











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkINTRODUCTION
Caring is something that compels caregivers to provide compassion, solidarity, and help, seeking the promotion of their patients’ well-being, as well as their moral integrity and dignity as a person. Care is related to the respect of the other’s desire, the acceptance of the other as they are, the acceptance of their needs, and the sharing of their anxieties (Coelho & Ferreira, 2015; Roudinesco, 2000).
The act of caring is related to social issues, gender, age, culture, and kinship ties (Hedler, Santos, Faleiros, & Almeida, 2016; Volpato & Santos, 2007). Caregivers are understood to be all persons involved in meeting patients’ needs, whether physical or psychosocial (Volpato & Santos, 2007). Often, the role of caregiver is something imposed by an unexpected situation, rather than a matter of choice (Coelho & Ferreira, 2015), as it sometimes emerges in family contexts, giving rise to informal caregivers (those who provide services without having been trained to do so). The majority of caregivers are women (Garrido & Menezes, 2004). In fact, there is a direct relationship between caregiver overload and being a female, given the variety of social roles a woman has, such as that of a mother, wife, and housewife, as well as professional work (Marins, Hansel, & Silva, 2016).
There are two types of caregiver depending on the frequency of care and the degree of involvement in care. The primary caregiver takes primary, total, or greater responsibility for the care provided, and the secondary caregiver performs activities complementary to those of the primary caregiver (Lemos, Gazzola, & Ramos, 2006). It is essential to distinguish two further types of caregivers concerning specialization. The formal caregiver is a specialized professional whose activity is performed according to a protocol and an ethical and deontological code. Family members and friends are designated as informal caregivers, where care is most often required. However, this type of care involves the expression of affection, protection, and reciprocity (Hedler et al., 2016). In this way, it is plausible to speak of the ambivalence of sensations, sometimes harmful (physical, mental, and financial overload) and sometimes positive (feelings such as companionship, empathy, love, and gratitude towards family care) (Oliveira & D’Elboux, 2012). Caregivers who experience negative situation tend to perform their functions below their capabilities. When the caregiver sees the situation positively, feeling satisfaction and pleasure in what they do, their duties are performed satisfactorily (Fratezi & Gutierrez, 2011).
Family members account for 90% of caregivers (Lemos et al., 2006). This is one of the central nuclei in the formation of the beliefs, values, and knowledge of the individual, and, in general, when an individual becomes ill, the whole family suffers and feels the consequences of the moment experienced (Inocenti, Rodrigues, & Miasso, 2009).
When patients are diagnosed, relatives often react with denial. This is followed by the search for other medical opinions, in the hope that a mistake had been made in the initial diagnosis. Denial can be accompanied by feelings of anger, revolt, and resentment. Over time, the patient and the household, or most of them, eventually accept that one of them needs care (Coelho & Ferreira, 2015). This acceptance tends to be the beginning of a gradual process of social isolation.
In addition to the physical exhaustion of caregivers from engaging in the activities associated with care, there is the emotional and social impact related to the lack of time for leisure, which is sometimes associated with a feeling of guilt, as well as a fear of suffering from the same illness or problem as the person cared for. In most cases, the financial difficulties arising from the abandonment of work activities are added (Oliveira, Carvalho, Stella, Higa, & D’Elboux, 2011). Thus, assuming the role of the caregiver within the family can be so demanding and exhausting that the mental health of the caregiver may be affected and, consequently, lead to limitation of the capacity to continue providing care (Inocenti et al., 2009).
For caregivers, formal or informal, working with patients involves unpredictability and complexity linked to pain, suffering, impotence, anguish, fear, hopelessness, helplessness, and mortality. In providing care for the patients, Caregivers promote their physical, psychological, and social well-being. Also, it is crucial to adopt a posture that goes beyond their technical skills, such as helping the patient to overcome their suffering (Machado & Merlo, 2008).
The formal caregiver follows the patients’ trajectory while they are hospitalized, and this can provide them with pleasure and/or suffering. This type of relationship between the caregiver and the person cared for can become intimate in a short time, even without having had any previous relationship before care. In the process of accomplishing the technical tasks and the emotional investment required for the patient’s improvement, conditions are created in which the caregiver may suffer from the patient’s pain or death. Moreover, the professionals’ suffering is also related to the fact that they cannot express their own feelings, which can lead to a mental imbalance that can contribute, over time, to the caregivers themselves becoming ill (Machado & Merlo, 2008).
