefit on the host (36). Most of probiotic products are yoghurts, fermented milks (such as kefir, buttermilk and aryan) or other fermented beverages (kombucha) available in the supermarkets (37, 38). The first study to provide evidence of improved glucose metabolism with probiotics evaluated 256 normoglycaemic pregnant women (11). These pregnant women were randomly divided into three treatment groups: dietary counselling with probiotic [Lactobacillus rhamnosus and Bifidobacterium lactis (diet/probiotic)]; dietary counselling with placebo (diet/placebo); controls (control/placebo). The authors demonstrated that blood glucose concentrations were lowest in the diet/probiotics group during pregnancy and over the 12 months’ postpartum period (11). In a subsequent study, the same authors aimed not only to assess the impact of probiotic intervention on maternal glucose metabolism, but also to determine the safety and efficacy of perinatal dietary counselling and probiotic supplementation, evaluating fetal and infant growth for 24 months of follow up (12). In this elegant study, probiotic intervention had shown to reduce the frequency of GD: 13% (diet/probiotic) vs. 36% (diet/placebo) and 34% (control); (p=0.003). Moreover this study showed that probiotic intervention can be a safe and cost-effective tool to prevent GD (12). More recently, a randomized trial with 423 pregnant women with history of atopic disease, concluded that GD prevalence was lower in the Lactobacillus rhamnosus HN001 supplemented group than placebo, particularly among olders (age ≥35 years) and those with previous gestational diabetes (13).
In addition to their preventive role, probiotics have also been indicated as a therapeutic method for the control of glucose levels in women diagnosed with GD. Thus, in 64 women with newly diagnosed GD the supplementation with probiotics (Lactobacillus acidophilus LA-5, Lactobacillus delbrueckii bulgaricus LBY-27, Bifidobacterium BB-12 and Streptococcus thermophiles STY-31) had shown a decrease in insulin resistance and weight gain in pregnant women when compared with placebo group (14). Additionally, two short-term studies (up to 8 weeks) found that probiotic supplementation decreased serum insulin levels (39, 40). Furthermore, probiotics reduced the triglycerides and VLDL levels (but not on other lipid profiles) (39) and significantly reduced inflammatory mediators (IL-6, TNF-α and high sensitive C-reactive protein) (40). On the other hand, Lindsay et al. showed that probiotic intervention had no effect on glycemic control among women with GD or impaired glucose tolerance (41). Curiously, this last study was the only that did not used Bifidobacterium spp. in their probiotics. So far, the evidence suggests probiotic supplementation as a promising therapeutic approach for the management of GD (42).
Even if it is not completely understood how probiotics modulate glucose metabolism, potential mechanisms involving SCFAs have been reported (42). Probiotics strains that increase fermentation capacity of gut microbiota generated SCFAs that can reduce appetite by slowing intestinal transit time and reduce insulin resistence, through upregulation of Peptide YY and Glucagon-like peptide-1 when SCFAs bind to G protein-coupled receptors (42). SCFAs also prevent the circulation of LPS by regulating the intestinal permeability (21, 42) and, consequently, reduce inflammatory markers, as Jafarnejad et al. (40) demonstrated.
CONCLUSIONS
Maternal nutrition during pregnancy may initiate a cascade of metabolic and immune inflammatory conditions in infant (11). Changes occur in the intestinal and vaginal microbiota during pregnancy and may generated a microbiota composition associated with metabolic diseases, leading to insulin resistance and modulation of lipid metabolism. The development of the placenta, its hormone release and its specific microbiota may lead to disruptions in the uptake of glucose by the cells, causing hyperglycemia. A recent and very well-structured review lists a number of pathological conditions associated with teratogenicity due to maternal obesity, GD and/or excessive weight gain throughout pregnancy, such as the development in later years of diabetes, non-alcoholic fatty liver disease and metabolic-syndrome (6). This mother-to-child dysbiosis becomes a vicious cycle: a mother with a high body mass index, insulin resistance or GD has a less diverse microbiota with less Bifidobacteria and more Escherichia coli and Staphylococcus, producing different SCFAs, leading to inflammation (by LPS); this disease related information is transmitted to the fetus, who will transmit to its offspring years later and so on. These data are consistent with “Barker hypothesis” that prenatal nutrition and lifestyle play a decisive role in fetal programming and may be responsible for long-lasting effects on physiological function that could be associated with the development of disease later in life (intrauterine fetal programming) (43). Adequate treatment reduces not only the maternal adverse effects but also to the fetus. Dietary counseling associated to the probiotic supplementation is a safety and cost-effective alternative. Intake of probiotics can be as simple as eating fermented milks or yoghurts available in the supermarkets. Randomized controlled clinical trials must be implemented for a evidence-based intervention.
REFERENCES
- Koren O, Goodrich JK, Cullender TC, Spor AA, Laitinen K, Backhed HK, et al. During Pregnancy. Cell. 2013;150(3):470–80.
- Catarina A, Endocrinologia M, Garcia H. Consenso “ Diabetes Gestacional ”: Atualização 2017. 2017;12(1):24–38.
