










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Portuguesa de Nutrição
versão On-line ISSN 2183-5985
Acta Port Nutr no.15 Porto dez. 2018
https://doi.org/10.21011/apn.2018.1504
ARTIGO ORIGINAL
Nutritional, health status and well-being at work: gender’s differences
Estado de saúde e bem-estar no local de trabalho: diferenças ENTRE géneros
João PM Lima1-3*; Sofia A Costa4; Ada Rocha2-4
1Escola Superior de Tecnologia da Saúde de Coimbra do Instituto Politécnico de Coimbra, Rua 5 de Outubro, 3046-854 Coimbra, Portugal
2LAQV - Requimte, Rede de Química e Tecnologia, Rua Jorge de Viterbo Ferreira, n.º 228, 4050-313 Porto, Portugal
3GreenUPorto, Centro de Investigação em Produção Agroalimentar Sustentável,Campus de Vairão, Rua da Agrária, n.º 747, 4485-646 Vairão, Portugal
4Faculdade de Ciências da Nutrição e Alimentação da Universidade do Porto, Rua Dr. Roberto Frias, 4200-465 Porto, Portugal
Endereço para correspondência
ABSTRACT
Introduction: A report from the Institute of Medicine referred that “being male or female is a determinant variable that should be considered when analyzing basic and clinical research”.
Objectives: This work aims to look at gender differences concerning food consumption, health status, chronic diseases and well-being indicators such as: energy, mood, concentration, stress, productivity in University of Porto’s workers.
Methodology: A cross sectional observational study was conducted. Data collection was developed through the application of a self-administrated questionnaire. 513 university employees were assessed, including academic and non-academic workers.
Results: A larger number of women had breakfast (97.3% vs. 91.0%; p=0.002), mid-morning (57.0% vs. 35,3%; p<0.001) and mid-afternoon snacks (66.8% vs. 41.5%; p<0.001), everyday compared with men The frequency of consumption of fruit (58.1% vs. 29.1%; p<0.001) and vegetables (46.4% vs. 32.2%; p<0.001) everyday was higher in women than men. The frequency of consumption of alcoholic beverages at the workplace was higher in men (59.9% vs. 29.2%; p<0.001 – percentages of consumption at least once a week).
Compared to men, women reported more frequently to suffer from chronic diseases and to have a worse health status, as well as a worst well-being at the workplace.
Conclusions: Women reported to have worse health status and well-being, despite the best eating habits which could be explored and treated as an occupational concern.
Keywords
Chronic diseases, Food consumption, Gender, Health status, Occupational health
RESUMO
Introdução: Um relatório do Institute of Medicine referiu que “ser homem ou mulher é uma variável determinante que deve ser considerada quando realizada investigação básica e clínica”.
Objetivos: Este trabalho tem como objetivo analisar as diferenças entre géneros quanto ao consumo de alimentos, estado de saúde, doenças crónicas e indicadores de bem-estar como: energia, humor, concentração, stress e produtividade nos trabalhadores da Universidade do Porto.
Metodologia: Foi realizado um estudo observacional de corte transversal. A recolha de dados foi desenvolvida através da aplicação de um questionário autoadministrado. Foram avaliados 513 colaboradores, incluindo docentes e não docentes.
Resultados: Um maior número de mulheres realizou o pequeno-almoço (97,3% vs. 91,0%; p = 0,002), meio da manhã (57,0% vs. 35,3%; p <0,001) e meio da tarde (66,8% vs. 41,5%; p <0,001) ), todos os dias em comparação com os homens. A frequência de consumo de frutas (58,1% vs. 29,1%; p <0,001) e hortícolas (46,4% vs. 32,2%; p <0,001) com uma periodicidade diária foi maior em mulheres do que em homens. A frequência de consumo de bebidas alcoólicas no local de trabalho foi maior em homens (59,9% vs. 29,2%; p <0,001 - percentagens de consumo relativas a pelo menos uma vez uma semana). Em comparação com os homens, as mulheres relataram mais frequentemente sofrer de doenças crónicas e ter um pior estado de saúde, bem como um pior bem-estar no local de trabalho.
Conclusões: As mulheres relataram um pior estado de saúde e bem-estar, apesar dos melhores hábitos alimentares, o que poderá ser explorado e tratado como uma preocupação ao nível da saúde ocupacional.