The intensity of the suffering changes according to the culture, the values, and the emotional and social environment, as well the feelings of belonging, the ideas, and the choices of the subject. In this way, expectations of family or professional caregivers are reflective of this singularity and complexity. Accompanying a human being who is suffering or dying is one of the biggest challenges the caregiver can face. It is a process characterized by crises of fear and insecurity. There is no right way to follow these patients because the death of each is as unique as their living. Caring for someone sick, dependent, or dying requires not only physical and emotional effort, but also the sharing of tasks, decisions, and psychically complex commitments (Coelho & Ferreira, 2015).
The caregiver seeks to alleviate physical suffering, as well as meeting the psychosocial and spiritual needs of the sick person. They aim to prevent discomfort and provide the best quality of life possible (Oliveira et al., 2011). Fratezi and Gutierrez (2011) point out the importance of caregivers taking care of themselves so that they can dedicate themselves to their patient in a dignified way. Caregivers, like the patient, need to be heard regarding their anguish, fears, anxieties, and feelings. Thus, the quality of life of the caregiver is paramount for the quality of life of the patient (Verdullas, Ferreira, & Nogueira, 2011).
Coelho and Ferreira (2015), in a qualitative study investigating the narratives of caregivers, found that the act of talking provided relief transmitted the sense of empathy and acceptance, and had a beneficial or therapeutic effect. The caregivers expressed their suffering through the reports and, at the end of the interview, stated that they felt much better. In this way, it becomes pertinent to create strategies to accommodate the suffering of the caregiver and to minimize their emotional overload through the creation of times and spaces during their work week that facilitate the exchange of experiences among the caregivers, through sharing their doubts, anguishes, and joys (Soares & Munari, 2007).
In fact, there is an extensive discussion in the literature about the quality of life and biopsychosocial implications that the task of taking care of the other entails in the caregiver. However, it is pointed out as a limitation that nothing is done to advance policies and practices that diminish the suffering and the overload of these people. Thus, studies that can support initiatives to mitigate and prevent this type of impact in the life of caregivers are of great importance.
From the literature review, one can gain insight into caregivers’ degree of suffering. It is not enough to say that caregivers are invisible and lonely heroes, because they are not always seen as fundamental or valued as caregivers, either by the family or by health services (Luzardo & Waldman, 2004). There seems to be a consensus when it comes to affirming the need to evaluate the suffering of caregivers, in particular, to raise awareness among families, health services, and employers. However, to achieve this, it is urgent to find instruments that allow you to carry out such evaluation reliably.
In the absence of validated instruments for the Portuguese language (Europe) and considering the presence of the Caregiver Grief Scale (CGS) in the literature, we have chosen to translate and validate it. The choice of this scale is also based on the fact that it presents items that directly question the pain and loss, thus allowing for evaluation of suffering, as well as validating and normalizing the experiences associated with it (Meichsner et al., 2016). This is the first instrument to effectively capture the multifaceted and well-documented nature of caregivers’ suffering (Meichsner et al., 2016).
The Caregiver Grief Scale (CGS) was designed by Meichsner et al. (2016), and effectively evaluates the avoidance of suffering. It consists of 11 items that evaluate four significant aspects of the caregiver’s suffering: emotional pain, relational loss, complete loss, and acceptance of loss. The psychological pain factor refers to the experience of suffering and other unpleasant emotions related to the loss of someone. This factor is related to the feelings that are experienced in the present. The relational loss factor refers to the losses related to the relationship and shared experiences with the person cared for when the person was still healthy. The absolute loss factor relates to the end of the relationship with the person who needs care and anticipation on the part of the caregiver of a future without that person. Finally, the acceptance of the loss factor reflects the caregiver’s acceptance of the person’s illness or problem and the grieving reaction. This acceptance includes the expression of suffering because caregivers often avoid expressing or even feeling sadness during the period when the person in need of care is alive (Meichsner et al., 2016).
It should be noted that CGS allows differentiation between subgroups of caregivers. For example, it predicts that a caregiving spouse presents a higher intensity of grief and that caregivers who live with the person cared for have higher values in SGA because they regularly witness losses in daily life, increasing the suffering experienced. It is this sensitivity to this kind of thing and to the differences between the subgroups of caregivers that make CGS a helpful tool for clinical practice, as well as being beneficial for research (Meichsner et al., 2016).
