










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
Print version ISSN 2341-4545
GE Port J Gastroenterol vol.25 no.6 Lisboa Dec. 2018
https://doi.org/10.1159/000486561
CLINICAL CASE STUDY
Increased Gastric Retention Capacity, Assessed by Scintigraphy, after APC Treatment of Dilated Gastrojejunal Anastomosis
Aumento da Capacidade de Retenção Gástrica, Medido por Cintigrafia, após Tratamento com APC de Anastomose Gastrojejunal Dilatada
Sérgio Barrichelloa, Manoel dos Passos Galvão Netob, Thiago Ferreira de Souzaa,b, Eduardo Guimarães Hourmeaux de Mouraa, Maurício Minataa, Ana Paula Oliveira de Quadrosc, Jaques Waisberga Eduardo Greccob, Guilherme Macedod, Marco Silvad, Luiz Gustavo de Quadrosa
aHospital das Clínicas de São Paulo, Medical School of the University of São Paulo (USP), São Paulo, Brazil; bABC Medical School, São Paulo, Brazil; cUniversity of the State of São Paulo (UNESP), São Paulo, Brazil; dGastroenterology Department, Centro Hospitalar de São João, Porto Medical School, Porto, Portugal
* Corresponding author.
ABSTRACT
Background: Weight regain occurs in about 20% of patients after Roux-en-Y gastric bypass (RYGB). Studies have reported that in most cases this regain is associated with dilatation of the gastrojejunal anastomosis. To correct this dilatation, one of the methods used is the application of argon plasma coagulation (APC). Case: The authors report the case of a 39-year-old woman submitted to RYGB who had weight regain. In the endoscopic evaluation, the patient presented with dilatation of the gastrojejunal anastomosis, for which treatment with APC and an adjusted diet was proposed. After 3 sessions of APC, the patient presented with a reduction of the anastomosis diameter, weight loss, and increased satiety to food, with an increased gastric emptying time evidenced by scintigraphy. Conclusion: APC proved to be a safe and efficacious method.
Keywords: Roux-en-Y gastric bypass, Gastric bypass, Obesity, Weight regain, Bariatric endoscopy
RESUMO
Introdução: O reganho de peso após bypass gástrico em Y de Roux (RYGB) ocorre em cerca de 20% dos doentes. Estudos relatam que na maioria dos casos este reganho está associado a dilatação da anastomose gastrojejunal. Para corrigir esta dilatação um dos métodos utilizados é a aplicação de árgon plasma (APC). Caso: Os autores relatam o caso de uma mulher de 39 anos de idade, submetida a RYGB, que apresentou reganho de peso. Na avaliação endoscópica a doente apresentava dilatação da anastomose gastrojejunal sendo proposta a realização de APC e dieta ajustada. Após 3 sessões de APC, a doente apresentou redução do diâmetro da anastomose associada a perda de peso, aumento da saciedade alimentar e aumento do tempo de esvaziamento gástrico documentado em cintigrafia. Conclusão: O tratamento com APC mostrou ser um método seguro e eficaz.
Palavras-Chave: Bypass gástrico em Y de Roux, Bypass gástrico, Obesidade, Reganho de peso, Endoscopia bariátrica
Introduction
Obesity is considered a worldwide epidemic. Bariatric surgery is one of the safest and most effective methods of combating obesity and its comorbidities. The most common surgical modality in Brazil and the second most common around the world is the Roux-en-Y gastric bypass (RYGB) [1].
Patients submitted to RYGB tend to have a significant weight loss. When this loss does not occur as expected or when a patient regains weight after an initial loss, a review surgery may be necessary [2]. In most cases, the cause of weight regain is dilatation of the gastrojejunal anastomosis. An alternative to corrective surgery is the use of argon plasma coagulation (APC) in several sessions with reduction of the caliber of the gastrojejunal anastomosis. The reduced size leads to a delay in gastric emptying, increasing the satiety time of the patient, and thus is conducive to weight loss. APC is a less invasive method than surgery, and when the patient is followed up by a multidisciplinary team, the results are often satisfactory.
Case Report
The authors report the case of a 39-year-old woman who was submitted to RYGB in 2003. At surgery, her weight was 119 kg (body mass index [BMI] = 45.4). For 5 years after the procedure (2003–2008), the patient had been able to maintain her target weight by following the recommended diet. She reached a minimum weight of 70 kg (BMI = 26.7), at which time further consultations were considered unnecessary.
