










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versión impresa ISSN 2341-4545
GE Port J Gastroenterol vol.26 no.4 Lisboa ago. 2019
https://doi.org/10.1159/000493438
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
Inflammatory Pseudotumor of the Liver: Clinical Case
Pseudotumor inflamatório do fígado: caso clínico
Cristina Lameirão Gomes, Nuno Silva, José Presa Ramos
Liver Unit, Internal Medicine Department, Centro Hospitalar de Trás-os-Montes e Alto Douro, Vila Real, Portugal
* Corresponding author.
Keywords: Inflammatory pseudotumor of the liver, Liver biopsy, Nonsteroidal anti-inflammatory drugs
Palavras-Chave: Pseudotumor inflamatório do fígado, Biópsia hepática, Anti-inflamatórios não esteroides
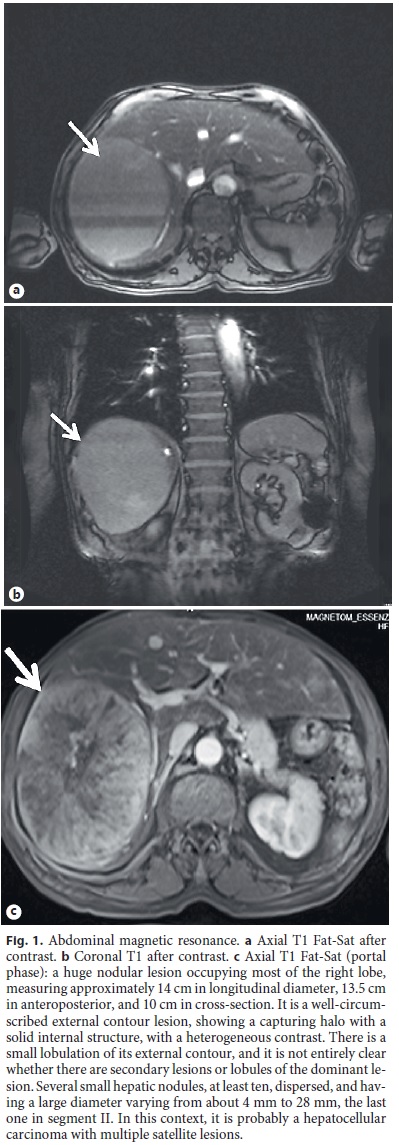
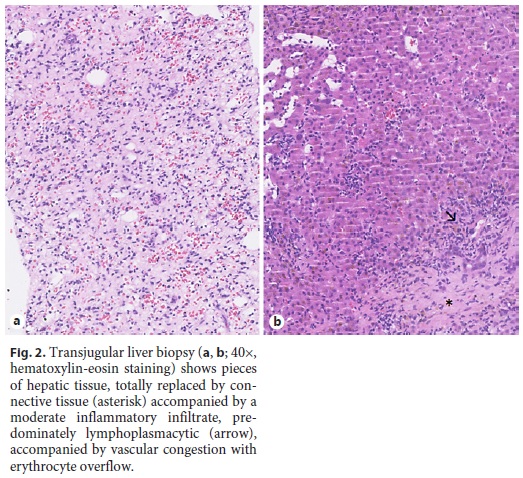
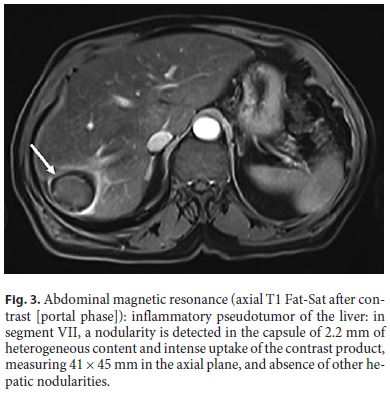
The authors present the case of an 81-year-old man with hypertension and alcohol consumption (60–80 g/ day) who was admitted to the Emergency Department with abdominal pain in the upper right quadrant, with 1 month of evolution, diarrhea (5–6 liquid stools per day), and slimming of 10 kg in the past 2 months. He had no fever or stigmas of alcoholic liver disease. Analytically, he had no increase in inflammatory markers, but because of these complaints, an abdominal computed tomography was performed, which showed a bulky mass. The mass occupied almost the whole right lobe of the liver, measured 14.5 cm of greater axis, and had well-defined contours and signs of intralesional necrosis at the central level. The patient was referred to the Ambulatory Liver Unit. In the first evaluation, a hard mass in the upper right quadrant was detected, with well-defined limits and slightly painful to deep palpation. In the etiological study, we highlight: hemoglobin 9.27 g/dL (normal: 13–18), mean corpuscular volume 109 fL (normal: 87–103), mean corpuscular hemoglobin (HGM) 35.3 pg (normal: 27–33), leukocytes 5,000/μL (normal: 4,000–11,000), platelets 377,000/μL (normal: 150,000–400,000), aspartate aminotransferase 33 U/L (normal: < 40), alanine aminotransferase 23 U/L (normal: < 41), gamma-glutamyltransferase 96 U/L (normal: 10–49), total bilirubin 0.6 mg/dL (normal: < 1.2), albumin 3.6 g/dL (normal: 3.4– 4.8), alkaline phosphatase 99 U/L (normal: 40–130), Creactive protein 0.6 mg/dL (normal: < 0.5), normal coagulation, renal function, and ionogram, negative viral serology (hepatitis B virus, hepatitis C virus, and human immunodeficiency virus), tumor markers: alpha-fetoprotein 2.2 IU/mL (normal: 1–8), carcinoembryonic antigen 2.3 ng/mL (normal: < 0.5), and CA19.9 77 U/mL (normal: 0–37). In order to better characterize the nodule, abdominal magnetic resonance imaging was performed, which described a well-circumscribed contour lesion, showing a halo with a solid internal structure with heterogenous contrast uptake, which was interpreted as a probable hepatocellular carcinoma with several satellite lesions; the suprahepatic veins, the portal vein, and the hepatic artery remain