Until the onset of CGS, the only tool developed to assess caregiver pain was the Marwit - Meuser Caregiver Grief Inventory (MM-CGI). This inventory includes items that assess depression and overload but does not directly address avoidance of caregiver distress (Meichsner et al., 2016). For the construction of the original version of the CGS in Germany, a sample of n = 229 was used. The validation of this instrument for the English population is underway, however, as far as we know, no validation has previously been conducted for Portuguese. With these validations, it will be possible to validate the constructs in international terms (Meichsner et al., 2016). Thus, due to the lack of instruments that assess the suffering of caregivers in Portugal, it is relevant to validate this scale for the Portuguese population.
Given the above, the general objective of the present study is to validate the Caregiver Grief Scale (CGS) factorial structure for the Portuguese population, for formal and/or informal caregivers who provide or have already provided some type of care. The specific objective is to ascertain the psychometric properties - factorial validity, convergent validity, internal consistency, and discriminant validity - of the original version, and to assess whether they are maintained in the Portuguese sample.
METHOD
The sample consisted of 150 caregivers, of whom 72 were formal and 78 informal, with a minimum age of 19 years and a maximum age of 83 years, and with a mean age of 46.8 with a standard deviation of 12.2. Most caregivers (88.7%) are female. Regarding the literary qualifications, the high school represents 28.7%, being the most representative. More than half of the study sample took care of “Others” (52%), followed by “Mother/Father” care, with 24%, and, in addition, 60% cared for more than one person. Most said that they did not live or had not lived with the person cared for. (Table 1)
Regarding the person cared for, 59 patients were cared for by informal caregivers who cared for only one person, 27 males, and 32 females. Oncological diseases were the most representative, with 12%. The remaining patients (91) were cared for by formal or informal caregivers who cared for more than one person.
For the collection of data on formal caregivers, we requested collaboration from institutions in the northern region of the country. To overcome the difficulties in the process of constituting the sample, we used two sampling techniques: convenience and snowball.
Instruments
Participants completed a sociodemographic questionnaire, where subjects indicated their age, gender, literacy, formal or informal caregiver status, who they cared for, whether they cared for more than one person, whether they lived with the person you cared for, how long they have taken care of themselves, how long they have cared for the sick person(s), and whether they would answer the questionnaire with someone they have cared for, someone who cares for them, or both. Moreover, in the sociodemographic questionnaire, all subjects included in the informal caregiver group of only one person indicated the age of the patient (if still alive), the patient’s gender, and the disease/ problem presented. As an inclusion criterion, it was established that the caregiver should have accumulated a year or more of experience in this function.
The CGS, which consists of 11 items, evaluates four significant aspects of the caregiver’s suffering, using four different factors to assess the degree of suffering/pain of the caregiver. These are: emotional pain, relational loss, absolute loss, and acceptance of loss. The questionnaire response format is on a 5-point Likert scale (1 = totally disagree to 5 = strongly agree). The original version presents good psychometric characteristics, namely, high internal consistency (Cronbach’s α = .89) and high test-retest reliability. The correlation between the total CGS scores 6 months after the first application was .998 (p <.001). The authors, based on the reported values, present this scale as reliable for both a research context and clinical practice (Meichsner et al., 2016).
Procedure
Initially, the questionnaire was translated, taking care that the language of the items was accessible and easy to understand for anyone who answered the questionnaire. In addition, care was taken to reformulate each of the items in order to adapt to the situation of the most significant number of respondents. The translation was supervised by a specialist in psychology with a relevant background in the area in which the variables studied fit, who was also bilingual (Portuguese and English) since the original version was published in English.
Table 1: Sample characterization.
| N 150 | % 100 | |
| Gender | ||
| Male | 17 | (11.3) |
| Female | 133 | (88.7) |
| Age | 150 | (100) |
| Educational Qualifications | ||
| 1st cycle | 33 | (22%) |
| 2nd cycle | 14 | (9.3%) |
| 3rd cycle | 43 | (28.7%) |
| High school | 30 | (20%) |
| Higher education | 30 | (20%) |
| Caregivers | ||
| Formal | 72 | (48%) |
| Informal | 78 | (52%) |
| Whom do you take care of?/Whom did you take care of? | ||
| Spouse | 9 | (6%) |
| Mother/Father | 36 | (24%) |
| Son/Daughter | 1 | (.7%) |
| Relative | 26 | (17.3%) |
| Another | 78 | (52%) |
| Do you take care of more than one person? | ||
| Yes | 90 | (60%) |
| No | 60 | (40%) |
| Do you live with the one you take care of?/ or Did you live with the one you took care of? | ||
| Yes | 46 | (30.7%) |
| No | 103 | (6.7%) |
| Time of care with greater % | ||
| 24 months | 16 | (10.7%) |
| 36 months | 15 | (10%) |
| People cared by: | ||
| Formal or informal caregivers who take care or taking care of more than one person | 91 | (60.6%) |
| Informal caregivers who take care or taking care of one person People cared by an informal caregiver who takes care or taking care of one person | 59 | (39.3%) |
| Gender | ||
| Male | 27 | (18%) |
| Female | 32 | (21.3%) |
| Diseases/Trouble | ||
| Heart diseases | 13 | (8.7%) |
| Cancer diseases | 18 | (12%) |
| Neurodegenerative diseases | 11 | (7.3%) |
| Old age | 8 | (5.3%) |
| Others | 9 | (6%) |
The questionnaire was then applied to the caregivers of people with a disease/problem, who worked in different institutions in the Northern region of Portugal or provided care in a family context (non-institutionalized patients). All participants completed and signed an informed consent form, and each participating institution filled out a document agreeing to the completion of the present investigation, which simultaneously clarified the purpose of the study. Everyone was informed that participation was voluntary and that the confidentiality of the data collected was guaranteed, respecting the ethical principles governing research in psychology.