- Halkjaer SI, Nilas L, Carlsen EM, Cortes D, Halldórsson TI, Olsen SF, et al. Effects of probiotics (Vivomixx®) in obese pregnant women and their newborn: study protocol for a randomized controlled trial. Trials. 2016;17(1):491.
- Hu J, Nomura Y, Bashir A, Fernandez-Hernandez H, Itzkowitz S, Pei Z, et al. Diversified microbiota of meconium is affected by maternal diabetes status. PLoS One. 2013;8(11), e78257.
- Patel S, Lawlor DA, Callaway M, Macdonald-Wallis C, Sattar N, Fraser A. Association of maternal diabetes/glycosuria and pre-pregnancy body mass index with offspring indicators of non-alcoholic fatty liver disease. BMC Pediatr. 2016;16(1):47.
- Soderborg TK, Borengasser SJ, Barbour LA, Friedman JE. Microbial transmission from mothers with obesity or diabetes to infants: an innovative opportunity to interrupt a vicious cycle. Diabetologia. 2016;59(5):895–906.
- Xiang AH, Wang X, Martinez MP, Walthall JC, Curry ES, Page K, et al. Association of Maternal Diabetes With Autism in Offspring. Jama. 2015;313(14):1425.
- Singh S, Karagas MR, Mueller NT. Charting the Maternal and Infant Microbiome: What Is the Role of Diabetes and Obesity in Pregnancy? Curr Diab Rep. 2017;17(2):11.
- Gosalbes MJ, Llop S, Vall??s Y, Moya A, Ballester F, Francino MP. Meconium microbiota types dominated by lactic acid or enteric bacteria are differentially associated with maternal eczema and respiratory problems in infants. Clin Exp Allergy. 2013;43(2):198–211.
- Contreras M, Magris M, Hidalgo G, Robert N, Kuczynski J, Caporaso JG, et al. Human gut microbiome viewed across age and geography. 2012;486(7402):222–7.
- Laitinen K, Poussa T, Isolauri E, Nutrition AMI, Intestinal Microbiota G. Probiotics and dietary counselling contribute to glucose regulation during and after pregnancy: a randomised controlled trial. Br J Nutr. 2009;101(11):1679–87.
- Luoto R, Laitinen K, Nermes M, Isolauri E. Impact of maternal probiotic-supplemented dietary counselling on pregnancy outcome and prenatal and postnatal growth: a double-blind, placebo-controlled study. Br J Nutr. 2010;103(12):1792–9.
- K. L. Wickens, C. A. Barthow, R. Murphy et al., “Early pregnancy probiotic supplementation with Lactobacillus rhamnosus HN001 may reduce the prevalence of gestational diabetes mellitus: a randomised controlled trial,” Br J of Nutr. 2017;117(6): 804–813.
- Dolatkhah N, Hajifaraji M, Abbasalizadeh F, Aghamohammadzadeh N, Mehrabi Y, Abbasi MM. Is there a value for probiotic supplements in gestational diabetes mellitus? A randomized clinical trial. J Heal Popul Nutr. 2015;33(1):1–8.
- Gomez-Arango LF, Barrett HL, McIntyre HD, Callaway LK, Morrison M, Nitert MD, et al. Connections between the gut microbiome and metabolic hormones in early pregnancy in overweight and obese women. Diabetes. 2016;65(8):2214–23.
- Catalano PM, Presley L, Minium J, Hauguel-De Mouzon. Fetuses of Obese Mothers Develop Insulin Resistance in Utero. Diabetic Care. 2009;32(6):1076-1080.
- Collado MC, Isolauri E, Laitinen K, Salminen S. Effect of mother ’s weight on infant ’s microbiota acquisition , composition , and activity during early infancy : a prospective follow-up study initiated in early pregnancy. Am J Clin Nutr. 2010;92:1023–1030.
- Gohir W, Ratcliffe EM, Sloboda DM, Sciences B. Of the bugs that shape us: maternal obesity, the gut microbiome, and long-term disease risk. Pediatr Res. 2014;77(1):196–204.
- Cani PD, Delzenne NM. The role of the gut microbiota in energy metabolism and metabolic disease. Curr Pharm Des. 2009;15(13):1546–58.
- Cani PD, Delzenne NM. Gut microflora as a target for energy and metabolic homeostasis. Curr Opin Clin Nutr Metab Care. 2007;10(6):729–34.
- Delzenne NM, Neyrinck AM, Bäckhed F, Cani PD. Targeting gut microbiota in obesity: effects of prebiotics and probiotics. Nat Rev Endocrinol. 2011;7(11):639–46.
- Mokkala K, Röytiö H, Munukka E, Pietilä S, Ekblad U, Rönnemaa T, et al. Gut Microbiota Richness and Composition and Dietary Intake of Overweight Pregnant Women Are Related to Serum Zonulin Concentration, a Marker for Intestinal Permeability. J Nutr 2016;146(9):1694–700.
- Collado MC, Isolauri E, Laitinen K, Salminen S. Distinct composition of gut microbiota during pregnancy in overweight and normal-weight women. Am J Clin Nutr. 2008;88(4):894–9.