In 2012, she again attended a doctors appointment due to weight regain. She reported progressive weight gain over the previous 4 years (2008–2012) associated with lack of satiety after eating that did not improve with dietary corrections and exercise. Blood tests did not identify any alterations in cell counts, thyroid function, or iron kinetics or vitamin deficiencies, and the patient did not present any other comorbidities. She was assessed by a psychologist, who found no disorder.
Gastric emptying scintigraphy was performed, which showed an accelerated gastric transit with retention of 42% at 30 min (reference value >70%) and 18.2% at 60 min (reference value >30%). In the absence of reference values for RYGB patients, standard reference values for normal individuals were used. Satiety was empirically evaluated after a standard solid meal: 150 g of rice, 50 g of beans, 60 g of chicken, and 2 leaves of lettuce; the patient reported satiety for only 30 min after the meal. Consequently, the patient was referred to a multidisciplinary team including a nutritionist and physiatrist, but was unable to lose weight despite a diet plan and optimized physical activity schedule.
Four years later, in 2016, after a multidisciplinary discussion of the case, the risks and benefits of endoscopic therapy and review surgery were elucidated, and the patient decided for APC sessions. In the endoscopic evaluation, she had an adequately sized stomach pouch (5 cm) with a dilated gastrojejunal anastomosis measuring 30 mm. At the time of the RYGB surgery, the gastrojejunal anastomosis was handsewn using a Fouchet catheter 12 mm in diameter.
At the first treatment session (February 2016), the patient weighed 93.5 kg. Argon was applied around the entire circumference of the anastomosis and to approximately 1.5 cm of the proximal gastric mucosa (power: 70 W; flow: 2.0 L/min). After the procedure, the patient was prescribed a restricted liquid diet for 1 week, after which she resumed a standard solid diet. The patient reported feeling satiated for 1 h after consuming her first solid meal.
Eight weeks later (April 2016), APC was performed again. The patient weighed 79.5 kg and the anastomosis was 21 mm in diameter. The procedure was performed according to the same settings as the first session, and the patient was again prescribed a restricted liquid diet for 1 week. She reported feeling satiety for 2 h after her first solid meal after the second session.
The last APC session took place 8 weeks later (June 2016). The patient weighed 72.5 kg, the surgical pouch was 4 cm, and the anastomosis was 14 mm in diameter. APC was applied around the entire circumference of the anastomosis and extended to about 0.5 cm of the proximal mucosa.
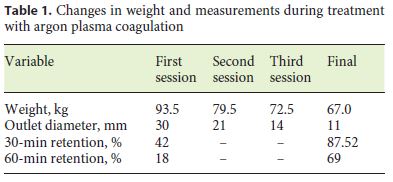
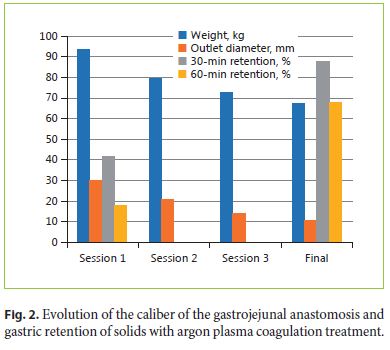
One month after the last procedure, the patient weighed 67 kg and she reported satiety for 2.5 h after solid meals. On endoscopic evaluation, the stomach pouch measured 4 cm and the anastomosis was 11 mm in diameter. A solid retention scintigraphy study was performed, showing gastric transit with retention of 87.5% at 30 min and 69% at 60 min. Table 1 describes the variations in weight and main measurements throughout treatment.
Discussion
Bariatric surgery, the most effective method of combating obesity, is associated with a reduction of associated comorbidities and prolonged patient life [1]. There are several possible surgical techniques, with RYGB, one of the most common techniques, producing excellent results. However, some patients have short- or long-term complications. These complications must be treated by a multidisciplinary team, with endoscopic evaluations playing a fundamental role [3]. Up to 20% of the patients submitted to treatment tend to have weight regain 5–10 years after the surgical procedure [4]. The causes of this weight regain are numerous, but they include metabolic dysfunctions, relaxed diets, a sedentary lifestyle, hormonal changes, fistulas, a large stomach pouch, and dilatation of the gastrojejunal anastomosis [3–6]. In fact, dilatation of the gastrointestinal anastomosis is one of the most common causes [7, 8].