Palavras-chave
Doenças crónicas, Consumo alimentar, Género, Estado de saúde, Saúde ocupacional
INTRODUCTION
A sedentary lifestyle and poor eating habits are frequently associated with the onset of Noncommunicable Diseases (NCDs), such as obesity, type 2 diabetes, cardiovascular disease and some cancers (1). These conditions have been raising at younger ages, affecting the active population (2). Thus, NCDs have impact not only on health and quality of life of individuals and their families, but also on the socio-economic structure of a country (1).
A report from the Institute of Medicine noted that “being male or female is an important variable that should be considered when analyzing basic and clinical research” (3). The report also stated that “the understanding of gender differences in health and illness merits serious scientific enquiry in all aspects of biomedical and health-related research” (3).
Gender differences in behavior and cognition were also noted to play a part in differences in health (4). Observations show that the female survival advantage is a relatively modern phenomenon, that it has varied considerably over time, and that it differs between countries, pointing to the need of considering the environmental and behavioral factors in gender differences in health (5-7).
According to various authors, health and well-being may affect productivity through absenteeism and presenteeism (lack of full functioning and performance at work often due to the diminished health of workers) (8, 9). Attending that well-being at worksite seems to have a positive correlation with health status, programs to promote health of workers are justified, playing an important role on improving productivity, happiness and health (10, 11), particularly in women workforce (12).
This work aims to look at gender differences related to food consumption, health status, chronic diseases and well-being indicators such as: energy, mood, concentration, stress, productivity in University of Porto’s workers.
METHODOLOGY
The university under analysis had 3307 employees: 1750 teachers and researchers (academic), 1551 non-teaching staff (non-academic) (13).
From the total of human sources, participants were randomly selected. A cross sectional observational study was conducted.
Informed consent was obtained and the purpose of the study was individually explained after approval by the Ethics Committee of the University.
Data collection was performed during labor hours and it was obtained through the application of a self-administrated questionnaire, developed according to the aim of the study. Participants were asked to report the frequency or quantity of fresh fruit, soup, vegetables, alcoholic and water consumption at the workplace. For the analysis of the frequency of consumption, a scale of 4, 6 or 8 points was used, depending on the factor under analysis. They were also asked to classify in a scale of 5 points their health status, between very bad to very good. Levels of energy, mood, concentration, stress and productivity were reported using also a scale of 5 points, between very low and very high. Respondents were also questioned about suffering from any chronic disease and asked to identify them. After data collection, reported diseases were grouped according to the etiology. Socio-demographic questions were also included.
Normality distribution of cardinal variables was tested applying skewness and kurtosis. Only the Body Mass Index (BMI) was considered a variable with a normal distribution.
Descriptive statistical analysis was performed crossing with gender. Student’s t-test for was applied to identify statistical difference in normal variables. Mann-Whitney was used to determine statistical difference between nominal and ordinal variables and Chi Square for nominal variables. Mean and standard deviation or median and interquartile range were used to describe the variables according upon the shape of their distribution. The significance level assumed in hypothesis testing was 5% maximum. Data analysis was performed using IBM SPSS® Statistics 24.0 for Windows® (2012, SPSS Inc., Chicago, USA).