permeable, with no other changes (Fig. 1). A liver biopsy was performed, which revealed histologic pattern of an inflammatory pseudotumor of the liver (IPT) (Fig. 2). He started nonsteroidal anti-inflammatory drugs (naproxen 500 mg/day), and about 1 year after starting the treatment, he was asymptomatic. He repeated imaging 1.5 years afterwards, which revealed a significant reduction of the hepatic lesion, currently measuring 41 × 45 mm (Fig. 3). He maintained treatment for 2 years and trimestral follow-up in the Ambulatory Liver Unit.
IPT is a rare benign lesion with only about 300 cases described in the literature [1]. It predominantly affects children and young adults (predominance of the 3rd decade), but can occur at any age, being more frequent in the Asian population, predominantly in males [2, 3]. The etiology and pathogenesis remain unknown, but it is assumed that it may result from an exaggerated inflammatory response directed to a particular aggression (inflammatory, infectious, autoimmune, trauma, or surgical processes) [2, 4]. IPT can appear as a single mass or multiple masses characterized histologically by the proliferation of fibroblasts and inflammatory cells [4, 5]. Diagnosis of IPT is challenging, because there are no clinical symptoms, signs, or laboratory or pathognomonic imaging of this pathology, often leading to an incorrect diagnosis [2]. Liver biopsy is necessary to establish a definitive diagnosis [2, 3, 5]. Treatment can be done with antibiotics, nonsteroidal anti-inflammatory drugs, steroids, or just an expectant attitude [2, 5]. Surgical resection is not usually recommended [2]. In general, the prognosis is good [2, 3].
References
1 Yang X, Zhu J, Biskup E, Cai F, Li A. Inflammatory pseudotumors of the liver: experience of 114 cases. Tumour Biol. 2015 Jul;36(7):5143–8. [ Links ]
2 Soares M, Honovar M, Pimentel Barbosa J. Pseudotumor inflamatório do fígado: o imitador bom das neoplasias hepáticas. Galicia Clin. 2014;75(1):36–8. [ Links ]
3 Park JY, Choi MS, Lim YS, Park JW, Kim SU, Min YW, et al. Clinical features, image findings, and prognosis of inflammatory pseudotumor of the liver: a multicenter experience of 45 cases. Gut Liver. 2014 Jan;8(1):58–63. [ Links ]
4 Patnana M, Sevrukov AB, Elsayes KM, Viswanathan C, Lubner M, Menias CO. Inflammatory pseudotumor: the great mimicker. AJR Am J Roentgenol. 2012 Mar;198(3):W217–27. [ Links ]
5 Conceição JS, Santos AM, Júnior LEF, Braga HJV, Silva LR. Pseudotumor inflamatório do fígado – um diagnóstico diferencial raro de massa hepática. GED Gastroenterol Endosc Dig. 2012;31:102–106. [ Links ]
Statement of Ethics
This study did not require informed consent nor review/approval by the appropriate ethics committee.
Disclosure Statement
The authors declare no conflicts of interest.
* Corresponding author.
Cristina Lameirão Gomes
Centro Hospitalar de Trás-os-Montes e Alto Douro
Av. Da Noruega, Lordelo
PT–5000-508 Vila Real (Portugal)
E-Mail cristinasofiagomes@hotmail.com
Received: May 24, 2018; Accepted after revision: September 2, 2018