Abu Dayyeh et al. [9] performed a study that directly correlated the size of the perimeter of a gastrojejunal anastomosis to weight regain in a series of patients who were followed up for 4 years after RYGB. The authors suggested that dilatation of the anastomosis should be evaluated as a predictor of weight regain. A recent meta-analysis also concluded that dilatation of the gastrojejunal anastomosis was associated with postsurgical weight regain [5].
Several surgical and nonsurgical procedures have been implemented to treat patients with dilatation of the anastomosis [10]. Spaulding [11] proposed sclerotherapy injections into the muscular wall of the anastomosis to reduce its diameter. More than 1 treatment session was required for the majority of patients evaluated, and the results were modest [11]. Some endoluminal procedures have also been developed, with good results but using high-cost platforms [12]. Kumar and Thompson [6] carried out a study on patients with weight regain after RYGB in whom the anastomosis was greater than 15 mm in diameter. The patients underwent an endoscopic suturing procedure to reduce the diameter of the anastomosis. After the procedure, the patients safely and efficaciously returned to their desired weight.
An alternative endoscopic treatment is the application of APC on the tissue bordering the gastrojejunal anastomosis to cause retraction of the dilatation. APC is a noncontact photocoagulation method endoscopically applied to tissue after sedation in an outpatient setting [13]. In 2009, Aly [14] reported a case of APC in a patient with weight regain after RYGB that produced satisfactory results and concluded that this technique is effective and safe. Baretta et al. [4] evaluated the safety and efficacy of APC in a study that included 30 patients with weight regain after RYGB who had dilatation of the gastrojejunal anastomosis. Each patient underwent 3 sessions of APC at 8-week intervals. A reduction by approximately 67% in the diameter of the anastomosis was observed in the final evaluation, as were reductions in weight and BMI; the complication rate was low. Another study conducted on 10 patients (70% female) with a mean age of 56 years and a mean weight of 133.4 kg evaluated weight loss, caloric intake, and satiety after 1 session of APC. This study proved that the application of APC was effective in increasing satiety time, reducing caloric intake, and reducing weight in patients [15].
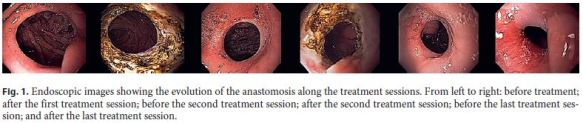
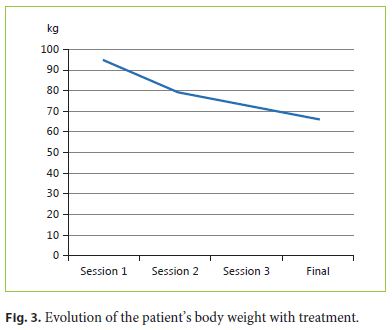
To the authors best knowledge, this is the first case reported in the literature correlating reduction of the gastric anastomosis using APC (Fig. 1) with an increase in the scintigraphic gastric emptying time (Fig. 2), weight loss, and a prolonged feeling of postprandial satiety. In fact, this method resulted in increases of 108 and 283% in the gastric retention capacity of solids 30 and 60 min after ingestion, respectively. The application of APC in conjunction with an adequate dietary plan led to a rapid and effective loss of the patients regained weight, i.e., 26.5 kg (28.3% of the total body weight of the patient) in 7 months of follow-up, even reducing it below the minimum weight achieved after RYGB (70 kg) (Fig. 3). The authors report this case in order to highlight the efficacy and safety of this widely accessible and easy-to-execute method. The increased gastric retention of solids, as seen by scintigraphy, explains the prolongation of the sensation of postprandial satiety and most probably contributes to a better adherence of the patient to her dietary plan and to the excellent results described with this technique.
References
1 Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, Schoelles K: Bariatric surgery: a systematic review and metaanalysis. JAMA 2004;292:1724–1737. [ Links ]
2 Parikh M, Pomp A, Gagner M: Laparoscopic conversion of failed gastric bypass to duodenal switch: technical considerations and preliminary outcomes. Surg Obes Relat Dis 2007;3:611–618. [ Links ]
3 Quadros LG, Kaiser RL Junior, Galvão MD Neto, Campos JM, Santana MF, Ferraz AA: Long-term postoperative endoscopic findings after gastric bypass procedure: a co-occurrence analysis. Arq Gastroenterol 2016;53:273–277. [ Links ]
4 Baretta GA, Alhinho HC, Matias JE, Marchesini JB, de Lima JH, Empinotti C, Campos JM: Argon plasma coagulation of gastrojejunal anastomosis for weight regain after gastric bypass. Obes Surg 2015;25:72–79. [ Links ]
5 Vargas EJ, Bazerbachi F, Rizk M, Rustagi T, Acosta A, Wilson EB, Neto MG, Zundel N, Mundi MS, Collazo-Clavell ML, Meera S, Abu-Lebdeh HS, Lorentz PA, Grothe KB, Clark MM, Kellogg TA, McKenzie TJ, Kendrick ML, Topazian MD, Gostout CJ, Abu Dayyeh BK: Transoral outlet reduction with full thickness endoscopic suturing for weight regain after gastric bypass: a large multicenter international experience and meta-analysis. Surg Endosc 2018;32:252–259.