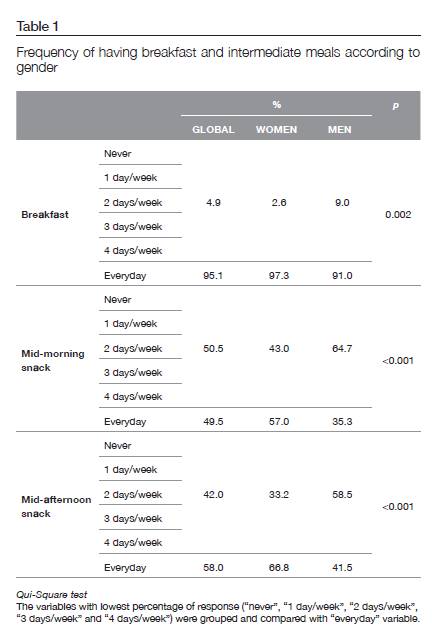
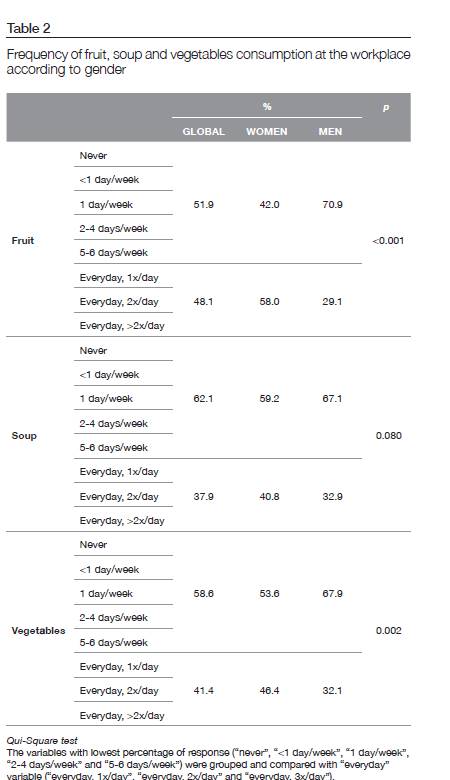
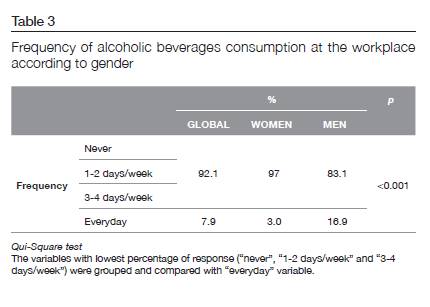
During data treatment, the variables of frequency of consumption with lowest percentage of response (in case of Table 1: “never”, “1 day/week”, “2 days/week”, “3 days/week” and “4 days/week”; in case of Table 2: “never”, “<1 day/week”, “1 day/week” , “2-4 days/week” and “5-6 days/week”; in case of Table 3: “never”, “1-2 days/week” and “3-4 days/week”) were grouped and compared with “everyday” variable (or in case of Table 2 “every day, 1x/day”, “every day, 2x/day” and “every day, 3x/day”).
RESULTS
Socio-demographic characteristics
There were assessed 513 employees, including academic and non-academic workers. The majority of them were women (N= 323; 63.0%) and married, had a university degree and developed non-academic activity.
Generally, university workers reported a sedentary lifestyle, 81.5% of them answered that they spend most of the time seated and that their work was not very physically demanding (74.5%). No differences were found between genders regarding to this topic. Additionally, 59.7% of individuals go to work by car and only 29.7% use public transports, which also contributes to a sedentary activity. Furthermore, only 48.2% of individuals reported to practice any type of physical activity. Males reported to be more active than women (59.1% vs. 42.5%; p<0.001).
Anthropometric characterization
About 46% of individuals were overweight. According student’s t-test statistical differences between gender were observed, with males presenting with a higher BMI than women (26.1 ± 3.7 vs. 24.5 ± 4.3 kg/m2; p<0.001).
Food Habits
Statistically significant differences were observed between genders regarding meals patterns with breakfast, mid-morning and mid-afternoon snacks being eaten everyday more frequently in women compared with men (97.3% vs. 91.0%; p=0.002), (57.0% vs. 35.3%; p<0.001) and (66.8% vs. 41.5%; p<0.001), respectively. These results are presented on Table 1.
Although 80% of participants considered to have a healthy diet at the workplace, only 48.2% ate fresh fruit, 37.9% ate soup and 41.5% ate vegetables at least once a day at the workplace (Table 2).
Statistically significant differences were observed between genders regarding frequency of intake of fruit, soup and vegetables, with more women consuming fruit and vegetables daily (58.0% vs 29.1%; p<0.001 and 46.4% vs 32.1%; p=0.002, respectively).
Despite this, about 30% of women reported to drink alcoholic beverages at the workplace nevertheless, its frequency was even higher in men, as shown on Table 3 (p<0.001).
No differences were found on water intake at the workplace between gender, and the average consumption was 1.1 L (±0.6 L), which was in accordance with recommendations.
