











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
A 47-year-old man, obese, without medical problems, presented with a 15-day history of painful erythematous nodular lesions on the anterior side of lower limbs. He had no improvement with antibiotics and non-steroidal anti-inflammatory drugs (NSAIDs). He developed migratory and symmetric arthralgias (ankles, knees, elbows) and low-grade fever. The skin lesions progressed to the upper limbs. On physical examination, a mild swelling and tenderness in both ankles was noted, and lesions suggestive of erythema nodosum were seen (Fig. 1).

Figure 1: Multiple lesions suggestive of erythema nodosum in both upper (left) and lower limbs (right).
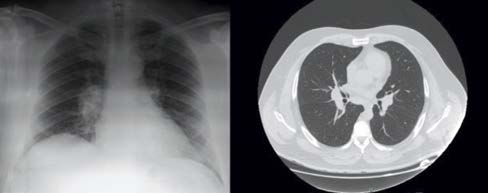
Figure 2: Bilateral para-hilar opacities on chest X-ray (left). The chest tomography (right) showing enlarged hilar and mediastinal lymph nodes.
Laboratory studies including a complete blood count, plasma levels of urea nitrogen, electrolytes, creatinine, calcium, liver enzymes, and urinalysis were normal, but a C-reactive protein (CRP) of 90.4 mg/L was detected. The chest X-ray showed bilateral para-hilar opacities and chest tomography revealed enlarged hilar and mediastinal lymph nodes (Fig. 2). Infectious causes were excluded, interferon gamma release assay test was negative and immunological study was normal, including normal level of angiotensin converting enzyme (ACE). Löfgren’s syndrome/acute sarcoidosis was assumed. Due to previous NSAIDs failure, the patient began treatment with 40 mg/day of prednisolone, with prompt resolution of the skin lesions, arthralgias and normalization of CRP. Corticosteroids were tapered to 5 mg/day without recurrent symptoms. No other organs were affected.
Sarcoidosis is a multi-systemic granulomatous disease of unknown etiology. Polyarthritis occurs in 10%-39%, particularly in the early stages of the disease.1 Löfgren’s syndrome is a particular type of acute sarcoidosis, characterized by symmetrical polyarthritis, hilar adenopathy and erythema nodosum.1,2 This triad has a 95% diagnostic specificity for sarcoidosis, and biopsy is not mandatory.3 However, it is essential to exclude other diagnoses, namely infectious causes such as tuberculosis, paraneoplastic syndromes, inflammatory bowel disease and drugs.4,5
Löfgren’s syndrome represents less than 10% of sarcoidosis cases and it is usually self-limited. Treatment involves corticosteroids in severe cases.4 High levels of ACE are associated with persistent arthritis, not observed in our patient.3