The questionnaires were completed in the presence of members of the research team. Only completed questionnaires were included in the database. Subsequently, the data collected were entered into the database for all statistical analyses.
Statistical analysis
To perform the statistical treatment of the data, we used SPSS (IBM SPSS Statistics, version 24) and AMOS (IBM SPSS AMOS, version 24). Initially, the analysis of descriptive statistics regarding the items of the dimensions, as well as the variables under analysis, was performed from the mean (M) and the standard deviation (SD). The analysis of the symmetry of the frequency distribution (univariate normality) was performed through the Skewness and Kurtosis coefficients, and the values must be between -2 and 2 to verify the normality of the data (Byrne, 2010). The degree of internal consistency of the dimensions was also calculated using the Cronbach’s alpha, to see if the instrument was reliable before the sample was collected. The following values are used as valuation criteria of Cronbach’s alpha values: values higher than .90 indicate a very good internal consistency; between .80 and .89, good; between .70 and .79, satisfactory; and below .60 as having low consistency (Marôco, 2014).
In the validation process, we used the Factorial Confirmatory Analysis (AFC) and an Exploratory Factor Analysis (AFE). Initially, an AFC was carried out to test the hypothesis that the structure proposed in the original version of the CGS was maintained for the Portuguese sample. As the factorial structure of the proposed model for the German sample was not confirmed in the sample under study, and based on the values obtained, we chose to perform an Exploratory Factor Analysis (EFA).
The AFE performed in the Portuguese sample suggested the existence of a single factor, rather than four, as initially proposed. To test the unifactorial structure, an AFC was performed again. Regarding the modification indexes, we dealt with correlations of items with values higher than 10. For the models tested, the maximum likelihood estimation method was used. In order to verify the suitability of the model to the data, the following measures of evaluation of the adjustment were used: Ratio chi-square statistics/degrees of freedom (χ2/df), Comparative fit index (CFI), Goodness of fit index (GFI), the root mean square error of approximation (RMSEA), and Akaike information criterion (AIC), and decision criteria . The χ2 /df (< 5, preferably below 2) is used as the index of fit of the model, the CFI (> .90) measures the suitability of the model in relation to the independent model, the GFI (> .90) evaluates the relative amount of variance and covariance simultaneously explained by the model, the RMSEA (< .08) ascertains the discrepancy in the adjustment between the estimated and observable matrices, and the AIC (the lowest score tends to identofy the best model) is used to compare models (Marôco, 2014; Raykov & Marcoulides, 2006). Finally, to determine which type of caregiver presented the highest degree of suffering, we used the t-test, using SPSS.
RESULTS
Table 2 presents the initial descriptive analysis performed on all items of the questionnaire, which was used to verify the normal distribution of the dependent variables through the values of asymmetry and flatness, as well as of internal consistency that, in this scale, was α = .943.