Health Status and Chronic Diseases
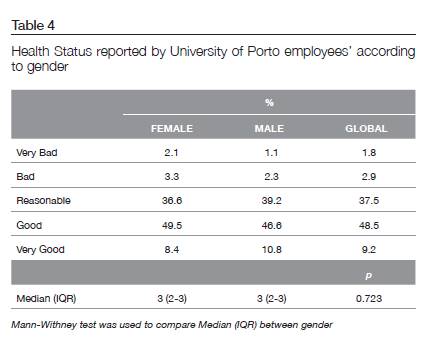
Globally, 57.7% of respondents considered their health status as “Good” or “Very Good”. A small percentage of them considered it bad or very bad. Even though results showed that more women reported a bad health status (5%), when compared to men (3%), no differences were found between gender in terms self-evaluation of health status (Table 4).
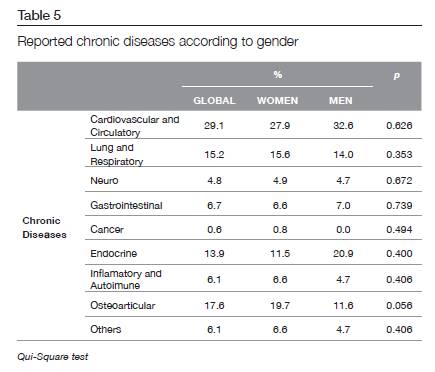
Although no significant differences were found regarding report of chronic diseases between gender (Table 5), a higher percentage of women reported to suffer from chronic disease (27.9% of women vs. 23.0% of men).
In our study absenteeism was reported to be higher in women (13.5% vs. 0%; p = 0.016) and 61.5% of women indicated that they had missed work in the previous year due to a chronic disease.
Well-being at the workplace
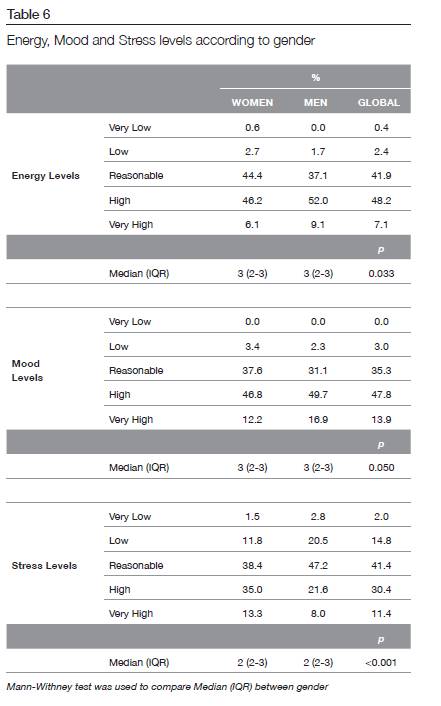
Workers of male gender reported more frequently to have higher energy (Table 6) and mood level (Table 6) than women, at the workplace. On the other hand, a higher percentage of women reported to have a great stress level (Table 6) than men.
No differences were found in terms of reported concentration and productivity between gender in our study.
DISCUSSION
Workers under analyses have a sedentary activity. Similar results were found by other authors related to physical activity of workers with similar professional activity (15, 16). This sedentary lifestyle is usually associated with a worse health status (17-19), which contributes to make these workers a risky group.
In general workers had unhealthy eating habits, considering studied variables. However, women reported to have healthier eating habits than men. This assumption is made considering as indicators of healthy eating the higher frequency of having breakfast and intermediate meals, the higher frequency of soup, fruit and vegetables consumption, the higher consumption of water and lower alcoholic beverages consumption, at the workplace. The low consumption of fruit and vegetables at the workplace may indicate that daily recommendation for these food groups (20) will be hardly achieved. The observed difference between gender in this study was explained by Courtenay that argued that healthy eating might be stereotyped as a “feminine” practice, and therefore men who are concerned about their masculinity might not choose healthier foods even if they knew that they should do this (21).
Attending to these results, the promotion of consumption of these food groups at the workplace may contribute to the achievement of nutritional recommendations, special in men. Andreyeva and Luedicke reported that an increase on consumption was accomplished by offering cash-value vouchers to purchase fruits and vegetables or increase fruit and vegetables availability and accessibility at the workplace (22, 23).
According to our results workers gender did not seem to influence their health status, which is contradictory with other authors, that indicated men as usually reporting a worse health status associated to their occupational tasks at work (24, 25). Once, at university settings, men and women play identical functions, no differences were found at this level.