6 Kumar N, Thompson CC: Transoral outlet reduction for weight regain after gastric bypass: long-term follow-up. Gastrointest Endosc 2016;83:776–779. [ Links ]
7 Thompson CC, Jacobsen GR, Schroder GL, Horgan S: Stoma size critical to 12-month outcomes in endoscopic suturing for gastric bypass repair. Surg Obes Relat Dis 2012;8:282–287. [ Links ]
8 Heneghan HM, Yimcharoen P, Brethauer SA, Kroh M, Chand B: Influence of pouch and stoma size on weight loss after gastric bypass. Surg Obes Relat Dis 2012;8:408–415. [ Links ]
9 Abu Dayyeh BK, Lautz DB, Thompson CC: Gastrojejunal stoma diameter predicts weight regain after Roux-en-Y gastric bypass. Clin Gastroenterol Hepatol 2011;9:228–233. [ Links ]
10 Bessler M, Daud A, DiGiorgi MF, OliveroRivera L, Davis D: Adjustable gastric banding as a revisional bariatric procedure after failed gastric bypass. Obes Surg 2005;15:1443–1448. [ Links ]
11 Spaulding L: Treatment of dilated gastrojejunostomy with sclerotherapy. Obes Surg 2003;13:254–257. [ Links ]
12 Horgan S, Jacobsen G, Weiss GD, Oldham JS Jr, Denk PM, Borao F, Gorcey S, Watkins B, Mobley J, Thompson K, Spivack A, Voellinger D, Thompson C, Swanstrom L, Shah P, Haber G, Brengman M, Schroder G: Incisionless revision of post-Roux-en-Y bypass stomal and pouch dilation: multicenter registry results. Surg Obes Relat Dis 2010;6:290–295. [ Links ]
13 Zenker M: Argon plasma coagulation. GMS Krankenhhyg Interdiszip 2008;3:Doc15. [ Links ]
14 Aly A: Argon plasma coagulation and gastric bypass – a novel solution to stomal dilation. Obes Surg 2009;19:788–790. [ Links ]
15 Souza TF, Marques LM, Santos FP, Nunes G, Barrichello S, Grecco E, Neto M: Therapeutic with argon plasma coagulation in Roux-en-Y anastomosis for weight regain after bariatric surgery: case series. Gastrointest Endosc 2016;83:AB512. [ Links ]
Statement of Ethics
All rules of the local ethics committee (Hospital das Clínicas de São Paulo, Medical School of the University of São Paulo [USP]) were followed, safeguarding the patients identity and confidentiality. The paper was written according to CARE guidelines.
Disclosure Statement
The authors declare that they have no conflict of interest.
* Corresponding author.
Dr. Luiz Gustavo de Quadros
Kaiser Clínica
Rua XV de Novembro no 3975
15015-110 São José do Rio Preto (Brazil)
E-Mail gustavo_quadros@hotmail.com
Received: November 7, 2017; Accepted after revision: January 2, 2018
Author Contributions
Sérgio Barrichello: endoscopic examination, drafting of the manuscript; Manoel dos Passos Galvão Neto: endoscopic examination, critical revision; Thiago Ferreira de Souza: endoscopic examination, drafting of the manuscript; Eduardo Guimarães Hourmeaux de Moura: data collection; Maurício Minata: data collection; Ana Paula Oliveira de Quadros: drafting of the manuscript; Jaques Waisberg: endoscopic examination, critical revision of the manuscript; Eduardo Grecco: critical revision of the manuscript; Guilherme Macedo: critical revision of the manuscript; Marco Silva: data collection, drafting of the manuscript; Luíz Gustavo de Quadros: drafting of the manuscript, final approval of the manuscript.