In the present study, and as can be seen in Table 3, the criteria for normality of asymmetry vary between - .684 and .446, while those of skewness vary between -1.088 and -.414.Therefore, it is verified that the asymmetry and flatness values are acceptable, since, according to Marôco (2014), these values must be between -2 and 2 to verify the normality of the data. After this normality was confirmed, it was possible to perform AFC. (Table 2)
Table 2: Descriptive analyses of CGS items (model proposed by the authors).
| M± SD | Skewness | Kurtosis | |
| 1. I feel great sadness. | 3.51± 1.289 | -.511 | -.789 |
| 2. This situation is totally unacceptable to my heart. | 2.92± 1.282 | .265 | -1.084 |
| 3. It hurts to realize she/he’s gone // that she/he’s no longer what she/he was. | 3.51± 1.230 | -.428 | -.869 |
| 4. I miss many of the activities we used to share before death/illness. | 3.80± 1.123 | -.684 | -.414 |
| 5. Longing for what we had and shared in the past. | 3.26± 1.184 | -.075 | -1.071 |
| 6. I’m worried that I can not talk to her/him anymore. | 3.50± 1.191 | -.299 | -.947 |
| 7. I feel that the future has no meaning or purpose without her/him. | 2.63± 1.303 | .446 | -.932 |
| 8. I feel that life is empty without her/him. | 2.93± 1.321 | .223 | -1.088 |
| 9. I try to avoid thinking about the fact that I lost her/him // I’m going to lose her/him. | 3.48± 1.180 | -.505 | -.602 |
| 10. It is difficult for me to allow myself to suffer and to show my sadness. | 2.99± 1.156 | .056 | -.790 |
| 11. I’m having trouble accepting that she/he is suffering/suffered from this disease. | 3.03± 1.258 | -.050 | -1.068 |
| Cronbach’s alpha | .943 |
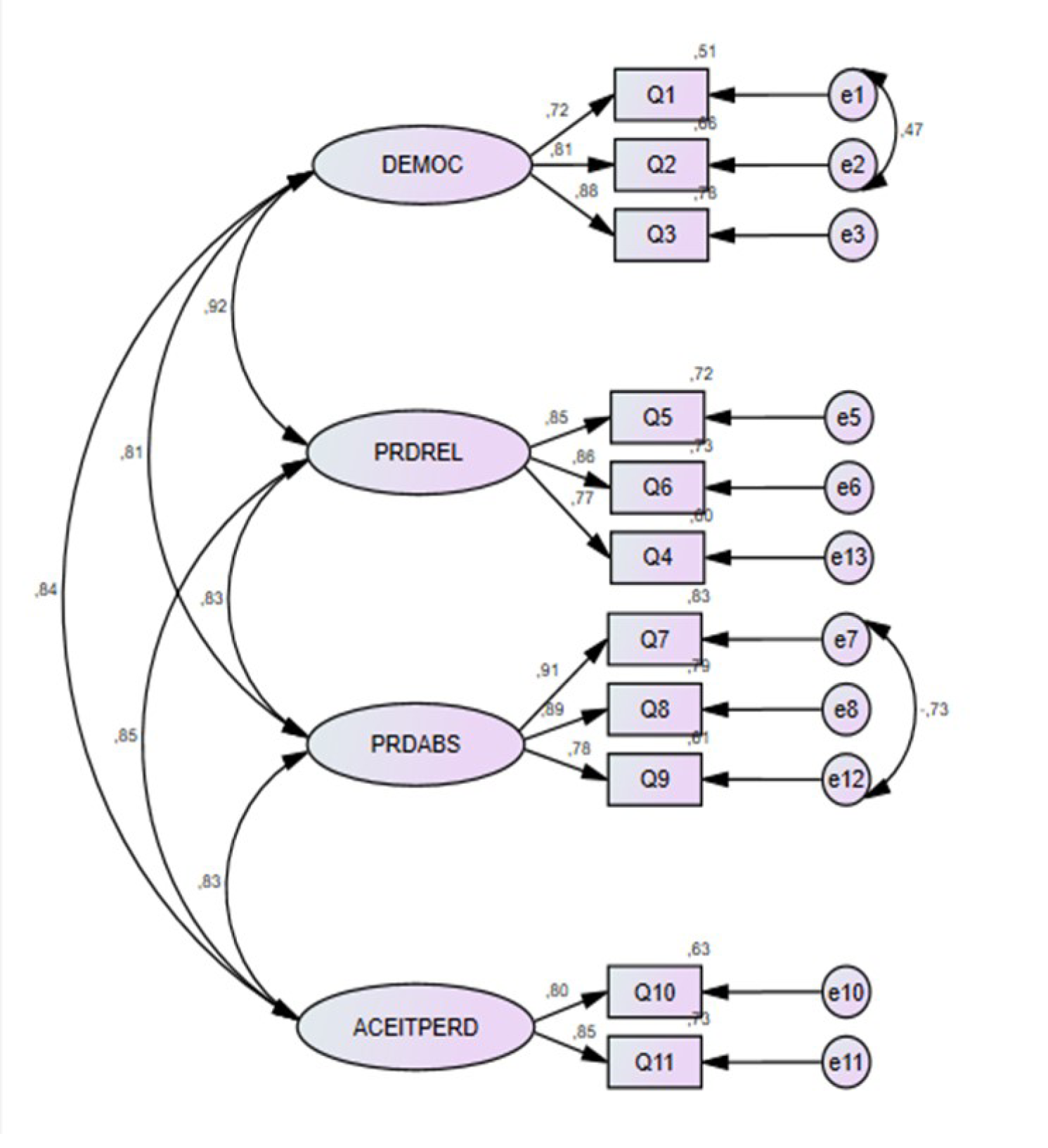
In the original validation version of the present scale, a multifactorial model was proposed with four factors: Emotional Pain, Relational Loss, Absolute Loss, and Acceptance of Loss, as shown in figure one. (Figure 1)
The model presented by the authors shows high correlations among the different subscales under analysis (r ≥ .8), which suggests that the different subscales proposed by the model are measuring a single construct. In addition to these correlation values, we found that the inadequacy of the model (χ 2 = 2.686, GFI = .893, CFI = .952, RSMEA = .106) was also evidenced. RSMEA was higher than 0.1 and, according