The major diseases of adult life have a b behavioural element (27) meaning that studies of gender differences in health behaviours could play an important role in understanding gender difference in health and illness. A study of cardiovascular disease mortality in 24 countries found that gender differences in five risk factors explained over 40% of the gender difference in mortality (28). Many studies of health behaviours have found that men have higher rates of risky behaviours and lower rates of a range of healthy and hygienic practices than women (4). However, according to recent findings, cardiovascular diseases are more common in women than in men (29) and in Portugal, the number of deaths caused by cardiovascular diseases was higher in women in 2014 (30). We didn’t study incidence of illness, but the report of these conditions, but also in our study women reported less frequently to suffer from cardiovascular and endocrine diseases compared to men. However, this difference wasn’t statistical significantly.
Well-being is a summative concept that characterizes the quality of working lives, and it may be seen as a major determinant of productivity at the individual, enterprise, and societal levels (31-34). The key for maintaining the effective functioning of the workforce is the concept of wellbeing, which encompasses more than just one’s state of health; it is also a reflection of one’s satisfaction with work and life (35). Difference in well-being shows a great influence of gender on welfare at the workplace. This research showed a worst well-being reported by women. For this worst well-being status of women, several tasks may be considered such as the responsibilities of women at home, in addition to hours of formal work (36-38). According to several authors, women are exposed to different physical and psychological stressors at and outside work (39-41). Also in other relevant studies, stress was found to be higher in women (12, 40, 42-47).
In our study, no statistical differences were observed between genders related to health status and chronic diseases. However, men reported more frequently to have higher energy and mood levels, but stress seems to be higher in women. Nevertheless, in general, women seem to have better food habits than men. These differences seem to constitute a paradigm since, better eating habits should be associated with a better health status and well-being, but women reported to have worse health status and well-being, despite the best eating habits which could be explored and treated as an occupational concern.
This knowledge should contribute to increase attention given to female workers in terms of occupational health and to recognize gender differences in the workforce as vital in ensuring the safety and health of both men and women workers, as proposed by the International Labour Organization (ILO) (48). Regarding to our results and data reported from previous studies described (10, 49), university workers of female gender are a target group that should be monitored carefully (12).
These results could contribute to classify women workers as “vulnerable workers” with special Occupational Health and Safety (OHS) needs, as recognized by the ILO (51) and to OHS management needs to consider other factors including a gender perspective to provide a broader view of the subject, as suggested by other authors (39, 44, 52-54). Similar results were described for Kuhn et al in German population (55).
Limitations
The analysis of health status and well-being was performed from reported information that could be biased, depending on the perception of health and well-being of each individual, mainly between genders.
On the other hand, the analysis is about workplace lifestyle, which could not represent the global behavior of the day. However, having into consideration the large number of hours at the workplace, it is likely that food intake at the work contributes significantly for total food intake.
ACKNOWLEDGEMENTS
Authors acknowledge to the Faculty of Nutrition and Food Sciences for the financial support to this research.
REFERENCES
- WHO. Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation. Geneva: WHO; 2003.
- Wanjek C. Food at Work: Wokplace Solutions for malnutrition, obesity and chronic diseases. Geneva; 2005.
- Exploring the Biological Contributions to Human Health: Does Sex Matter? Washington, DC: Institute of Medicine, 2001.
- Wardle J, Haase, AM, Steptoe, A, Nillapun, M, Jonwutiwes, K, Bellisle, F. Gender Differences in Food Choice: The Contribution of Health Beliefs and Dieting. Ann Behav Med. 2004;27(2):107-16.
- Perls T. Genetic and environmental influences on exceptional longevity and the AGE nomogram. Ann N Y Acad Sci. 2002;959:1-13.
- Kirkwood T. Time of Our Lives: The Science of Human Ageing. Oxford: Oxford University Press; 1999.
- Waldron I, Johnston S. Why do women live longer than men? Part II. J Human Stress. 1976;3:19-29.
- Schultz A, Edington DW. Employee health and presenteeism: A systematic review. J Occup Rehabil. 2007;17(3):547-79.