- Fugmann M, Breier M, Rottenkolber M, Banning F, Ferrari U, Sacco V, et al. The stool microbiota of insulin resistant women with recent gestational diabetes, a high risk group for type 2 diabetes. Sci Rep . 2015;5:13212.
- DiGiulio DB, Callahan BJ, McMurdie PJ, Costello EK, Lyell DJ, Robaczewska A, et al. Temporal and spatial variation of the human microbiota during pregnancy. Proc Natl Acad Sci. 2015;112(35):11060–5.
- Bisanz JE, Enos MK, PrayGod G, Seney S, Macklaim JM, Chilton S, et al. Microbiota at multiple body sites during pregnancy in a rural tanzanian population and effects of Moringa-supplemented probiotic yogurt. Appl Environ Microbiol. 2015;81(15):4965–75.
- Akison LK, Nitert MD, Clifton VL, Moritz KM, Simmons DG. Review: Alterations in placental glycogen deposition in complicated pregnancies: Current preclinical and clinical evidence. Placenta. 2017;54:52-28.
- Kumar R, Ouyang F, Story RE, Pongracic JA, Hong X, Wang G, et al. Gestational diabetes, atopic dermatitis, and allergen sensitization in early childhood. J Allergy Clin Immunol. 2009;124(5):1–18.
- Bassols J, Serino M, Carreras-Badosa G, Burcelin R, Blasco-Baque V, Lopez-Bermejo A, et al. Gestational diabetes is associated with changes in placental microbiota and microbiome. Pediatr Res 2016;80(6):777–84.
- Pelzer E, Gomez-Arango LF, Barrett HL, Nitert MD. Review: Maternal health and the placental microbiome. Placenta. 2016;54:30-37.
- van de Wijgert JHHM, Jespers V. The global health impact of vaginal dysbiosis. Res Microbiol. 2017;168(9-10):859-864.
- Hanlon DEO, Moench TR, Cone RA. Vaginal pH and Microbicidal Lactic Acid When Lactobacilli Dominate the Microbiota. 2013;8(11):1–8.
- Meek CL. Natural selection? The evolution of diagnostic criteria for gestational diabetes. Ann Clin Biochem 2017;54(1): 33-42.
- Gray SG, McGuire T, Cohen N, Little PJ. The emerging role of Metformin in Gestational Diabetes Mellitus. Diabetes, Obes Metab. 2017;19(6):765–772.
- de la Cuesta-Zuluaga J, Mueller NT, Corrales-Agudelo V, Velásquez-Mejía EP, Carmona JA, Abad JM, et al. Metformin Is Associated With Higher Relative Abundance of Mucin-Degrading Akkermansia muciniphila and Several Short- Chain Fatty Acid – Producing Microbiota in the Gut. Diabetes Care. 2017;40(1):54-62.
- Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B, et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol . 2014;11(8):506-14.
- Barrett HL, Callaway LK, Nitert MD. Probiotics: A potential role in the prevention of gestational diabetes? Acta Diabetol. 2012;49(1):1-13.
- Baschali A, Kyriacou A, Karavasiloglou N, Matalas A. Traditional low-alcoholic and non-alcoholic fermented beverages consumed in European countries : a neglected food group Nutrition Research Reviews Nutrition Research Reviews. 2017;30(1):1-24.
- Karamali, M. Dadkhah, F. Sadrkhanlou, M. Jamilian, M. Ahmadi, S. Tajabadi-Ebrahimi, M. Jafari, P. Asemi, Z. Effects of probiotic supplementation on glycaemic control and lipid profiles in gestational diabetes: Arandomized, double-blind, placebo-controlled trial. Diabetes Metab. 2016;42(4):234–241.
- Jafarnejad S, Saremi S, Jafarnejad F, Arab A. Effects of a Multispecies Probiotic Mixture on Glycemic Control and Inflammatory Status in Women with Gestational Diabetes : A Randomized Controlled Clinical Trial.Journal of Nutrition and Metabolism. 2016;2016,5190846.
- Lindsay KL, Brennan L, Kennelly MA, Maguire OC, Smith T, Curran S, et al. Impact of probiotics in women with gestational diabetes mellitus on metabolic health : a randomized controlled trial. Am J Obstet Gynecol. 2015;212(4):496.e1-496.e11.
- Taylor BL, Woodfall GE, Sheedy KE, Riley MLO, Rainbow KA, Bramwell EL, et al. Effect of Probiotics on Metabolic Outcomes in Pregnant Women with Gestational Diabetes : A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2017;9(5):461.
- Barker D. Mothers, babies and disease in later life. BMJ Publ Gr. 1994;673–4.
Conceição Calhau
Nutrição e Metabolismo, NOVA Medical School | Faculdade de Ciências Médicas da Universidade Nova de Lisboa,
Campo Mártires da Pátria, n.º 130,
1169-056 Lisboa, Portugal
ccalhau@nms.unl.pt
Recebido a 30 de janeiro de 2018
Aceite a 18 de junho de 2018


{kind=link}