to the criteria established in the literature, the models should be rejected whenever RSMEA is higher than .1 (Byrne, 2010; Marôco, 2014). As a complement to the decision criteria to reject the model, we use the discriminant validity calculation that evaluates whether the items that reflect a factor are correlated with other factors (Marôco, 2014), that is, whether the items of different scales actually measure different constructs. In the multifactor model, the Mean Estimated Variance (VEM) values obtained for each of the subscales were: Emotional Pain (De), .649; Relational Loss (Pr), .684; Absolute Loss (Pa), .743; and Acceptance of Loss (Ap), .680. The square of the correlations between factors were: r_ (DePr)2 = .846; R_ (DePa)2 = .656; r_ (DeAp)2 = .706; R (PrPa)2 = .688; R (PrAp)2 = .722; R (PaAp)2 = 0.688. Based on the criterion that the values of VEM must be greater than r2, we find that there is no discriminant validity between the subscales in the original version of the GSB.
The Composite Reliability (CR) calculation estimates the internal consistency of items where values should be equal to or greater than .7 (Colwell, 2016), in a range between 0 and In the multifactorial model, values obtained were: Emotional Pain, .846; Relational Loss, 0.866; Absolute Loss, .896; and Acceptance of Loss, 0.809. These values suggest that all the factors of this model have good composite reliability. However, by itself, the RC is not sufficient for the acceptance of this model.
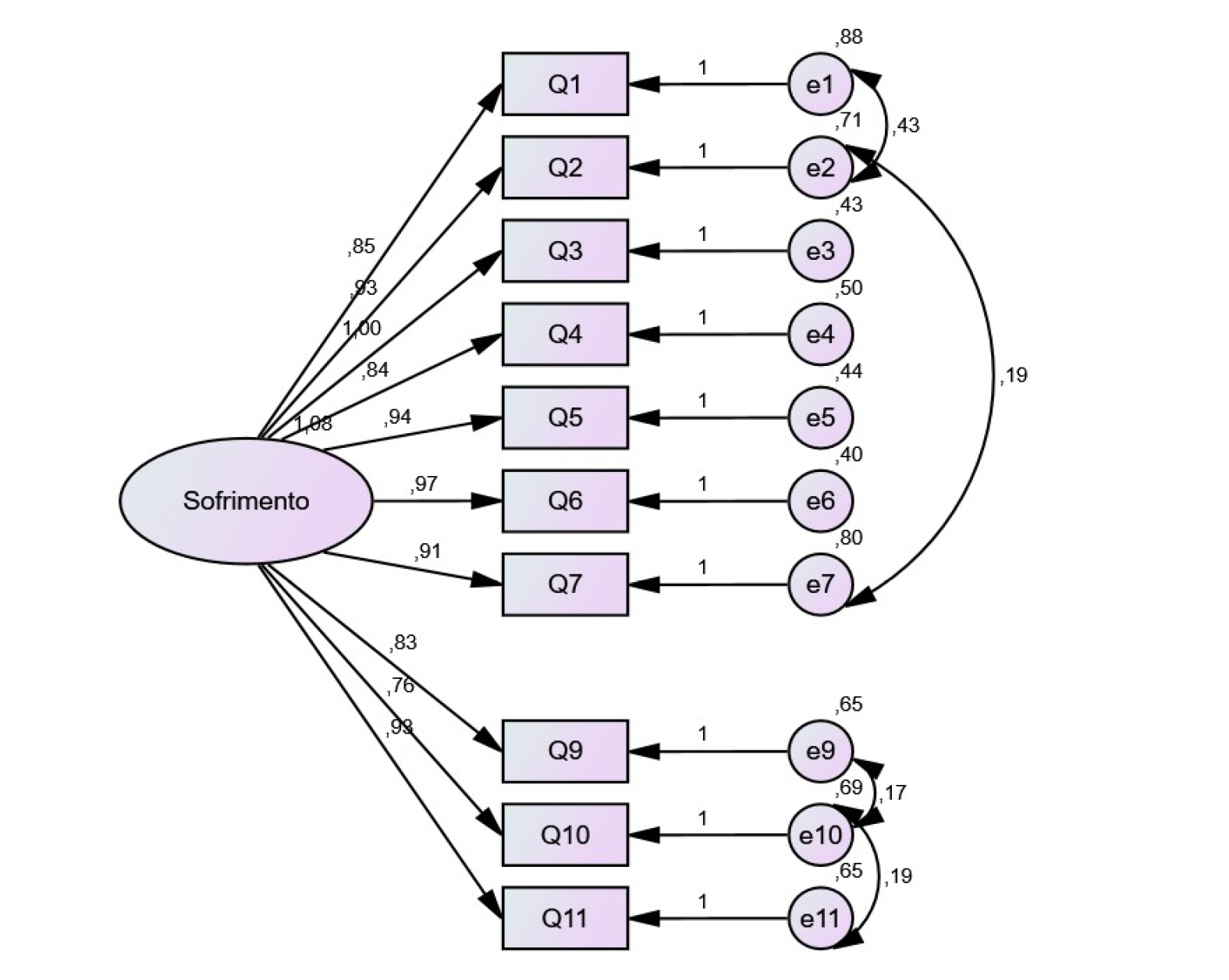
Considering the values obtained and evidencing the inadequacy of the model, we chose to perform an Exploratory Factorial Analysis (AFE), using varimax rotation. The AFE results, through the analysis of principal components, suggested a unifactorial structure, and explained 64% of the variance. This structure was later submitted to AFC, and the results were: χ2 / df (2,686) and GFI (.893); A good adjustment for the IFC (.952); and an unacceptable adjustment for the RMSEA (.106). In addition to the correction of these errors, item eight was removed, since, through the analysis of the covariance table, this showed that there were some adjustments to the single-factor model (e1-e2, e2-e7, e9-e10 and e10-e11). After the removal of item eight, it showed a good adjustment quality: χ2 / df = 2.023; GFI = .923; CFI = .970; and RMSEA = .083. In addition, it continued to present good internal consistency (α = .936). (Table 3) (Figure 2)