- Bergstrom G, Bodin L, Hagberg J, Aronsson G, Josephson M. Sickness presenteeism today, sickness absenteeism tomorrow?: a prospective study on sickness presenteeism and future sickness absenteeism. J Occup Environ Med. 2009;51(6):629-38.
- Schulte P, Vainio H. Well-being at work – overview and perspective. Scand J Work Environ Health. 2010;36(5):422-9.
- Holt M, Powell S. Health and well-being in small and medium-sized enterprises (SMEs). What public health support do SMEs really need? Perspectives in Public Health. 2015;135(1):49-55.
- Celisa I, Bobadilla-Güémezb SF, Alonso-Almeidac MdM, Velasco-Balmasedad E. Women’s occupational health and safety management: An issue for corporate social responsibility. Saf Sci. 2017;91:61-70.
- Recursos humanos da Universidade do Porto 2015. Porto: Universidade do Porto - Reitoria, 2016.
- Recursos Humanos da U.Porto. Reitoria da Universidade do Porto, 2013.
- Church T, Thomas DM, Tudor-Locke C, et al. Trends over 5 decades in U.S. occupation-related physical activity and their associations with obesity. PLoS One. 2011;6(5).
- Thorp A, Dunstan D, Clark B, et al. Stand up Australia: Sedentary behaviour in workers. Australia: Baker IDI Heart and Diabetes Institute and the Cancer Prevention Research Centre at the University of Queensland, in partnership with Medibank Private, 2009.
- Dishman R, Berthoud H, Booth FW. Neurobiology of exercise. Obesity. 2006;14(3):345-56.
- WHO. Global recommendations on physical activity for health. 2010.
- Pedersen S, Cooley PD, Mainsbridge C. An e-health intervention designed to increase workday energy expenditure by reducing prolonged occupational sitting habits. Work. 2014;49(2):289-95.
- WHO. Global action plan for the prevention and control of noncommunicable diseases 2013-2020. Geneve: World Health Organization; 2013.
- Courtenay W. Engendering health: A social constructionist examination of men’s health beliefs and behaviors. Psychology of Men and Masculinity. 2000;1:4-15.
- Alinia S, et al. A workplace feasibility study of the effect of a minimal fruit intervention on fruit intake. Public Health Nutr. 2011;14(8):1382-7.
- Backman D, et al. Effect of Fresh Fruit Availability at Worksites on the Fruit and Vegetable Consumption of Low-Wage Employees. Journal of Nutrition Education and Behavior. 2011;43(4):S113-S21.
- Turkish, Statistical Institute. Household Labour Force database. Ankara: State Institute of Statistics, 2003.
- Office, for National Statistics. Labour Force Survey. London: Office for National Statistics, 2001.
- Martínez-González M, Carmen de la Fuente-Arrillaga, Cristina López-del-Burgo, Zenaida Vázquez-Ruiz, Silvia Benito and Miguel Ruiz-Canela. Low consumption of fruit and vegetables and risk of chronic disease: a review of the epidemiological evidence and temporal trends among Spanish graduates. Public Health Nutr. 2011;14(12A):2309-15.
- McGinnis J, Foege WH. Actual causes of death in the United States. J Am Med Assoc. 1993;270:2207-12.
- Jackson R, Chambless L, Higgins M, et al. Gender differences in ischemic heart disease and risk factors in 46 communities: An ecologic analysis. Cardiovascular Risk Factors. 1998;7:43-54.
- Yolande A, Bas B. van Rijn, Monique E. ten Haaf, Eric Boersma, Sanne A.E. Peters. Sex differences in cardiovascular risk factors and disease prevention. Atherosclerosis. 2015;241:211-8.
- Portugal Doenças Cérebro-Cardiovasculares em números – 2014. Direção-Geral da Saúde.
- Kuoppala J, Lamminpää A, Husman P. Work health promotion, job well-being, and sickness absences-a systematic review and meta-analysis. J Occup Environ Med. 2008;50(11):1216-27.
- Hassan E, Austin C, Claire C, Disley E, Hunt P, Marjanovic S, et al. Health and well-being at work in the United Kingdom Santa Monica (CA): Rand Corporation; 2009.
- Tompa E. The impact of health on productivity: macro and microeconomic evidence and policy implications. In: Sharpe A, St-Hilaire F, Banting K,, editor. The review of economic performance and social progress 2002: towards a social understanding of productivity. Montreal: Institute for Research on Public Policy; 2002. p. 181-202.
- Amick B, Gimeno D. Measuring work outcomes with a focus on health-related work productivity loss In: Wittink H, Carr D, editor. Evidence outcome and quality of life in pain treatment: a handbook for pain treatment professionals. Edinburgh (UK): Elsevier; 2008.
- Schulte P, Vainio H. Well-being at work – overview and perspective. Scand J Work Environ Health. 2010;36(5):422–9.
- Gjerdingen D, McGovern P, Bekker M, Lundberg U, Willemsen T. Women’s work roles and their impact on health, well-being, and career: comparisons between the United States, Sweden, and The Netherlands. Women Health. 2000;31(4):1-20.
- Lukmanji Z. Women’s workload and its impact on their health and nutritional status. Prog Food Nutr Sci. 1992;16(2):163-79.
- Verbrugge LM. Multiple Roles and Physical Health of Women and Men. J Health Soc Behav. 1983;24(1):16-30.
- Messing K. Physical exposures in work commonly done by women. Can J Appl Physiol. 2004;29(5):639-56.
- ILO. Women Workers and Gender Issues on Occupational Safety and Health. Geneva: International Labour Organization, 2010.
- Lu J. Perceived job stress of women workers in diverse manufacturing industries. Human Factors and Ergonomics in Manufacturing & Service Industries. 2005;15(3):275-91.
- Messing K, Punnett L, Bond M, Alexanderson K, Pyle J, Zahm S, Wegman D, Stock SR, Grosbois S de, et al. Be the fairest of them all: challenges and recommendations for the treatment of gender in occupational health research. Am J Ind Med. 2003;43(6):618-29.
- Ogiwara C, Tsuda H, Akiyama T, Sakai Y. Gender-related stress among Japanese working women. Transcultural Psychiatry. 2008;45(3):470-88.
- Zeytinoglu I, Seaton MB, Lillevik W, Moruz J. Working in the margins: women’s experiences of stress and occupational health problems in part-time and casual retail jobs. Women Health. 2005;41(1):87-107.
- Hart S, Warren AM. Understanding nurses’ work: exploring the links between changing work, labour relations, workload, stress, retention and recruitment. Economic and Industrial Democracy. 2015;36(2):305-29.
- EU-OSHA. New Risks and Trends in the Safety and Health of Women at Work. Luxembourg: European Agency for Safety and Health at Work Office for Official Publications of the European Communities, 2014.
- Collins J, O’Sullivan L. Psychosocial risk exposures and musculoskeletal disorders across working-age males and females. Human Factors and Ergonomics in Manufacturing & Service Industries. 2010;20(4):272-86.
- ILO. 10 Keys for Gender Sensitive OSH Practice. Guidelines for Gender Mainstreaming in Occupational Safety and Health. Geneva: International Labour Organization, 2013.
- Holmes S. Work-related stress: a brief review. The Journal of the Royal Society for the Promotion of Health. 2001;121(4):230-5.
- OGIÅSKA-BULIK N. Emotional Intelligence in the workplace: exploring its effects on occupational stress and health outcomes in human service workers. Int J Occup Med Environ Health. 2005;18(2):167-75.
- ILO. Women at Work. Geneva: International Labor Office, 2016.
- Botha D, Cronjé, F. Occupational health and safety considerations for women employed in core mining positions. SA Journal of Human Resource Management. 2015;1:12.
- Messing K. Women’s place in workplace health research priorities in Québec. Ind Relat. 2002;57(4).
- Vogel L. La salud de la mujer trabajadora en Europa. Desigualdades no reconocidas. Madrid: Instituto Sindical de Trabajo Ambiente y Salud (ISTAS), 2003.
- Kuhn M, Dudel C, Vogt T, Oksuzyan A. Trends in gender differences in health at working ages among west and east germans. SSM – Population Health. 2019; 7.
João PM Lima
Escola Superior de Tecnologia da Saúde de Coimbra do Instituto Politécnico de Coimbra,
Rua 5 de Outubro,
3046-854 Coimbra, Portugal
joao.lima@estescoimbra.pt
Recebido a 10 de julho de 2017
Aceite a 3 de dezembro de 2018


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}