The value obtained from the CR for the unifactorial model was .934, which is considered as very good. As regards convergent validity, this occurs when items that are a reflection of a factor strongly saturate the same factor (Byrne, 2010; Marôco, 2014), that is, when the items that make up the factor have positive and elevated correlations between them. Thus, for there to be an adequate convergent validity, its value must be equal to or greater than .5. In the study presented, this convergent validity value is .587, thus suggesting an adequate convergent validity.
Table 3: Decision criteria to determine which model is the best fit for the study sample.
| χ2/df | GFI | CFI | RMSEA | AIC | |
| Values of the multifactor model | 2.686 | .893 | .952 | .106 | 157.356 |
| Values of the unifactor model | 5.450 | .784 | .849 | .173 | 283.818 |
| Values of the unifactor model without item 8 | 2.023 | .923 | .970 | .083 | 110.724 |
To test the predictive validity of CGS, we hypothesized: H0- “there are no statistically significant differences between the theoretically proposed model to measure the suffering of formal and informal caregivers compared with the data obtained.” The results suggest that there are differences between groups. The comparison between means shows that formal caregivers (26.8) suffer less than informal caregivers (37.9).
DISCUSSION
The act of caring implies concern, responsibility, and zeal in dealing with the patient, rather than merely a simple act of providing care, and covers all aspects of the life of the person cared for, from their suffering to their successes (Volpato & Santos, 2007).
Since the role of the caregiver is not always considered relevant, it is important to validate the CGS for the Portuguese population. Moreover, this is the only instrument to evaluate the avoidance of suffering effectively. This suffering can be manifested in different ways at different times in life (Roudinesco, 2000).
Based on the aforementioned theoretical rationale, the aim was to validate the present scale to enable evaluation of the suffering of caregivers in order to help them face difficult situations and deal with their own feelings and emotions.
The final version of the unifactorial model showed good indices of internal consistency, presenting a Cronbach alpha of .936. Although Cronbach’s alphas are very close in both the multifactor (.943) and the unifactorial model (.936), it was found that the latter had more adjusted global adjustment quality indices (χ2 / df, CFI, GFI, RMSEA, AIC). A possible explanation for such results may be because the authors who proposed the multifactor model used a sample of caregivers of elderly people with dementia, while, in contrast, in the present study, the sample consisted of caregivers of any type of person, regardless of age and disease/problem. However, this is not a reason for the multifactorial model to be rejected in future research with elderly populations with dementia. Our results show that, for samples similar to that which we used, the unifactorial model is more adequate.
To determine the construct validity, the four subcomponents must be considered: factorial validity, convergent validity, discriminant validity, and predictive validity. The instrument under study has factorial validity since the standardized factorial weights of all items are higher than 0.5, which means that the items of this instrument are the reflection of the latent factor (suffering) that is intended to be measured. The convergent validity also presented good suitability, since the existence of positive correlations between the items was verified. Regarding the predictive validity, through the t-test and through the comparison of means between the two, it was possible to verify that formal caregivers present lower degrees of suffering compared to informal ones. This corroborates the theoretical prediction that the circle of people with a greater attachment to the person in need of care suffers more than health professionals, since, in the case of the latter, the emotional bond is not so strong.
As proposed in the literature, it was verified in the present study that women assume the primary role in caring, since, in the total of the study sample, there are only 17 male caregivers, compared to 133 female caregivers. This can be explained in terms of socially established roles concerning men and women (Marins et al., 2016).
Lemos et al. (2006), mentioned that the family represents 90% of the caregivers, that is, informal caregivers. Although a more significant number of informal caregivers were found in the study sample, the difference was tenuous compared to the number of formal caregivers. Thus, it is stated that this sample is homogeneous, and it should be noted that this is due to the fact that there was a careful selection among the types of caregivers.
Caring is an act that can be demanding and exhausting to the point of affecting the mental health of all persons involved in care, limiting the ability to continue to care. Thus, it becomes essential for caregivers to take care of themselves in order not to become someone who lacks care (Fratezi & Gutierrez, 2011). In this way, it would be beneficial to create spaces and times during the work period, so that caregivers can share experiences, anguishes, and feelings, thereby feeling supported by those who are going through or have been through the same situation.
We believe, however, that the results of the present study should be analyzed in the light of some limitations. One of these concerns the fact that no pilot study was carried out to ascertain whether any changes to the questionnaire were needed in order to make it easier to understand. In addition, the sample was constituted according to a predefined characteristic (being a caregiver). Another limitation is the fact that this sample is not representative of the Portuguese population since it was limited to a region in the interior north of Portugal.
In future research, it would be advisable to extend this study to other regions of the country so that it becomes representative of the Portuguese population. It would also be important to continue to study this instrument, since there are few instruments to assess the suffering of caregivers and, also, the GSB is only validated for the German population, and validation is underway for the English population, as can be seen by literature review. Thus, we could extend this study to other Portuguese-speaking communities. Moreover, knowing that the degree of suffering varies from culture to culture, it would be interesting to understand the specificities of this construct, that is, the different perceptions of suffering among different countries, as well as between formal and informal caregivers. Do the formal and informal caregivers of different countries and cultures perceive suffering in the same way? Will the intensity of this feeling be the same? What makes this perception and intensity different? In order to answer such questions, it is of the utmost importance to continue the study of the GSB, since understanding these issues can be a starting point to help in understanding caregivers, as well as developing interventions that target them.
It might also be relevant to conduct a study with a more gender-balanced sample in the future, to evaluate the extent to which the model proposed in this study behaves equally well in both males and females.
CONCLUSION
As a response to the study objective, it is concluded that the multifactorial structure of the CGS, originally developed in Germany, is not reproducible in the Portuguese sample we studied. The AFE performed with the Portuguese sample suggested that the CGS presented a unifactorial structure. After the AFC, it was possible to confirm that the CGS is a valid instrument to measure suffering among formal and/or informal Portuguese-speaking caregivers (Europe). Thus, it is recommended that, in future investigations with Portuguese samples, the CGS be used as a unifactorial model. The unifactorial structure, when applied to compare formal and informal caregivers, produced results consistent with existing theoretical proposals.
In short, professionals who intend to work on assessing the extent of suffering in caregivers assisted by using the CGS, since it presents good psychometric characteristics and, therefore, will be a desirable option.

